1662
Cardiovascular assessment of diastolic dysfunction in people living with the HIV: correlation with markers of disease activity1The First Affiliated Hospital of China Medical University, Shenyang, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: People living with HIV are at increased risk of cardiovascular disease compared with healthy people.
Goal(s): To explore the extent of diastolic atrial and left ventricular dysfunction in PLWH by CMR in correlation with clinical markers of disease activity.
Approach: 101 PLWH and 62 healthy volunteers were recruited for this study in China. Both left atrial (LA) and LV strain and strain rate were calculated using CMR feature tracking.
Results: PLWH had a larger LAVImax, LAVImin and LAVIpre-a as compared to healthy volunteers. The LA
reservoir, conduit and booster pump function were all impaired in PLWH.
Impact: The prevalence of diastolic dysfunction as well as asymptomatic systolicabnormalities is observed in HIV patients.
Introduction
People living with HIV (PLWH) are at increased risk of cardiovascular disease compared with healthy people(1). However, the pathophysiology of HIV-associated cardiomyopathy remains uncertain and is likely multifactorial. The proposed causes include direct infection of the myocardium by the HIV-1 virus with or without myocarditis, immune mechanisms, toxicity from the medications used to treat HIV-1 infection, and opportunistic infections. Nowadays a high prevalence of diastolic abnormalities as well as asymptomatic systolic dysfunction is observed in HIV patients that may lead to higher mortality. Accordingly, assessment of early markers of diastolic dysfunction are important for risk stratification and detecting incipient heart failure in HIV patients.Among people without HIV, left atrial (LA) volumetric analysis by imaging techniques is well suited to assess the cumulative effect of diastolic dysfunction (2).Strain and strain rate are more sensitive markers of diastolic dysfunction (3). Thus, analysis of the LA volumetric parameters as well as atrial and ventricular diastolic are sensitive markers of diastolic dysfunction.
CMR allows accurate strain evaluation of the left atrium as well as the left ventricle owing to its high spatial resolution, larger field of view, and high reproducibility Nadir CD4+T-cell counts decrease with longer times since HIV-1diagnosis an reflect the extent of HIV-1 induced immune damage as a marker of excess mortality, systemic inflammation and clinical complications in chronicallyHIV-1 infected persons.
Accordingly, the purpose of this study was to explore the presence and extent of atrial and ventricular diastolic dysfunction by CMR in PLWH as compared to healthy people, and to explore whether HIV clinical markers and risk factors are associated with the CMR parameters.
Methods
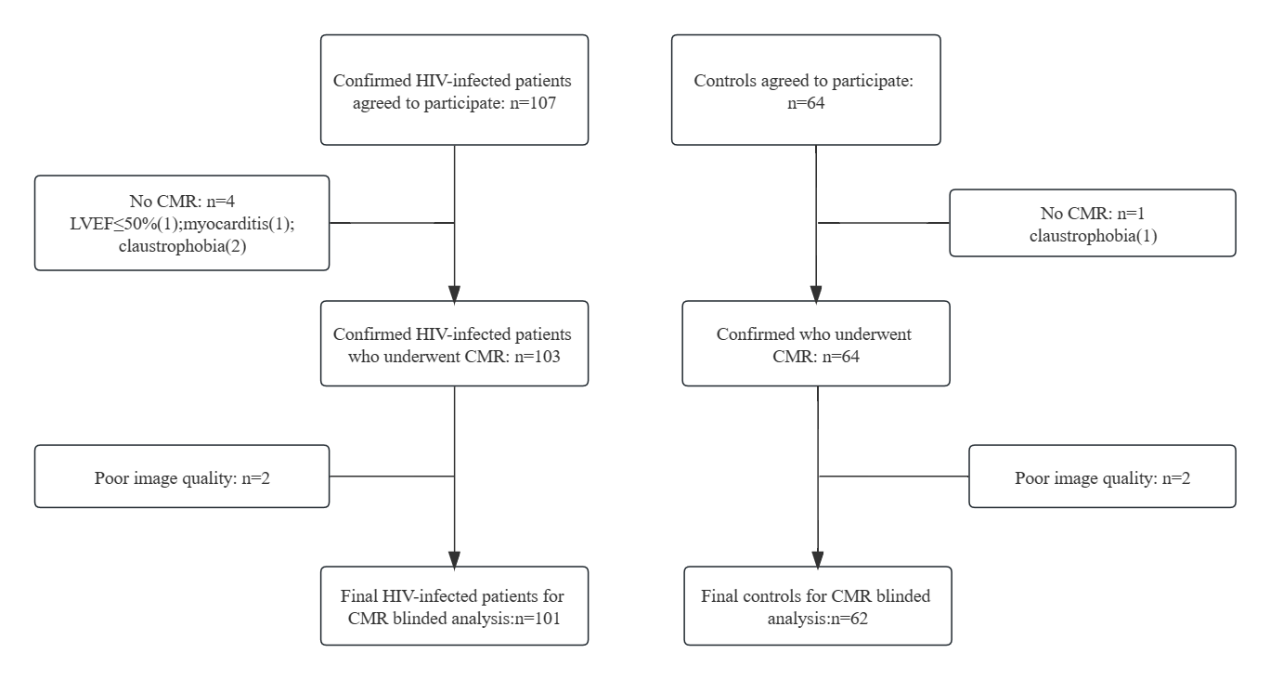
A total of 163 participants (50 ±10 years, 87.1% men) comprising 101PLWH and 62 age- and sex-matched healthy volunteers were recruited for this cross-sectional study in China. Both left atrial (LA) and LV strain and strain rate were calculated using CMR feature tracking. Data were analyzed using the software package SPSS Statistics Version 26.0. The used tests included independent t test and Univariate and multivariate linear or logistic analyses (significance level: P value<0.05).Results
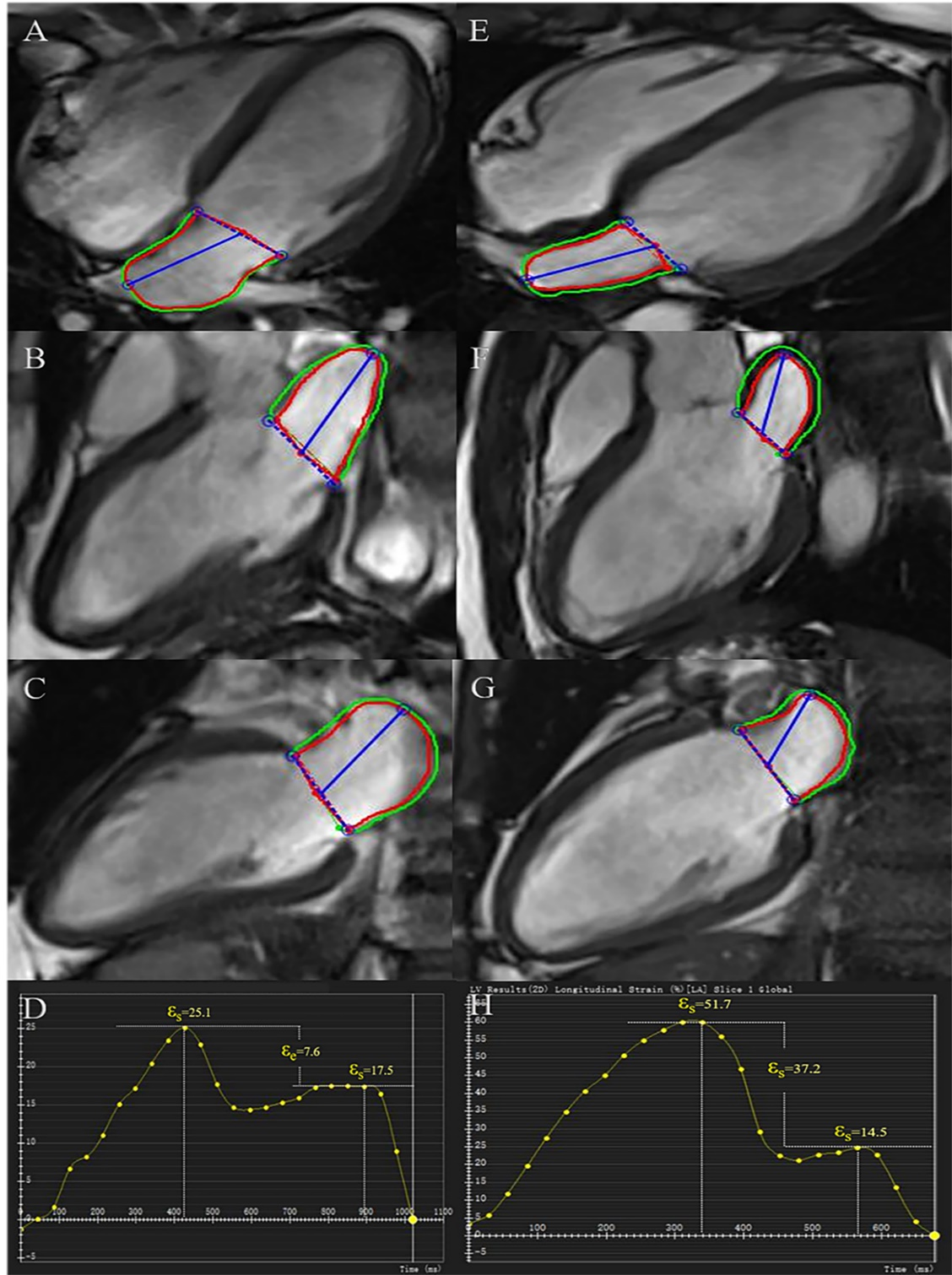
PLWH had a larger left atrial volume maximum index (LAVImax: 32.6±8.6mL/m2 vs. 28.7±8.1 mL/m2, P=0.006; ), minimum (LAVImin: 14.8±5.5 mL/m2 vs.11.5±5.4 mL/m2, P<0.001), and prior to atrial contraction (LAVIpre-a: 23.4±6.7mL/m2 vs. 19.7±7.2 mL/m2, P=0.002) as compared to healthy volunteers. The LAreservoir (LA total EF: 55.0±10.1 vs. 61.4±10.3, P<0.001;εs: 29.0±8.1 vs. 33.8±11.8,P=0.002), conduit (LA passive EF: 28.4±8.2 vs. 32.3±11.3, P=0.01l; εe: 16.3±6.5 vs.18.9±8.2, P=0.03) and booster pump function (LA booster EF: 37.4±12.4 vs.42.7±13.1, P=0.01, εa: 12.7±5.1 vs. 14.9±5.7, P=0.005) were all impaired in PLWH. Global circumferential left ventricular diastolic strain rate (LVGCS-d) was lower in the HIV patients(P=0.004). Multivariate analysis results showed that Nadir CD4+ T cells had an adverse association with LVGCS-d (y=0.61+0.001x, r=0.64, P<0.001).Discussion
In this study we explored the presence and extent of left atrial and left ventriculardysfunction by using volumetrics and strain analysis assessed by cardiovascularmagnetic resonance in HIV patients and sought to correlate functional changes withclinical markers of disease activity. The main findings of our study are: 1. HIVpatients revealed larger atrial volumes and lower left atrial function as compared tohealthy subjects. 2. Atrial strain analysis was also abnormal in HIV patients ascompared to healthy subjects. 3. Left ventricular strain analysis was lower in HIVpatients as compared to normal subjects. 4. Left ventricular strain was significantlycorrelated with lower nadir CD4+ counts. Collectively, our findings indicate thatdiastolic atrial and left ventricular dysfunction is prevalent in our patient cohort andthat markers of disease activity are more pronounced in conjunction with abnormalleft ventricular strain.Conclusion
Atrial and left ventricular diastolic dysfunction is manifest in people living with chronic human immunodeficiency virus infection and correlates with marker of more severe immune damage.Acknowledgements
This author takes responsibility for all aspects of the reliability and freedom from biasof the data presented and their discussed interpretation.References
1. UNAIDS. UNAIDS global report on AIDS. 2020.2. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations forthe evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr.2009;10(2):165-93.3. Peters DC, Lamy J, Sinusas AJ, Baldassarre LA. Left atrial evaluation by cardiovascular magneticresonance: sensitive and unique biomarkers. Eur Heart J Cardiovasc Imaging. 2021;23(1):14-30.4. de Leuw P, Arendt CT, Haberl AE, Froadinadl D, Kann G, Wolf T, et al. Myocardial Fibrosis andInflammation by CMR Predict Cardiovascular Outcome in People Living With HIV. JACC CardiovascImaging. 2021;14(8):1548-57.5. Chirinos JA, Sardana M, Ansari B, Satija V, Kuriakose D, Edelstein I, et al. Left Atrial PhasicFunction by Cardiac Magnetic Resonance Feature Tracking Is a Strong Predictor of IncidentCardiovascular Events. Circ Cardiovasc Imaging. 2018;11(12):e007512.Figures