1657
Cardiac function and strain analysis at 7T in comparison to 3T1Dept. of Diagnostic, Interventional and Pediatric Radiology, Inselspital, Bern University Hospital, Bern, Switzerland, 2Translation Imaging Center (TIC), Swiss Institute for Translational and Entrepreneurial Medicine, Bern, Switzerland, 3Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Bern, Switzerland, 4Magnetic Resonance Methodology, Institute of Diagnostic and Interventional Neuroradiology, Inselspital, Bern University Hospital, Bern, Switzerland, 5Physikalisch-Technische Bundesanstalt (PTB), Berlin, Germany, 6Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, 7Department of Anaesthesiology and Pain Medicine, Inselspital, Bern University Hospital, Bern, Switzerland
Synopsis
Keywords: Myocardium, High-Field MRI, Cardiac function, Strain
Motivation: To investigate whether a single set of shim values can provide reliable image quality for cardiac MRI at 7T.
Goal(s): To establish an efficient workflow for cardiac cine imaging at 7T.
Approach: Short-axis and long-axis views were acquired in five subjects with different spatial resolution at 3T and 7T. Volumetric parameters and peak global longitudinal and circumferential strain were assessed for left and right ventricle.
Results: No significant differences of volume parameters, field strength or spatial resolution were found. A single B1 shim set for the whole examination providing reliable image quality and quantification results constitute an essential step towards clinical cardiac imaging.
Impact: An efficient workflow and reliable image quality of cine images for the assessment of cardiac volumes and strain at 7 Tesla could be realized with results in close agreement to 3T – an essential step towards clinical routine cardiac examinations.
INTRODUCTION
Even though progress in Ultra-high field MRI has been made revealing clinical potential of body imaging at 7 Tesla, it is still far from being established in a clinical setting1. The major drawback hindering this step is given by the shorter RF wavelength compared with lower field strength leading to strong spatial heterogeneities of the transmit B1+ magnitude. To tackle this pitfall, static and dynamic parallel transmission (pTx) strategies have been proposed that, however, may yield in a significant increase of the overall examination time2. The feasibility of cine imaging and assessing volumetry of the heart at 7T has been demonstrated3-5. However, these studies were lacking from 3T comparison, dedicated RF optimizations, state-of-the-art hardware (e.g. 1Tx coil) etc.The purpose of this study focused on following aspects: 1) Establish an efficient workflow for additional 7T-specific static pTx (B1 shimming) procedure as short as possible. 2) Investigate whether a single set of B1 shim values calculated at the beginning of the exam provides reliable image quality over a region of interest (ROI). 3) Investigate whether spatial resolution or field strength has an influence on volumetric and myocardial strain parameters. 4) Parameter comparison to 3T.
METHODS
Data acquisitionFive healthy volunteers were examined at 7T and, subsequently, at 3T (MAGNETOM Terra and Prisma, Siemens Healthcare, Erlangen, Germany) on the same day using an 8-channel Tx and 32-channel Rx (Tesla Dynamic Coils, Zaltbommel, The Netherlands) and a standard 32-channel Rx body coil, respectively. The protocol consisted of cine acquisition of 2-, 3-, and 4-chamber views as well as of a short-axis (SA) stack covering the left ventricle (LV). All of these acquisitions were performed twice with different in-plane resolution (“low res” and “high res”). Acquisition parameters are summarized in Fig.1.
B1 phase shimming at 7T
Following the initial localizers, a 2D relative B1 map6 was acquired in three equidistant transverse slices covering the heart from the base to the apex (8 mm slice thickness, 200% gap, TA 1:42 min). Volunteers were instructed to do shallow breathing during this acquisition. Raw data was transferred to an external computer and reconstruction was done in MATLAB (MathWorks, Natick, Massachusetts). One ROI was drawn on each slice containing LV and RV. To increase the B1+ homogeneity one shim set of phase values was calculated with the constraint of minimizing the coefficient of variation (CV=std/mean of |B1+|) within the ROI. A resulting B1+ phase shim vector for the 8 transmit channels was copied once to scanner and then automatically applied for all subsequent acquisitions. The time for the whole B1 shimming procedure (data acquisition, data transfer, reconstruction, ROI drawing, transfer of calculated shim set) was in the order of 5 minutes maximum.
Image analysis
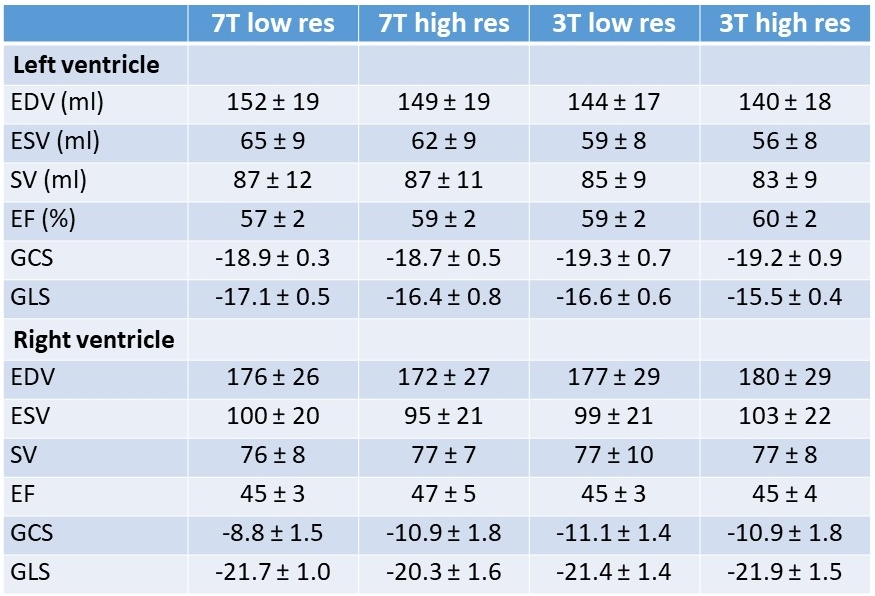
Data was analyzed using cvi42 (version 5.17, Circle Cardiovascular Imaging, Calgary, Canada). For all short-axis stacks (low res, high res, 3T, 7T), end-diastolic (EDV), end-systolic (ESV), stroke volumes (SV), and ejection fraction were assessed for LV and RV. Furthermore, peak global longitudinal strain (GLS) and peak global circumferential strain (GCS) were determined using feature tracking (FT). A paired non-parametric general linear model not accounting for multiple comparisons was used to compare the acquisitions.
RESULTS and DISCUSSION
The B1 shim set turned out to provide excitation patterns without substantial dropouts in the region of the three transverse slices. Fig.2 shows systolic and diastolic 4-chamber and short-axis views of one subject for both field strengths. Fig.3 shows short-axis and 4-chamber images in all subjects at 7T. Quantitative data evaluation is summarized in Fig.4. No significant differences of volume parameters, field strength or spatial resolution was observed (p>0.05); however, more subjects are required for a valid statistical analysis.In all subjects, a reduced contrast between myocardium and blood pool was observed for GRE images at 7T compared to bSSFP images at 3T, which was always more pronounced in long-axis images due to lower inflow effect compared to short-axis acquisitions. However, despite residual B1+ variations (cf. Fig.3) the reduced contrast did not affect the final volumetry and strain quantifications. For FT, more corrections and guiding contours were required during the analysis on the 7T long-axis views and on the short-axis of the RV to achieve an accurate tracking of the myocardium.
CONCLUSION
A fast and efficient workflow could be realized at 7T for cardiac cine examination with no significant difference in function and strain parameters to 3T. The B1 shimming procedure could be further accelerated to only about 3 minutes additional time by using the GRE localizers in the very beginning for the estimation of B1 maps7.Acknowledgements
No acknowledgement found.References
Figures
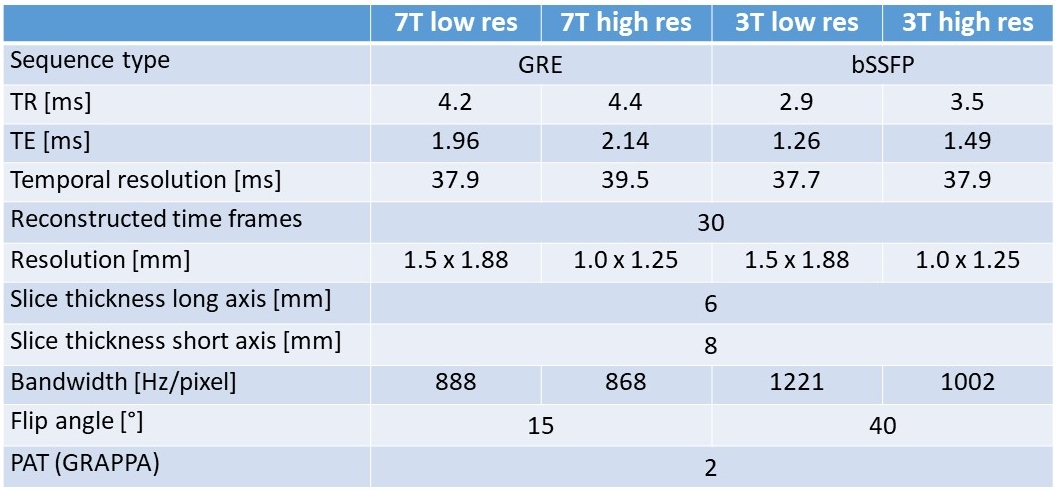
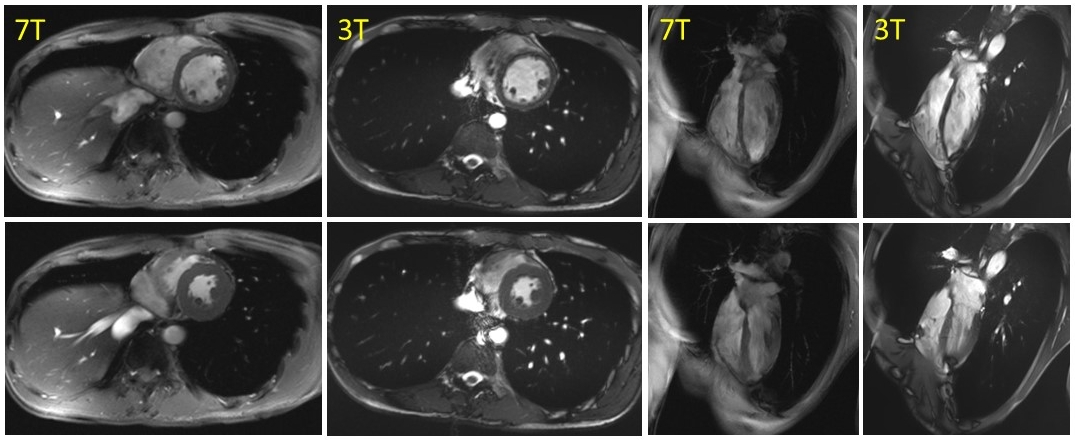
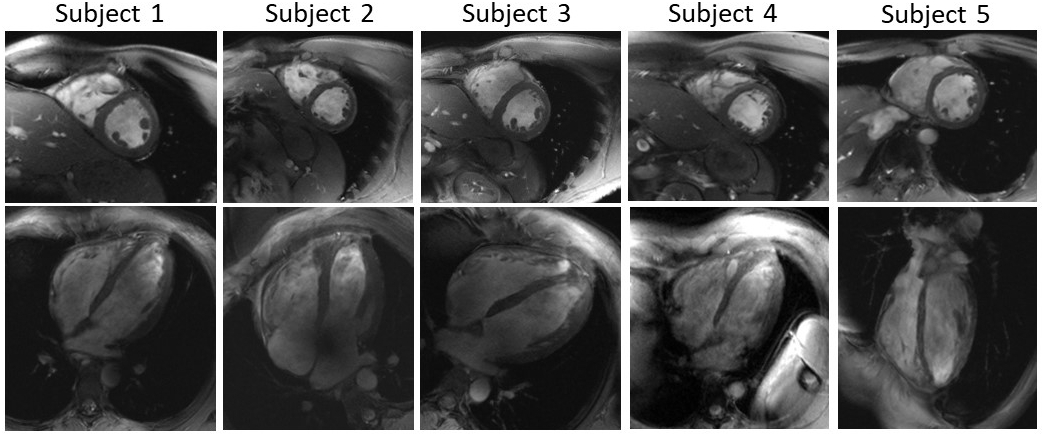
Fig. 3: High-resolution diastolic midventricular short-axis slice (top row) and 4-ch view (bottom row) for all subjects acquired at 7T. In subject 2 some shading due to B1 inhomogeneity can be observed in the left atrium.