1668
Impact of isometric hand-grip exercise (IHE) on metrics of diastolic function by MRI1Yale University, New Haven, CT, United States, 2Department of Radiology and Biomedical Imaging, Yale University, New Haven, CT, United States
Synopsis
Keywords: Flow, Cardiovascular, Exercise, diastolic function
Motivation: Exercise testing is important in evaluation of diastolic dysfunction but there is little use of exercise for diagnosis.
Goal(s): Test if MR phase-contrast and cine techniques can identify changes in E, A, and e’ with hand-grip exercise.
Approach: Five healthy subjects underwent diastolic function evaluation by MRI, during isometric handgrip exercise. E, A and e’ were evaluated.
Results: In this group, E/A decreased with exercise, and recovered after a period of rest. Isometric handgrip exercise is promising approach for revealing diastolic dysfunction in patients.
Impact: Isometric hand-grip exercise may be a useful tool in exercise cardiac MRI for diagnosis in patients with heart failure with preserved ejection fraction.
Introduction
While exercise testing is used for diagnosis of ischemia, there is little use of exercise for diagnosis in patients with heart failure with preserved EF. This might be important, because at rest the heart may be compensated, with normal EF, cardiac output, and LV filling pressure, while during increased oxygen demand, patients might develop symptoms when LV filling pressure is increased (1). In response to exercise, healthy subjects can increase LV filling flow by lowering LV minimum pressure, but for subjects with diastolic dysfunction or HFpEF, flow is increased by increasing left atrial pressure causing subsequent pulmonary congestion (2). In healthy subjects, E/e’ (a surrogate of pressure) is not expected to increase with exercise, while for patients E/e’ may increase. Isometric hand-grip exercise (IHE), one of the earliest exercise methods used in MRI (3). IHE reproducibly increases LV afterload and myocardial oxygen demand (4). IHE provokes changes in HFpEF patients diastolic parameters (E/e’ by TTE) similar to bicycle exercise (4). IHE is used during invasive evaluation of LV filling pressure (5), where pressure has been measured to increase by 30% in response to handgrip exercise. IHE is very suitable for MRI, because motion artifacts associated with other forms of exercise in the bore are not generated; it is also inexpensive and accessible. Our hypothesis is the MR phase-contrast and cine techniques can identify changes in E, A, and e’ with hand-grip exercise. In an echocardiography study (4) using hand grip exercise in healthy young subjects, no change in E or A were observed, a very small increase in E/e’ was found, but there was a decrease in E/A (2.2 decreasing to 1.4 at exercise).Methods
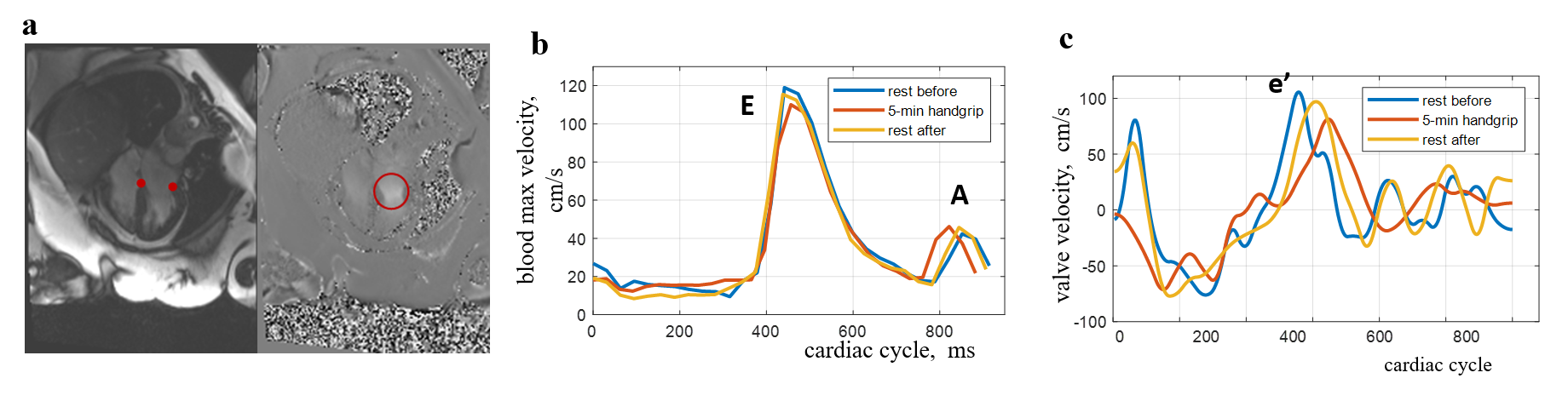
We studied five healthy volunteers with hand grip exercise (age=39 ±21, 3 females). The protocol and equipment are shown in Figure 1. Handexer hand-grip equipment was used to measure maximal hand grip strength. After MRI at rest, the volunteers were asked to performed isometric hand grip exercise in the magnet for 5 minutes, using 40% of measured maximal hand grip strength, similar to other protocols. Subjects were imaged to measure E, A, and e’, using the methods described below, while performing IHE. After imaging, subjects were asked to rest for five minutes, and then the MRI protocol was repeated. All subjects provided written informed consent. MR imaging: Healthy controls were imaged on a 3T Siemens with a 4 chamber (4ch) cine, and 4ch cine PC using in-plane flow-encoding in the LV long-axis direction (Figure 1). Scan parameters for the long-axis cines (4ch) were retrospectively ECG-gated bSSFP, TR/TE/ q =2.4ms/1.2ms/45°, 36ms temporal resolution, 8mm slice, 208 x168 matrix, 320x320cm FOV (1.5x1.9 mm2 in-plane resolution). The long-axis 4ch PC sequence used in-plane velocity encoding, parallel to the long-axis with a VENC of 150 cm/s. Scan parameters were: 2D GRE breath-hold, retrospective ECG gating, TR/TE/q = 5.9ms/2.5ms/20°, temporal resolution of 36ms, 192x115 matrix, 380x278mm FOV (2.0x2.4 mm2 in-plane resolution), 6-8mm slice thickness. A 4-ch balanced SSFP PC approach was also performed (6), with scan parameters similar to the conventional PC, except with TR/TE/ q =4ms/2.0ms/45°. The PC-SSFP method measures E, A and e’ in a single scan.Results
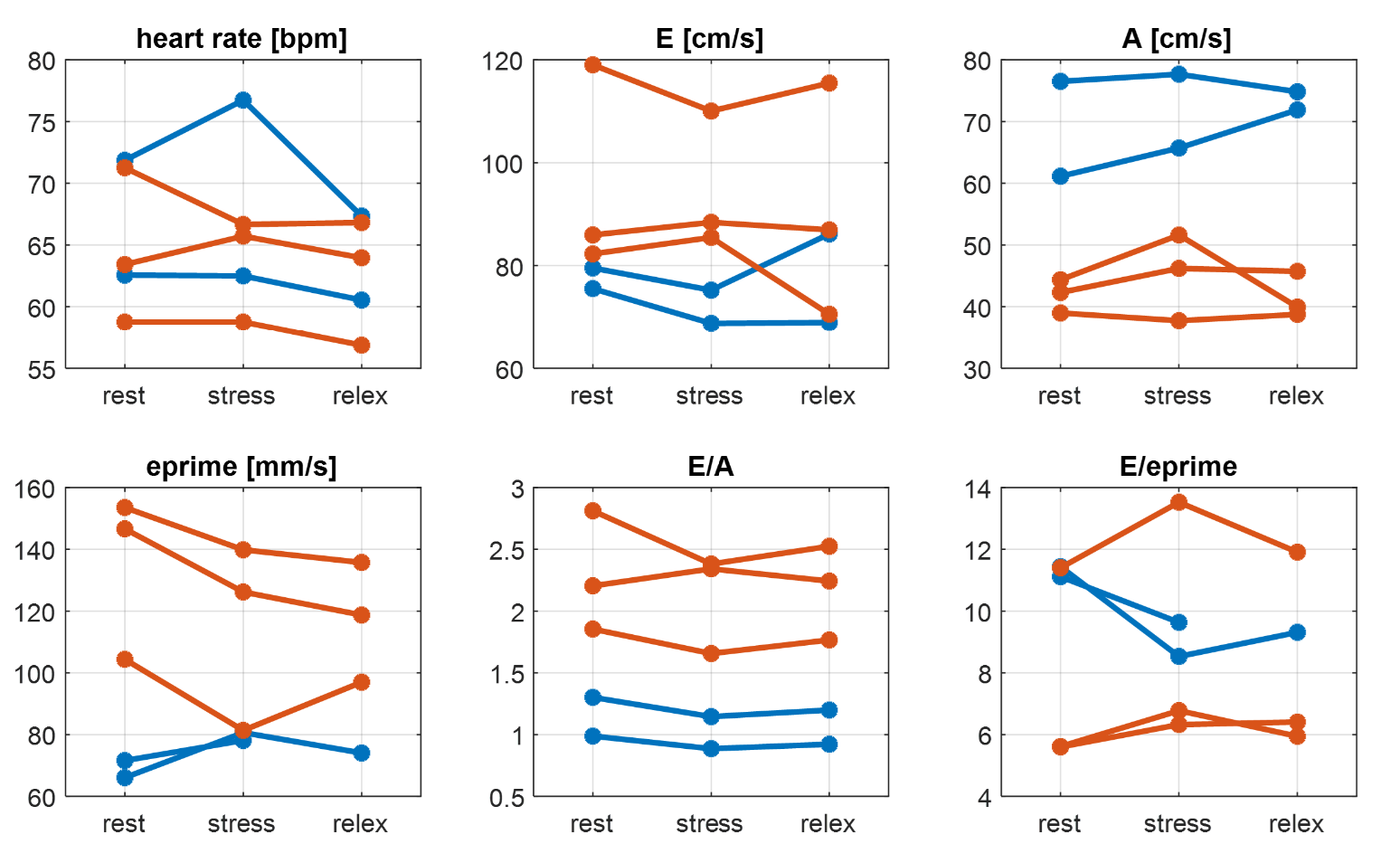
No subjects reported difficulty with IHE, except for minor hand discomfort in one. Figure 2 shows an example of changes in E, A and e’, during the three stages of rest and exercise, based on PC-SSFP data. Figure 3 presents the data for 5 healthy subjects. We measured a small but consistent increase in heart-rate at 5 minutes after hand grip exercise. In most subjects (4 of 5), E/A decreased with exercise (1.8± 0.7 vs. 1.7±0.7, p=0.09 by paired t-test), and then recovered during rest. However, we did not find consistent changes in E/e’, which seemed to increase slightly in younger subjects (expected) and decrease slightly in older subjects.Discussion
Although this a simple exercise test, we found reproducible results and an expected decrease in E/A, indicating that as afterload and oxygen demand increase, if the early filling (E wave) is not sufficiently increased, atrial filling (A wave) can compensate. PC-SSFP, as an all-in-one diastology scan, might be useful in this exercise protocol. This study shows that IHE may be a useful tool in exercise cardiac MRI, although a larger cohort is needed, and other exercise protocols could be tested.Acknowledgements
No acknowledgement found.References
1. Ha JW, Andersen OS, Smiseth OA.
Diastolic Stress Test: Invasive and Noninvasive Testing. JACC Cardiovasc
Imaging 2020;13(1 Pt 2):272-282.
2. Mitter SS, Shah SJ, Thomas JD. A
Test in Context: E/A and E/e' to Assess Diastolic Dysfunction and LV Filling
Pressure. J Am Coll Cardiol 2017;69(11):1451-1464.
3. Weiss RG, Bottomley PA, Hardy CJ, Gerstenblith G. Regional myocardial metabolism of high-energy phosphates during isometric exercise in patients with coronary artery disease. N Engl J Med 1990;323(23):1593-1600.
4. Jake Samuel T, Beaudry R, Haykowsky MJ, et al. Isometric handgrip echocardiography: A noninvasive stress test to assess left ventricular diastolic function. Clinical cardiology 2017;40(12):1247-1255. 5. Penicka M, Bartunek J, Trakalova H, et al. Heart failure with preserved ejection fraction in outpatients with unexplained dyspnea: a pressure-volume loop analysis. J Am Coll Cardiol 2010;55(16):1701-1710.
6. Xiang J, Lamy J, Galiana G, Peters D. K-t PCA Accelerated In-Plane Balanced Steady-State Free Precession Phase-Contrast (PC-SSFP) for All-in-One Diastolic Function Evaluation. Magn Reson Med 2023.
Figures