1665
Short-term Performance of Single Bolus r-SAK Prior to PCI in ST-Segment Elevation Myocardial Infarction by Cardiac Magnetic Resonance Imaging1Department of Radiology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Atherosclerosis, Heart
Motivation: Compared with primary percutaneous coronary intervention (PPCI), it is not known whether patients with ST-elevation myocardial infarction (STEMI) benefit from thrombolysis prior to PCI within 120 minutes of symptom onset.
Goal(s): This study was to compare the short-term performance between STEMI patients with and without a single bolus recombinant staphylokinase (r-SAK) prior to PCI by Cardiac Magnetic Resonance (CMR) imaging.
Approach: The global and segmental [mainly focusing on LGE+ segment (transmural extent >50%)] CMR parameters were compared between r-SAK group and control group.
Results: Patients can benefit from thrombolysis prior to PCI with better myocardial function and smaller extent of edema.
Impact: This study investigated the short-term advantages of adjunctive thrombolysis with r-SAK for STEMI patients undergoing PCI. A single bolus r-SAK intravenously prior to PCI for STEMI improves myocardial function and reduces the extent of edema.
Introduction
Compared with primary percutaneous coronary intervention (PPCI), it is not known whether patients with ST-elevation myocardial infarction (STEMI) gain benefit from adjunctive thrombolysis prior to PCI within 120 minutes of symptom onset1-3. This study was to compare the short-term performance between STEMI patients with or without a single bolus recombinant staphylokinase (r-SAK) prior to PCI by Cardiac Magnetic Resonance (CMR) imaging.Method
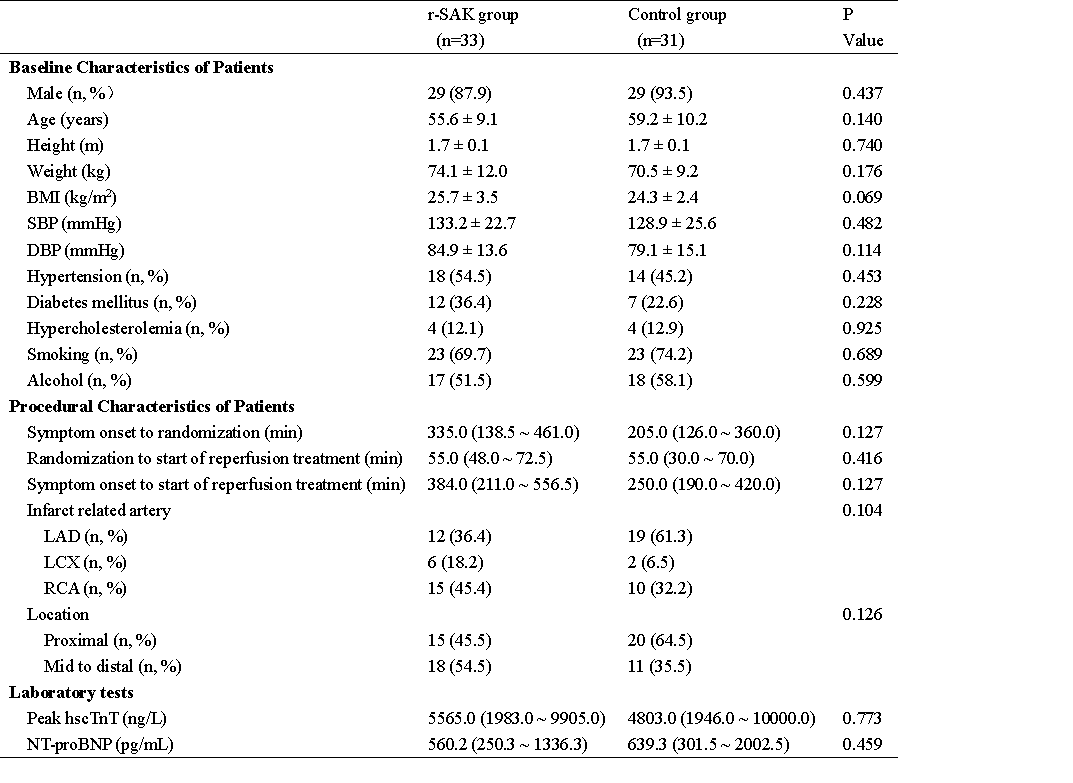
A total of 64 patients with acute STEMI were retrospectively recruited for CMR, 33 patients were from r-SAK group and 31 patients from control group. Scans were performed on a 3-T MRI system (Ingenia CX, Philips Healthcare). The global and segmental [mainly focusing on LGE+ segment (transmural extent >50%)] CMR parameters were compared between r-SAK group and control group.Results
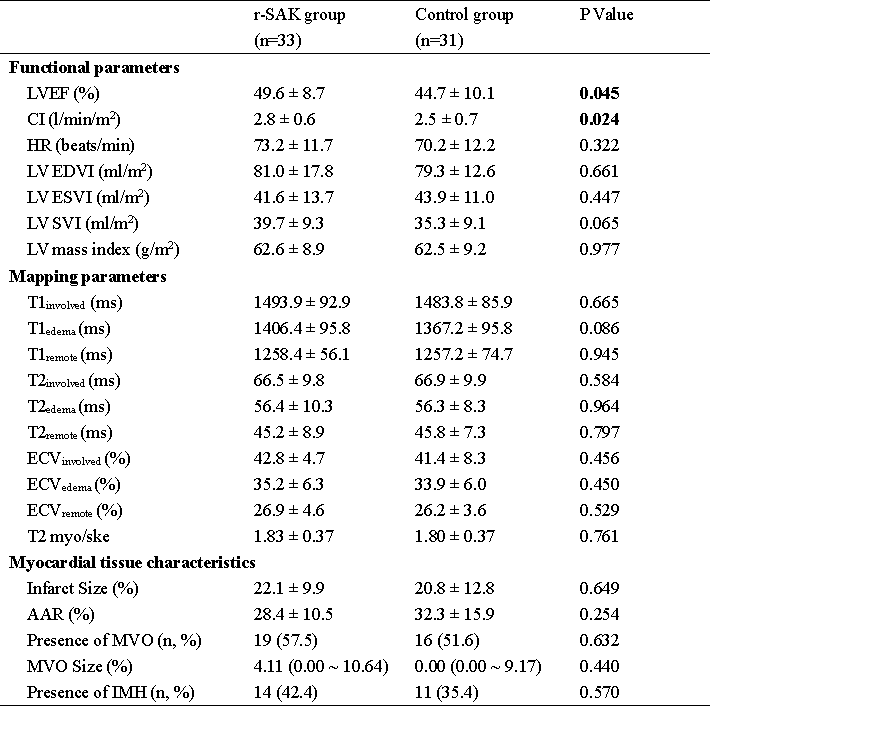
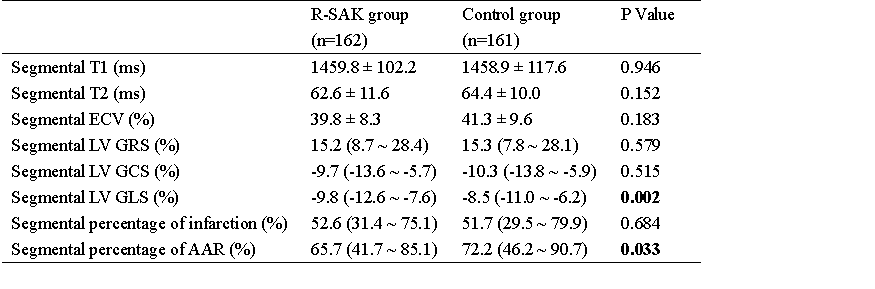
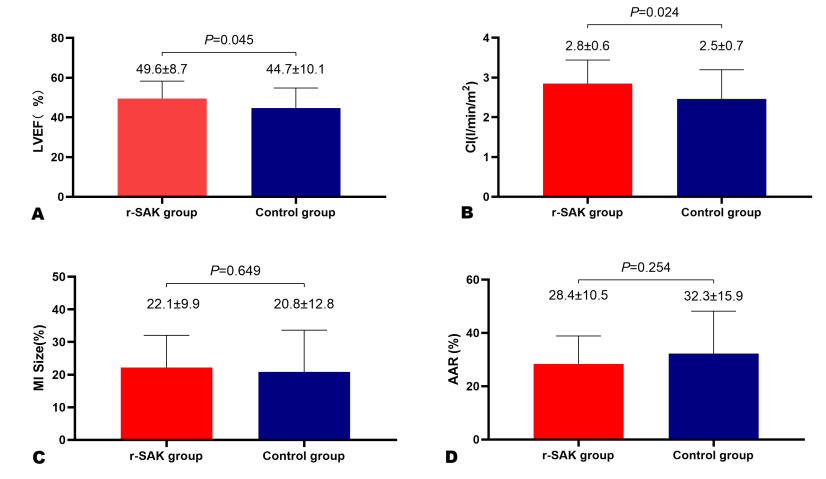
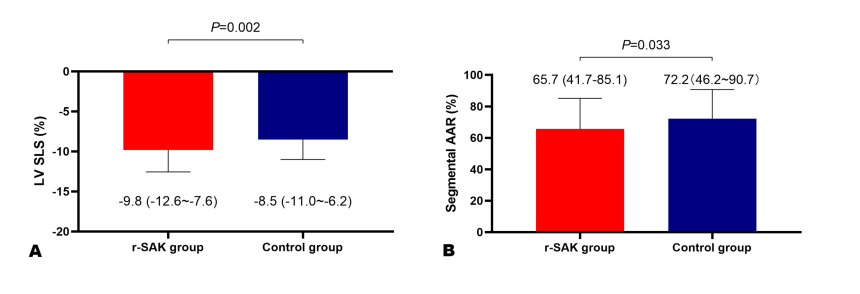
The CMR scan was performed a average of 5.2 ± 1.1 days after reperfusion. There were no significant differences in baseline and procedural characteristics and laboratory tests between r-SAK group and control group. Compared with those from control group, patients from r-SAK group had higher left ventricular ejection fraction (LVEF) and cardiac output index (CI) (49.6 ± 8.7% vs. 44.7 ± 10.1%, P = 0.045; 2.8 ± 0.6 vs. 2.5 ± 0.7, P =0.024).There was no significant difference between two groups in global infarct size (IS) (22.1 ± 9.9% vs. 20.8 ± 12.8%, P =0.649), global area at risk (AAR) (28.4 ± 10.5% vs. 32.3 ± 15.9%, P =0.254) or presence of microvascular obstruction (MVO) (57.5% vs. 51.6%, P =0.632) and intramuscular hemorrhage (IMH) (42.4% vs. 35.4%, P =0.570). When it comes to LGE+ segment (trans-mural extent >50%), the better LV segmental longitudinal strain (SLS) [-9.8 (interquartile range, -12.6 to -7.6) vs. -8.5 (interquartile range, -11.0 to -6.2); P = 0.002] and the smaller segmental AAR size [65.7% (interquartile range, 41.7% to 85.1%) vs.72.2% (interquartile range, 46.2% to 90.7%); P = 0.033] was observed in r-SAK group compared with control group.Discussion
Higher presence of IMH was not observed in the patients from r-SAK group, which suggested that a single bolus r-SAK prior to PCI didn’t increase the risk of myocardial hemorrhage. Moreover, a higher LVEF and CI was found in the patients with early thrombolysis. From regional perspectives, patients from r-SAK group also had a better LV SLS. Thus, early thrombolysis may result in less impairment in myocardial function at early stage after reperfusion. In LGE+ segments, compared with patients in control group, those in r-SAK group had smaller extent of edema. This indicated that earlier restoration of perfusion before PCI may restrict the extent of myocardial edema in the short-term postoperative period.While a small cohort of patients limited the applicability of this study. In addition, the long-term performance was needed to be investigated.Conclusion
A single bolus r-SAK prior to primary PCI for STEMI does not increase the risk of IMH. In addition, patients can benefit from adjunctive thrombolysis prior to PCI with better global and regional myocardial function and smaller extent of edema. Early thrombolysis results in less impairment in myocardial function and restrict the extent of myocardial edema in the short-term postoperative period.Acknowledgements
I would first like to thank Yi Xu and Xiaomei Zhu, whose expertise was invaluable in formulating the research questions and methodology.
I also thank all the investigators, and participating staff members in this study.
References
1. De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation. 2004;109:1223-1225. doi: 10.1161/01.CIR.0000121424.76486.20
2. Ellis SG, Tendera M, de Belder MA, van Boven AJ, Widimsky P, Janssens L, Andersen HR, Betriu A, Savonitto S, Adamus J, et al. Facilitated PCI in patients with ST-elevation myocardial infarction. The New England journal of medicine. 2008;358:2205-2217. doi: 10.1056/NEJMoa0706816
3. Armstrong PW, Gershlick AH, Goldstein P, Wilcox R, Danays T, Lambert Y, Sulimov V, Rosell Ortiz F, Ostojic M, Welsh RC, et al. Fibrinolysis or primary PCI in ST-segment elevation myocardial infarction. N Engl J Med. 2013;368:1379-1387. doi: 10.1056/NEJMoa1301092
Figures