1660
Effects of blood uric acid levels and omega-6/omega-3 on left heart function: a CMR feature tracking analysis1The Second Affiliated Hospital of Dalian Medical University, Dalian, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Hyperuricemia and abnormal ω-6/ω-3 values contribute to cardiac damage, but the specific mechanisms remain unclear.
Goal(s): To explore the effects of uric acid and ω-6/ω-3 values on left heart function using cardiac magnetic resonance feature tracking.
Approach: We utilized the TrueFISP cine sequence, CVI42 software, and univariate and multivariate linear regression analyses to identify relationships of uric acid and ω-6/ω-3 values with left heart function.
Results: High ω6/ω3 values may exacerbate left ventricular dysfunction in patients with hyperuricemia.
Impact: Our findings concerning the effects of uric acid and ω-6/ω-3 values on left heart function will help to improve the clinical management and treatment of patients with hyperuricemia.
Omega-3 (ω-3) and omega-6 (ω-6) unsaturated fatty acids are associated with cardiovascular disease1 and worse cardiovascular outcomes2. Previous studies showed no statistically significant associations of plasma ω-6 or ω-3 levels with left ventricular (LV) structural parameters by using cardiac magnetic resonance imaging (CMR)3. However, no studies have explored the effects of uric acid (UA) and abnormal ω-6/ω-3 values on left heart strain parameters. Therefore, this study investigated the effects of UA and abnormal ω-6/ω-3 values on left heart function by cardiac magnetic resonance feature tracking (CMR-FT).
This study included 300 patients with normal left ventricular ejection fraction (LVEF) who underwent CMR from September 2019 to May 2022 in our cardiology department. All subjects gave written informed consent. They were divided into two groups (ω6/ω3>5 and ω6/ω3≤5), and each of the groups was divided into four independent subgroups using UA quartiles. The exclusion criteria included LVEF<50%, acute renal insufficiency, malignant tumor, and presence of organic heart disease. All individuals underwent CMR on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthineers AG, Erlangen, Germany). Imaging parameters for TrueFISP cine were as follows: TR=39.2 ms, TE=1.43 ms, flip angle=39°, slice thickness=8 mm, matrix size=208*139, voxel size=1.6*1.6*6 mm3, acquisition time=8s, acquisition heartbeat=4.62, and FOV=234 mm*280 mm. It was performed from the base to the apex level on short-axis and long-axis views; continuous cine imaging results were subjected to post-processing. CMR images of patients were utilized to evaluate structure, function, and myocardial strain parameters in the left atrium (LA) and left ventricle (LV) via CVI42 software (Circle Cardiovascular Imaging, Inc., Calgary, Canada) (Figure 1). All data were analyzed using SPSS statistical software (version 26.0; SPSS Inc., Chicago, IL, USA). Normally distributed continuous variables were expressed as means ± standard deviations and compared using Student’s t-test or one-way analysis of variance; non-normally distributed variables were expressed as medians (interquartile ranges) and compared using the Mann–Whitney U test or Kruskal–Wallis test. To identify independent indicators of LV strain, variables with P<0.05 in univariate linear regression analyses were included in multivariate linear regression models using stepwise forward selection.
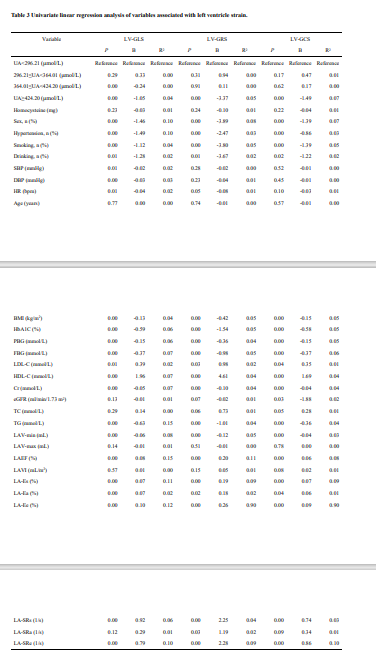
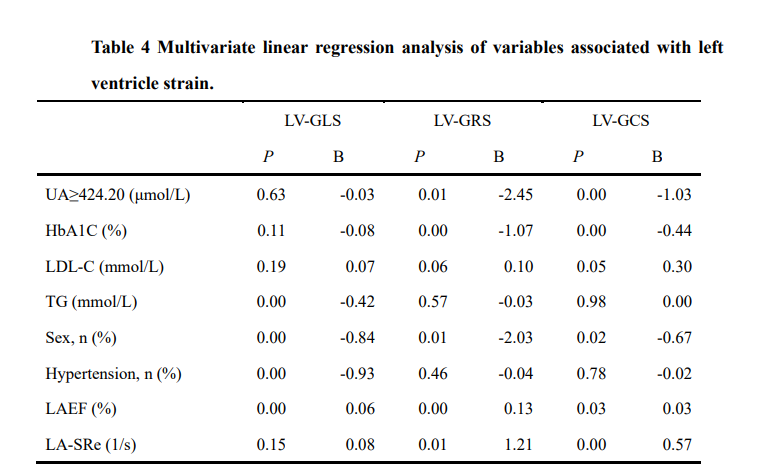
Compared with the ω6/ω3≤5 group, LV global longitudinal strain (LV-GLS), LS-apical, LV global radial strain (LV-GRS), RS-apical, circumferential strain-apical (CS-apical), and CS-mid were increased in the ω6/ω3>5 group (P<0.05) (Table 1). At the same UA quartile, ω6/ω3 values had no effect on LA or LV strain (P>0.05). In the ω6/ω3>5 group, LV-GLS, LS-apical, LV-GRS, RS-apical, RS-mid, RS-basal, LV global circumferential strain (LV-GCS), CS-apical, CS-mid, CS-basal, and peak diastolic strain rate (PDSR-L/S)-longitudinal/circumferential progressively decreased with increasing UA quartile (P<0.05). However, there were no significant differences in LA reservoir function, conduit function, and pump function among subgroups with different UA quartiles (P>0.05) (Table 2). Univariate linear regression demonstrated that hyperuricemia was associated with impaired LV strain (GLS, GRS, GCS) (P<0.05) (Table 3). Adjusted multivariate linear regression analyses showed that hyperuricemia had an independent effect on impaired LV strain (GRS, GCS) (P<0.05). Furthermore, triglycerides (TG), left atrial ejection fraction (LAEF), female sex, and presence of hypertension were independently associated with LV-GLS; glycated hemoglobin (HbA1C), female sex, LAEF, and LA early negative peak strain rate (LA-SRe) were independently associated with LV-GRS; and LAEF, HbA1C, low-density lipoprotein cholesterol (LDL-C), female sex, and LA-SRe were independently associated with LV-GCS (Table 4).
In this study, we used magnetic resonance feature tracking to examine the effect of UA level on left heart function at multiple ω6/ω3 values. We found that an increase in UA could lead to LV strain reduction in patients with ω6/ω3>5, predominantly in the apical region, although it did not have a significant effect on LA strain. Furthermore, multivariable linear regression analysis indicated that hyperuricemia was an independent indicator of LV strain. These findings suggest a unique role for LV strain in the assessment of altered left heart function, implying that high ω6/ω3 values may exacerbate LV dysfunction in patients with hyperuricemia. Our results will help to improve the clinical management and treatment of patients with hyperuricemia.
Acknowledgements
We thank the Siemens Research Team and the scientific adviser, Xiaofeng Qu, for organizational guidance during this project. Their contributions considerably improved the usefulness of the results.References
[1]. Tortosa-Caparrós E, Navas-Carrillo D, Marín F, et al. Anti-inflammatory effects of omega 3 and omega 6 polyunsaturated fatty acids in cardiovascular disease and metabolic syndrome. Crit Rev Food Sci Nutr. 2017;57: 3421-3429.
[2]. Liu Ju H, Wu Mei Z, Li Si M, et al. Association of serum uric acid with biventricular myocardial dysfunction in patients with type 2 diabetes mellitus. Nutr Metab Cardiovasc Dis. 2021;31: 2912-2920.
[3]. Anderson Jennifer S, Nettleton Jennifer A, Hundley W G, et al. Associations of plasma phospholipid omega-6 and omega-3 polyunsaturated Fatty Acid levels and MRI measures of cardiovascular structure and function: the multiethnic study of atherosclerosis. J Nutr Metab. 2011; 2011: 315134.
Figures
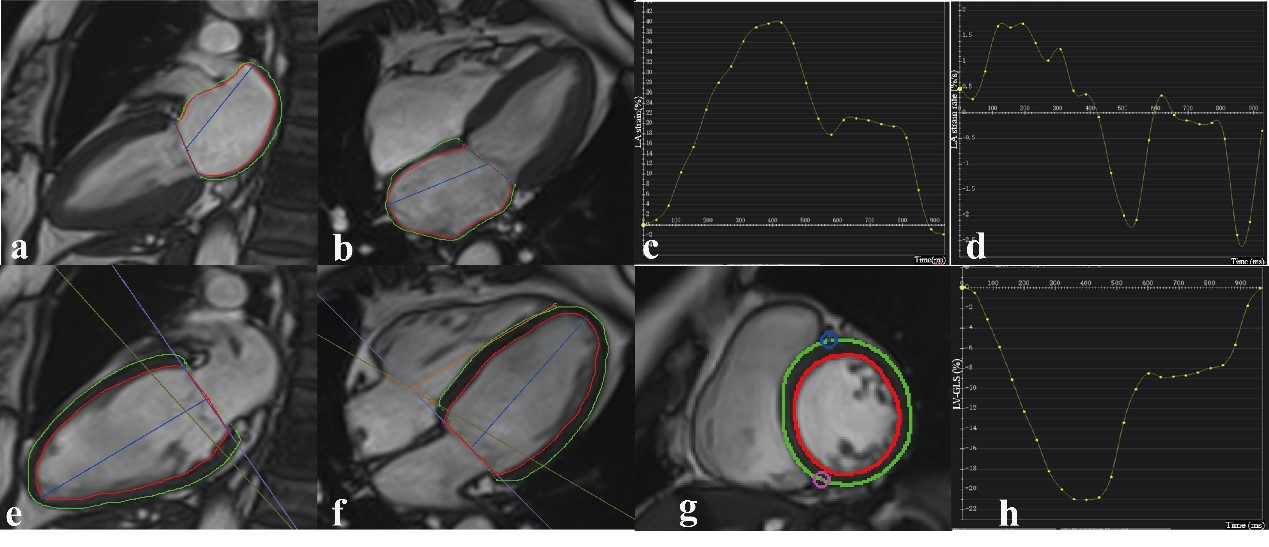
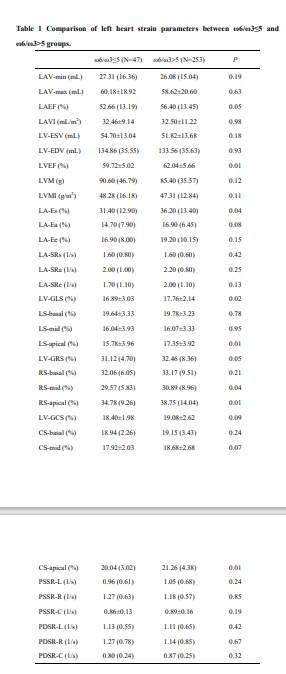
Table 1 Comparison of left heart strain parameters between ω6/ω3≤5 and ω6/ω3>5 groups.
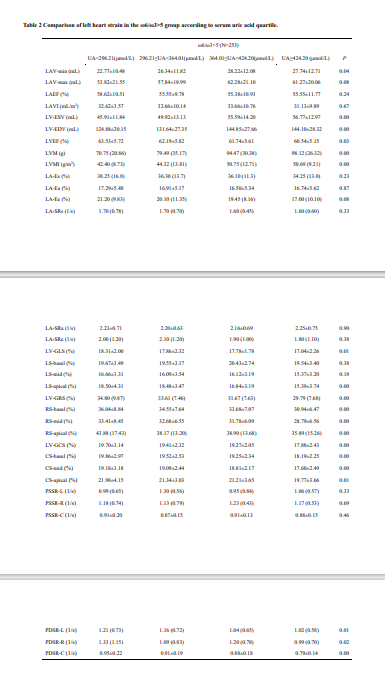
Table 2 Comparison of left heart strain in the ω6/ω3>5 group according to serum uric acid quartile.