1656
Left atrial strain for prediction of left ventricular reverse remodeling after STEMI by cardiac magnetic resonance feature-tracking1Radiology, Tongji Hospital, Tongji Medical College,Huazhong University of Science and Technology, Wuhan, China, 2Neurology, Xinqiao Hospital and the Second Affiliated Hospital, Army Medical University (Third Military Medical University), Chongqing, China, 3Radiology, Tongji Hospital, Tongji Medical College,Huazhong University of Science and Technology, wuhan, China
Synopsis
Keywords: Atherosclerosis, Cardiovascular, ST-segment elevation myocardial infarction; Left ventricular reverse remodeling; Cardiac magnetic resonance; Left atrial strain.
Motivation: Few studies have assessed the association of left atrial (LA) strain with left ventricular reverse remodeling (LVRR) after ST-segment elevation myocardial infarction (STEMI).
Goal(s): To investigate the potential utility of LA strain by using cardiac magnetic resonance feature-tracking (CMR-FT) to predict LVRR following STEMI.
Approach: The prospective study analyzed patients with a first STEMI and two CMR scans at 5 days and 4 months, and quantified LA strain by CMR-FT using cine images.
Results: LA reservoir and conduit strain, together with infarct size were independent predictors of LVRR.
Impact: The demonstrated predictive value of LA strain for the occurrence of LVRR after STEMI enables better assessment for the improvement of myocardial injury and guidance for the treatment in STEMI patients.
Introduction
Left ventricular reverse remodeling (LVRR) after ST-segment elevation myocardial infarction (STEMI) is associated with favorable outcomes. Cardiac magnetic resonance feature-tracking (CMR-FT) allows quantitative assessment of left atrial (LA) strain in three phases through the cardiac cycle. So far, few studies have assessed the association of LA strain with LVRR after STEMI. The study aimed to investigate the potential utility of LA strain by using CMR-FT to predict LVRR after STEMI.Methods
Patients with a first STEMI treated by primary percutaneous coronary intervention were consecutively enrolled in the prospective study and underwent a CMR scan at 5 days and 4 months. LA global longitudinal strain (reservoir strain [εs], conduit strain [εe], booster strain [εa], and corresponding strain rate were assessed by CMR-FT using cine images. Image analysis was performed using commercially available software (CVI42, version 5.13.7, Circle Cardiovascular Imaging, Calgary, Canada). LVRR was defined as a reduction in the LV end-systolic volume index of > 10% from baseline to follow-up. Logistic regression analyses were performed to determine the predictors of LVRR.Results
Of 90 patients analyzed, patients with LVRR (n = 35, 39%) showed higher values of LA strain and strain rate, and less extensive infarct size (IS) compared to patients without LVRR (n = 55, 61%) at initial and second CMR. LVRR group demonstrated significant improvements in LV and LA cardiac function over time, especially the obvious increase in LA strain and strain rate. In multivariate logistic regression analyses, εs and εe, together with IS were independent predictors of LVRR. The combination of εs and IS could optimally predict the LVRR with the highest area under the curve of 0.743 (95% CI: 0.640 - 0.830).Discussion
The study observed that εs and εe, together with IS were independent predictors of LVRR in multivariate models, which can be explained as follows. LA relaxation and compliance, and LV systolic function can largely influence LA reservoir function during LV systole. Most patients manifested LV diastolic or systolic dysfunction in the acute stage, consistently with a decrease in εs. Second, LV relaxation and impaired atrioventricular pressure gradient owing to increased LV filling pressure have important effects on LA conduit function during LV early diastole. Thus, conduit function seems to be deteriorated in the early stage. Third, intrinsic LA contractility and LV end-diastolic compliance can largely impact LA booster function during LV late diastole. Acute myocardial infarction directly deteriorated LV function and subsequently affected LA function, thus, εa may be not an early predictor of LVRR after STEMI.Conclusion
Post-STEMI patients with LVRR presented better recovery from cardiac function and LA deformation compared to patients without LVRR. Assessment of εs and εe by using CMR-FT after STEMI enabled better prediction of LVRR, which may help to find a potential CMR-derived parameter for assessing the improvement of treatment in STEMI patients.Acknowledgements
We acknowledged Wenzhe Sun for his valuable contributions in the statistical analysis of the data.
References
- Bulluck H, Carberry J, Carrick D, et al. Redefining Adverse and Reverse Left Ventricular Remodeling by Cardiovascular Magnetic Resonance Following ST-Segment-Elevation Myocardial Infarction and Their Implications on Long-Term Prognosis. Circ Cardiovasc Imaging. 2020;13(7):e009937.
- Funaro S, La Torre G, Madonna M, et al. Incidence, determinants, and prognostic value of reverse left ventricular remodelling after primary percutaneous coronary intervention: results of the Acute Myocardial Infarction Contrast Imaging (AMICI) multicenter study. Eur Heart J. 2009;30(5):566-575.
- Bodi V, Monmeneu JV, Ortiz-Perez JT, et al. Prediction of Reverse Remodeling at Cardiac MR Imaging Soon after First ST-Segment-Elevation Myocardial Infarction: Results of a Large Prospective Registry. Radiology. 2016;278(1):54-63.
- Cui J, Zhao Y, Qian G, Yue X, Luo C, Li T. Cardiac magnetic resonance for the early prediction of reverse left ventricular remodeling in patients with ST-segment elevation myocardial infarction [published online ahead of print, 2023 Jul 17]. Eur Radiol. 2023;10.1007/s00330-023-09907-3.
- Lønborg JT, Engstrøm T, Møller JE, et al. Left atrial volume and function in patients following ST elevation myocardial infarction and the association with clinical outcome: a cardiovascular magnetic resonance study. Eur Heart J Cardiovasc Imaging. 2013;14(2):118-127.
- Kim J, Yum B, Palumbo MC, et al. Left Atrial Strain Impairment Precedes Geometric Remodeling as a Marker of Post-Myocardial Infarction Diastolic Dysfunction. JACC Cardiovasc Imaging. 2020;13(10):2099-2113.
- Schuster A, Backhaus SJ, Stiermaier T, et al. Left Atrial Function with MRI Enables Prediction of Cardiovascular Events after Myocardial Infarction: Insights from the AIDA STEMI and TATORT NSTEMI Trials. Radiology. 2019;293(2):292-302.
- Mălăescu GG, Mirea O, Capotă R, Petrescu AM, Duchenne J, Voigt JU. Left Atrial Strain Determinants During the Cardiac Phases. JACC Cardiovasc Imaging. 2022;15(3):381-391.
- Thomas L, Marwick TH, Popescu BA, Donal E, Badano LP. Left Atrial Structure and Function, and Left Ventricular Diastolic Dysfunction: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;73(15):1961-1977.
Figures
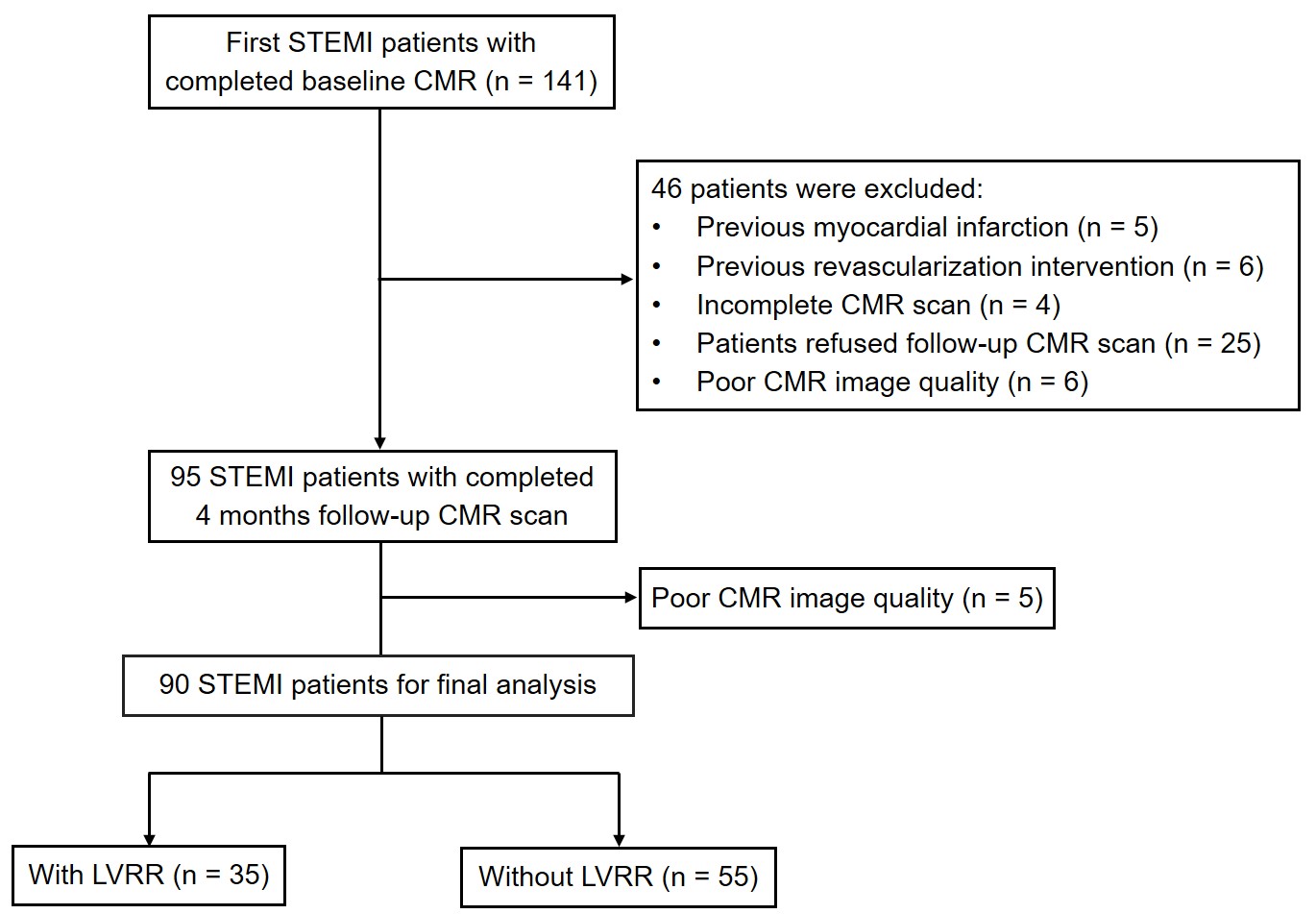
Fig. 1 Flow chart of study enrollment.
STEMI ST-segment elevation myocardial infarction, CMR cardiac magnetic resonance, LVRR left ventricular reverse remodeling.
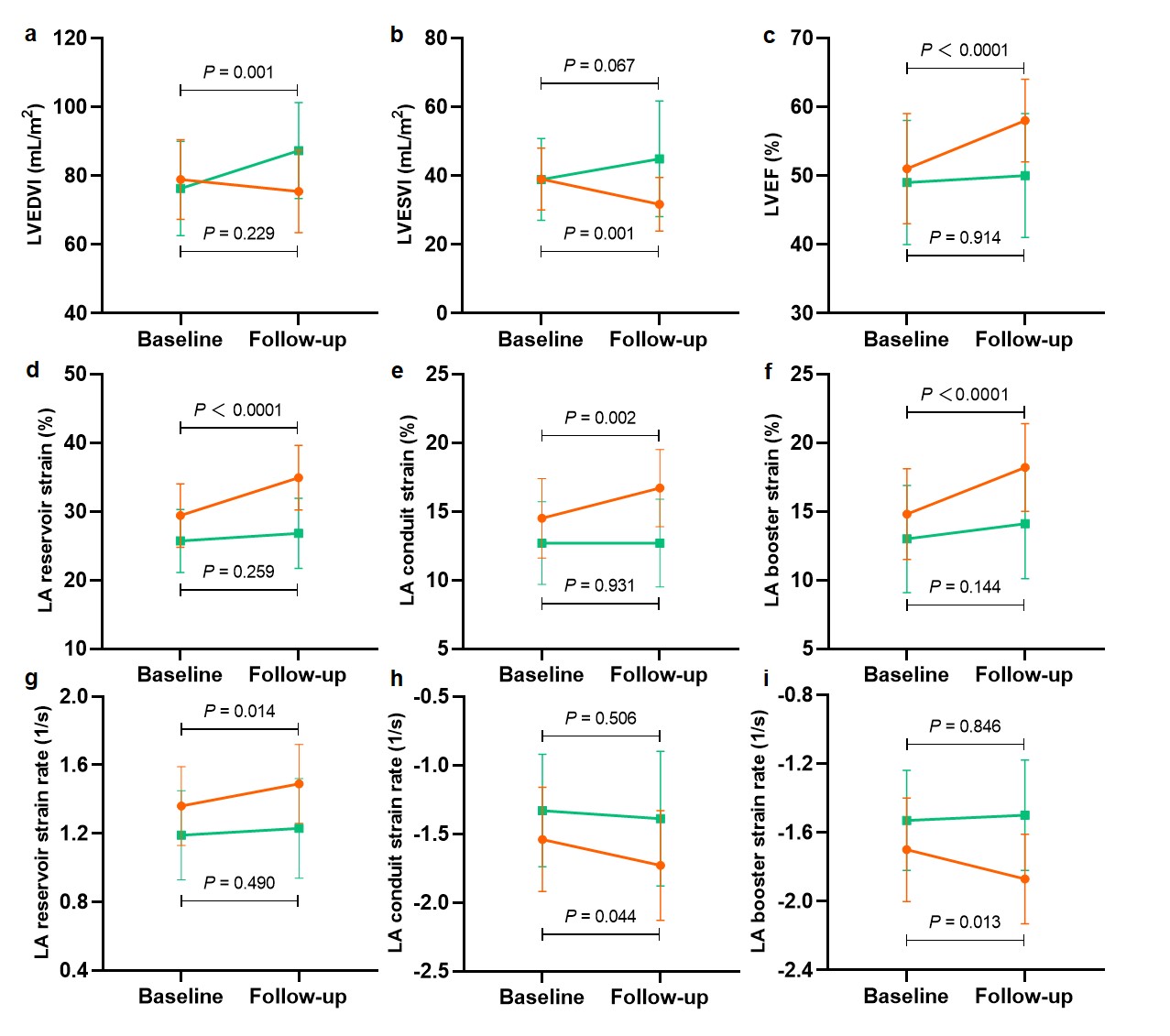
Fig. 2 Dynamic changes in LVEDVI (a), LVESVI (b), LVEF (c), and LA strain (d-f) and strain rate (g-i) in patients with and without LVRR from baseline to 4-month follow-up.
LVRR left ventricular reverse remodeling, LVEDVI left ventricular end-diastolic volume index, LVESVI left ventricular end-systolic volume index, LVEF left ventricular ejection fraction, LA left atrial.
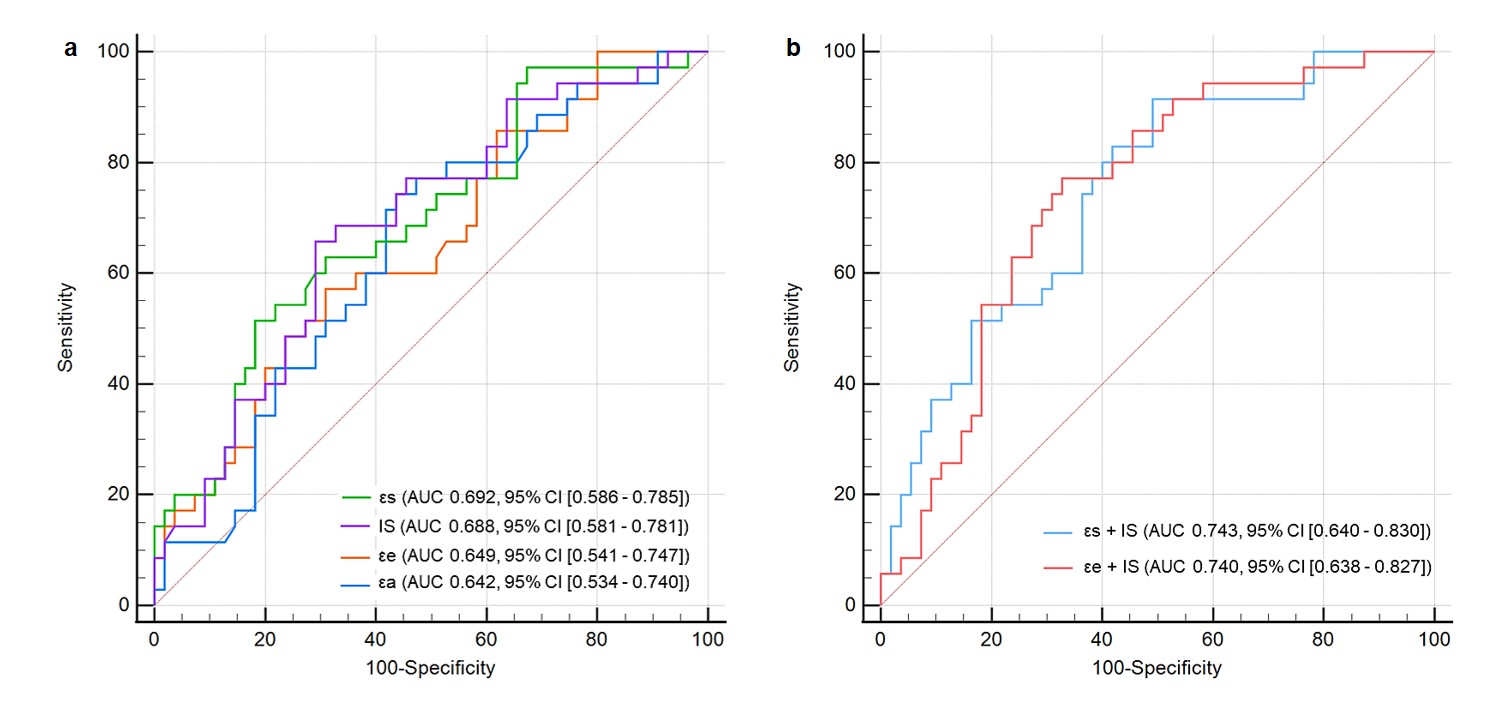
Fig 3. ROC curves of left atrial strain and infarct size (IS), as well as the combination of these parameters for prediction of LVRR.
ROC receiver-operating characteristic, LVRR left ventricular reverse remodeling, εs left atrial reservoir strain, εe left atrial conduit strain, εa left atrial booster strain, AUC area under the curve, CI confidence interval.
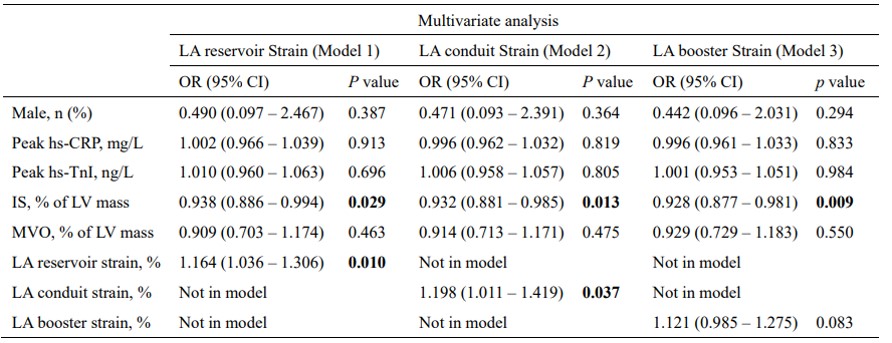
Table Predictors of LVRR in multivariate logistic regression analysis.
P values < 0.05 are highlighted in bold. LVRR left ventricular reverse remodeling, LA left atrial, OR odds ratio, CI confidence interval, hs-CRP high-sensitivity C-reactive protein, hs-TnI high-sensitivity cardiac troponin I, IS infarct size, MVO microvascular obstruction.