1658
The value of left atrial strain for predicting left ventricular reverse remodeling in dilated cardiomyopathy patients1Department of Radiology, The Second Clinical Medical College of Nanchang University, Nanchang, China, 2The Children's Hospital of Zhejiang University School of Medicine, Radiology, Hangzhou, China, 3GE Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiomyopathy, Cardiac magnetic resonance, Left ventricular reverse remodeling, Left atrial strain
Motivation: The structure and function of left atrial (LA) have shown significant value in prognostic and risk stratification in dilated cardiomyopathy (DCM) patients. But no previous studies had reported its value for predicting left ventricular reverse remodeling (LVRR) in DCM.
Goal(s): This study aimed to explore whether fast long-axis strain (FLAS) of LA can provide predictive value.
Approach: LA strain and other cardiac magnetic resonance (CMR) parameters were measured by CVI (version 5.13.7) in 96 patients. Statistical analysis was performed using SPSS.
Results: Both LACS and LGE were independent predictors of LVRR. The combination of LACS and LGE provided better prediction performance.
Impact: For the first time, our study demonstrated the predictive value of LA strain for LVRR. It would be beneficial for DCM patients who were contradictive to contrast agencies.
Introduction
Dilated cardiomyopathy (DCM) is a heterogeneous disease characterized by ventricular enlargement and systolic dysfunction [1]. Its pathogenic mechanism is mainly the rise of ventricular load and progression of myocardial remodeling caused by the loss of myocardial systolic function, which ultimately results in heart failure [2]. After pharmacological, mechanical, or surgical therapy, the cardiac function can be partial or total restoration, which named left ventricular reverse remodeling (LVRR) [3]. Studies have shown that heart failure patients with LVRR have lower mortality than those without LVRR (8% vs. 30%), and the probability of complex endpoint events, such as heart failure readmission and cardiac arrest, is also lower (9.5% vs. 24.2%) [4, 5]. Thus, the prediction of LVRR is important for the selection of clinical interventions [6]. In recent studies, left atrial (LA) structure and function have shown significant value in prognostic and risk stratification in DCM patients [7, 8]. To our knowledge, no previous studies had reported the value of LA strain for predicting LVRR in DCM. Therefore, this study aimed to explore if fast long-axis strain (FLAS) of LA can provide predictive value.Methods and Materials
Study population51 patients with LVRR (36 men, 46.90±14.76 years) and 45 patients without LVRR (27 men, 50.13±13.70 years) were enrolled in the study.
Cardiac magnetic resonance imaging protocols
Cardiac magnetic resonance (CMR) was performed using a 3.0T MRI scanner (Discovery MR750W; GE Healthcare, Milwaukee, CA, USA) with an 8-channel cardiac coil. Electrocardiogram and respiratory navigators were used for all CMR. The patients were trained to breathe for 3 minutes and repeat inhaling, exhaling, and end-exhaling hold as instructed before imaging. Cardiac cine images in short-axis and long-axis planes (including 2-chamber, 3-chamber, and 4-chamber) from the base to the apical level were performed by steady-state free precession sequences. The dose of gadobutrol (Gadovist, Bayer HealthCare Pharmaceuticals, Germany) was 0.1 mmol/kg. The intravenously injection rate was 3.0 mL/s and followed by a 10-20 mL saline flush. At 8-10 minutes after contrast administration, inversion recovery gradient echo sequence was used to acquire late gadolinium enhancement image.
Imaging analysis
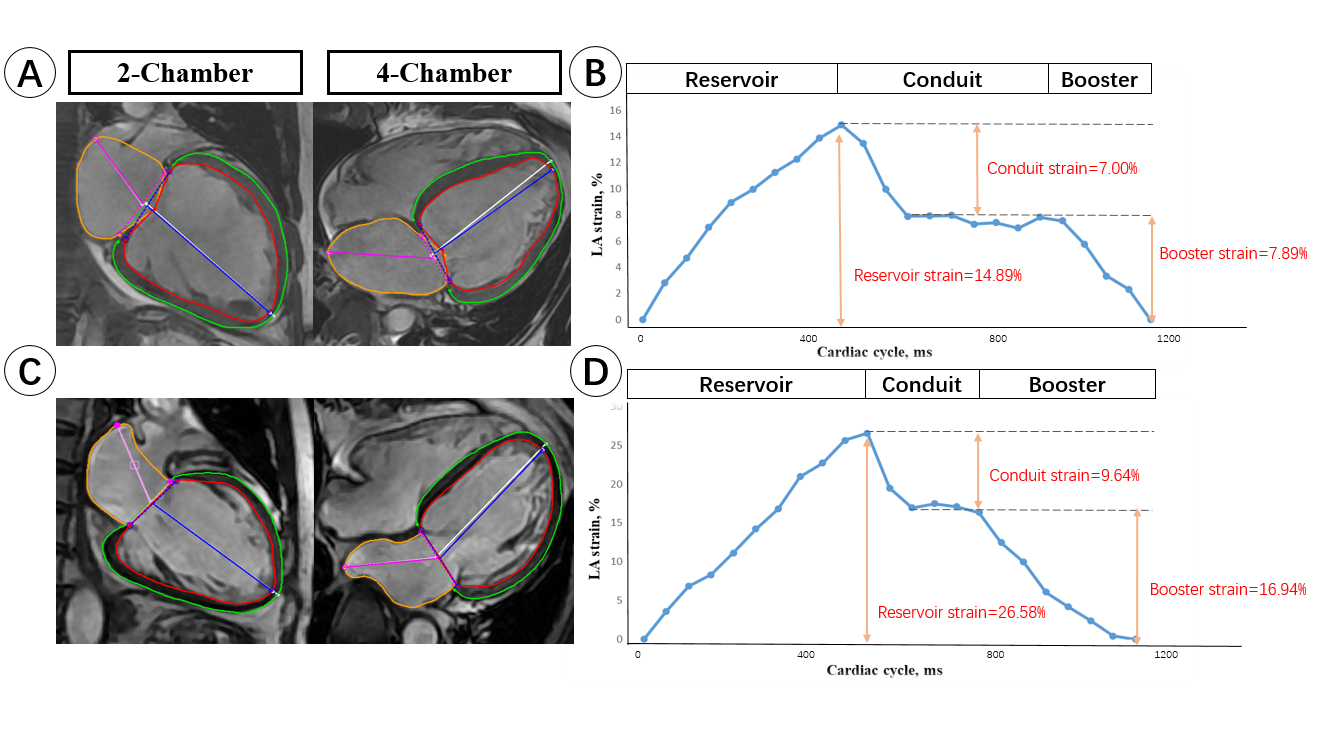
All CMR data was analyzed on CVI (version 5.13.7). The FLAS analysis of LA was performed on two- and four-chamber long-axis views by one author who was blinded to clinical data and other MRI information, and another physician with 5 years of CMR experience reviewed the results. The strain curve was plotted based on the average LA junction strain value during the cardiac cycle (Figure 1). One author analyzed other CMR parameters, such as left ventricular end-diastolic index (LVEDVi), late gadolinium enhancement extent (LGE) and left ventricular ejection fraction (LVEF).
Statistical Analysis
Statistical analysis was performed using SPSS (version 26.0, Statistical Package for the Social Sciences, International Business Machines, Inc., Armonk, New York, USA). Data were subjected to a normality test using the Shapiro-Wilk normality test. Continuous variables were compared using independent samples t-tests or Mann-Whitney U tests. Categorical variables were compared using χ2, continuous correction χ2 test, or Fisher’s exact tests. Variables with P < 0.05 in the univariate analyses were selected for the forward stepwise multivariable analysis. The variance inflation factor was used to determine collinearity, and one variable was included in the multivariable analysis among parameters with variance inflation factor greater than 2.0. Variables with P < 0.05 in the multivariable analyses were selected to build predictive models and ROC analysis. The correlation was assessed by using the Pearson correlation coefficient (r value). Delong test was used to compare the differences between different models. Intra- and inter-observer variability was tested by using the intraclass correlation coefficient.
Result
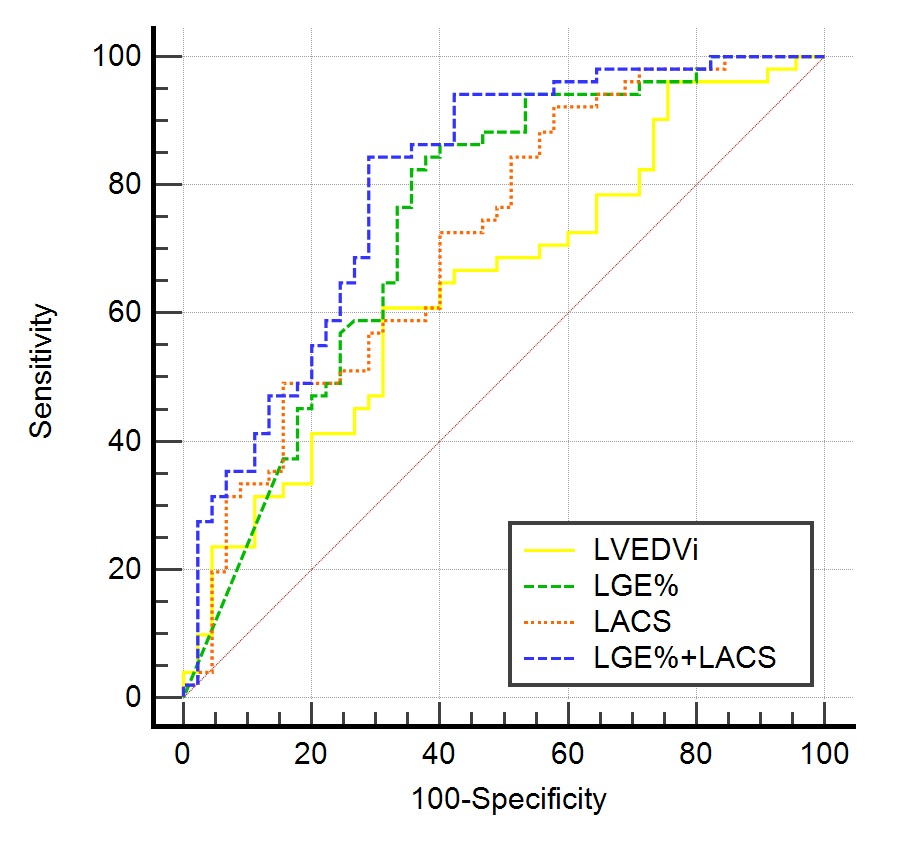
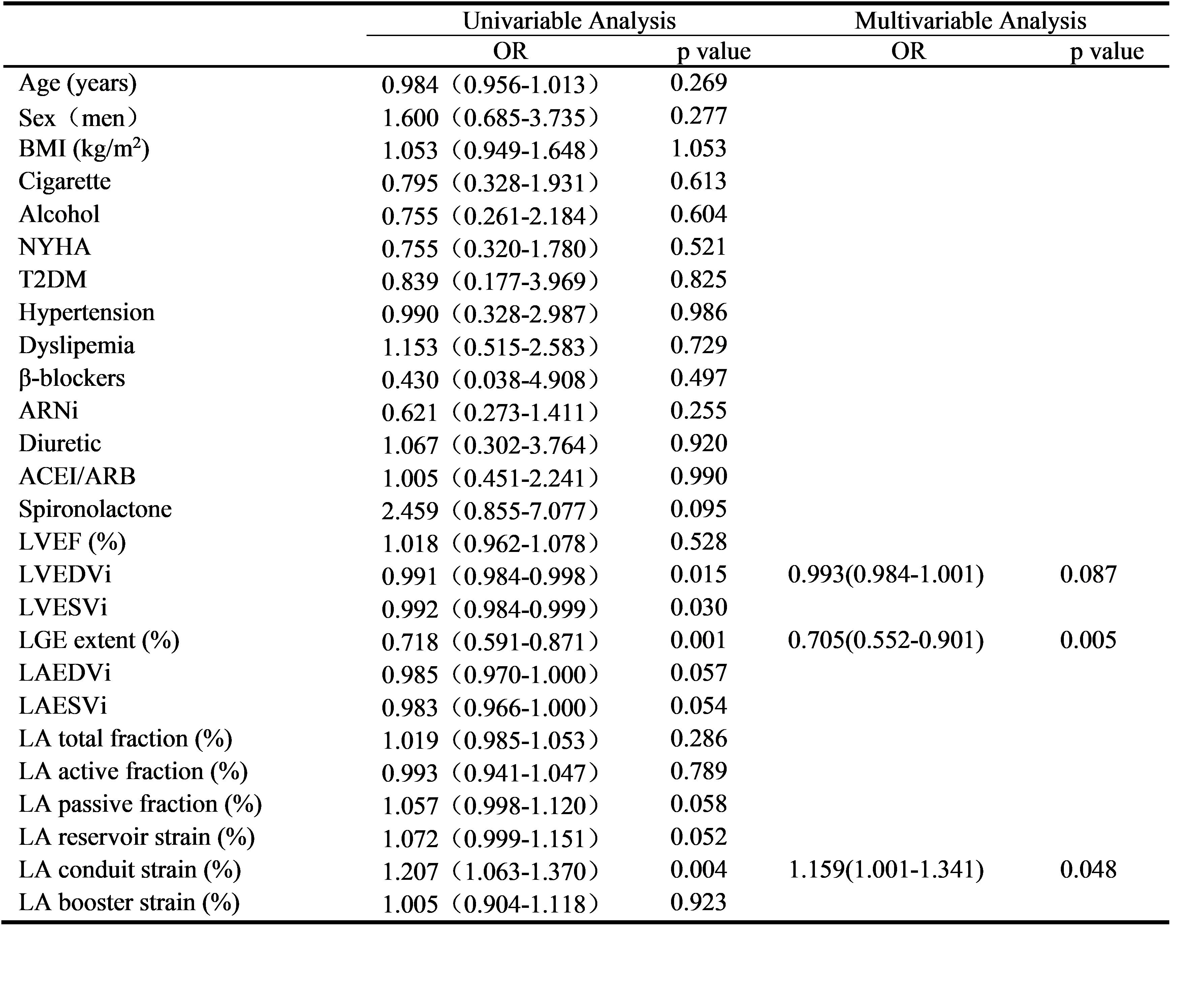
In LVRR group, the LA reservoir strain [6.32 (4.12-9.45) vs. 4.05 (2.06-6.36); p<0.001] and LACS [11.48 (8.66-16.11) vs. 8.78 (5.61-13.04); p=0.011] were higher than non-LVRR group, and the LVEDVi [155.34 (117.79-195.30) vs. 177.43 (145.07-246.75); p=0.014], LGE [1.58 (0.00-2.44) vs. 5.63 (1.23-6.94); p< 0.001] were lower. Multivariable analysis revealed that LGE (OR:0.705 95% CI:0.552-0.901, p=0.005) and LA conduit strain (LACS) (OR:1.159 95% CI:1.001-1.341, p=0.048) were independent predictors of LVRR in DCM. The combination of LGE and LACS has the best performance (AUC=0.801, CI: 0.707-0.876), and is better than LGE (AUC=0.745, CI: 0.645-0.828, p=0.077) and LACS (AUC=0.717, CI: 0.616-0.804, p=0.070) (Figure 2).Discussion and Conclusions
This study investigated whether LA strain could predict the occurrence of LVRR in DCM patients. The results showed that LACS as well as LGE at baseline were significantly different between LVRR and non-LVRR patients. Consistent with previous studies the LGE was independent predictor of LVRR in DCM [9, 10]. For the first time, our results showed LACS as novel independent predictor. This may because patients with larger LACS at baseline are in the early stage of disease and can get benefit easily from clinical treatment. The predictive performance was comparable between LACS and LGE. Thus, LACS was particularly valuable for predicting LVRR for DCM patients who were contradictive to contrast agencies. In addition, the combination of LACS and LGE showed improved prediction performance.In conclusion, a higher LA conduit strain at baseline could predict the occurrence of LVRR in DCM.
Acknowledgements
No acknowledgement found.References
1. Ciarambino, T., et al., Cardiomyopathies: An Overview. Int J Mol Sci, 2021. 22(14).
2. Schultheiss, H.P., et al., Dilated cardiomyopathy. Nat Rev Dis Primers, 2019. 5(1): p. 32. 3. González, A., et al., Cardiac remodelling - Part 1: From cells and tissues to circulating biomarkers. A review from the Study Group on Biomarkers of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail, 2022. 24(6): p. 927-943.
4. Gold, M.R., et al., Redefining the Classifications of Response to Cardiac Resynchronization Therapy: Results From the REVERSE Study. JACC Clin Electrophysiol, 2021. 7(7): p. 871-880.
5. Bulluck, H., et al., Redefining Adverse and Reverse Left Ventricular Remodeling by Cardiovascular Magnetic Resonance Following ST-Segment-Elevation Myocardial Infarction and Their Implications on Long-Term Prognosis. Circ Cardiovasc Imaging, 2020. 13(7): p. e009937.
6. Kimura, Y., et al., A clinical score for predicting left ventricular reverse remodelling in patients with dilated cardiomyopathy. ESC Heart Fail, 2021. 8(2): p. 1359-1368.
7. Raafs, A.G., et al., Left Atrial Strain Is an Independent Predictor of New-Onset Atrial Fibrillation in Dilated Cardiomyopathy. JACC Cardiovasc Imaging, 2023.
8. Lydell, C.P., et al., Left Atrial Function Using Cardiovascular Magnetic Resonance Imaging Independently Predicts Life-Threatening Arrhythmias in Patients Referred to Receive a Primary Prevention Implantable Cardioverter Defibrillator. Can J Cardiol, 2019. 35(9): p. 1149-1157.
9. Kubanek, M., et al., Novel predictors of left ventricular reverse remodeling in individuals with recent-onset dilated cardiomyopathy. J Am Coll Cardiol, 2013. 61(1): p. 54-63. 10. Xu, Y., et al., Myocardial Tissue Reverse Remodeling After Guideline-Directed Medical Therapy in Idiopathic Dilated Cardiomyopathy. Circ Heart Fail, 2021. 14(1): p. e007944.
Figures