1655
Myocardial Strain Disparities in Genetic and Secondary Dilated Cardiomyopathy: Insights from Cardiac Magnetic Resonance Imaging1Department of Radiology, Peking University First Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiomyopathy, Dilated cardiomyopathy, Myocardial strain, Cardiac magnetic resonance imaging
Motivation: Dilated Cardiomyopathy (DCM) poses a significant clinical challenge due to its high mortality and limited cognitive understanding. Our motivation is rooted in enhancing diagnostic precision, unraveling novel insights into DCM pathology, and paving the way for targeted therapeutic interventions.
Goal(s): This study aims to unravel the intricate myocardial strain patterns in DCM patients through cardiac MRI techniques.
Approach: In this study, feature tracking method were used to evaluate myocardial strain.
Results: There is no significant difference in global left ventricular strain, variations emerge in segmental myocardial strain between genetic and secondary DCM patients. The myocardial strain rate exhibits disparities both globally and segmentally.
Impact: This study unveils nuanced myocardial strain disparities in DCM, which could be utilized to illuminate diagnostic precision. The insights catalyze targeted therapeutic strategies, potentially revolutionizing care for DCM patients.
Introduction
Dilated Cardiomyopathy (DCM) arises from a multitude of genetic and non-genetic factors, leading to left ventricular systolic dysfunction and dilatation independent of abnormal loading or coronary artery disease1. Clinical presentations vary from asymptomatic to heart failure symptoms, or sudden cardiac death in previously asymptomatic individuals. Precise evaluation of cardiac function is pivotal for effective treatment. Traditional parameters like left ventricular ejection fraction (LVEF), stroke volume (LVSV), and LV end-diastolic volume (LVEDV) may signal cardiac function alternative but lack sensitivity to myocardial wall motion abnormalities in cases of extensive impairment of myocardial contractility in DCM2. Cardiac magnetic resonance (CMR) feature tracking excels in gauging myocardial wall motion and strain changes, providing superior accuracy and reproducibility compared to echocardiography3, 4. While prior studies focused on overall LV mechanics in DCM patients, the global and segmental performance of the LV in genetic versus secondary DCM patients remains unexplored. Delving into these differences sheds light on unique etiologies, guiding personalized treatment, informing prognosis, and advancing our scientific understanding of these conditions. Consequently, this study aims to scrutinize global and segmental ventricular strain changes between genetic and secondary DCM patients.Methods
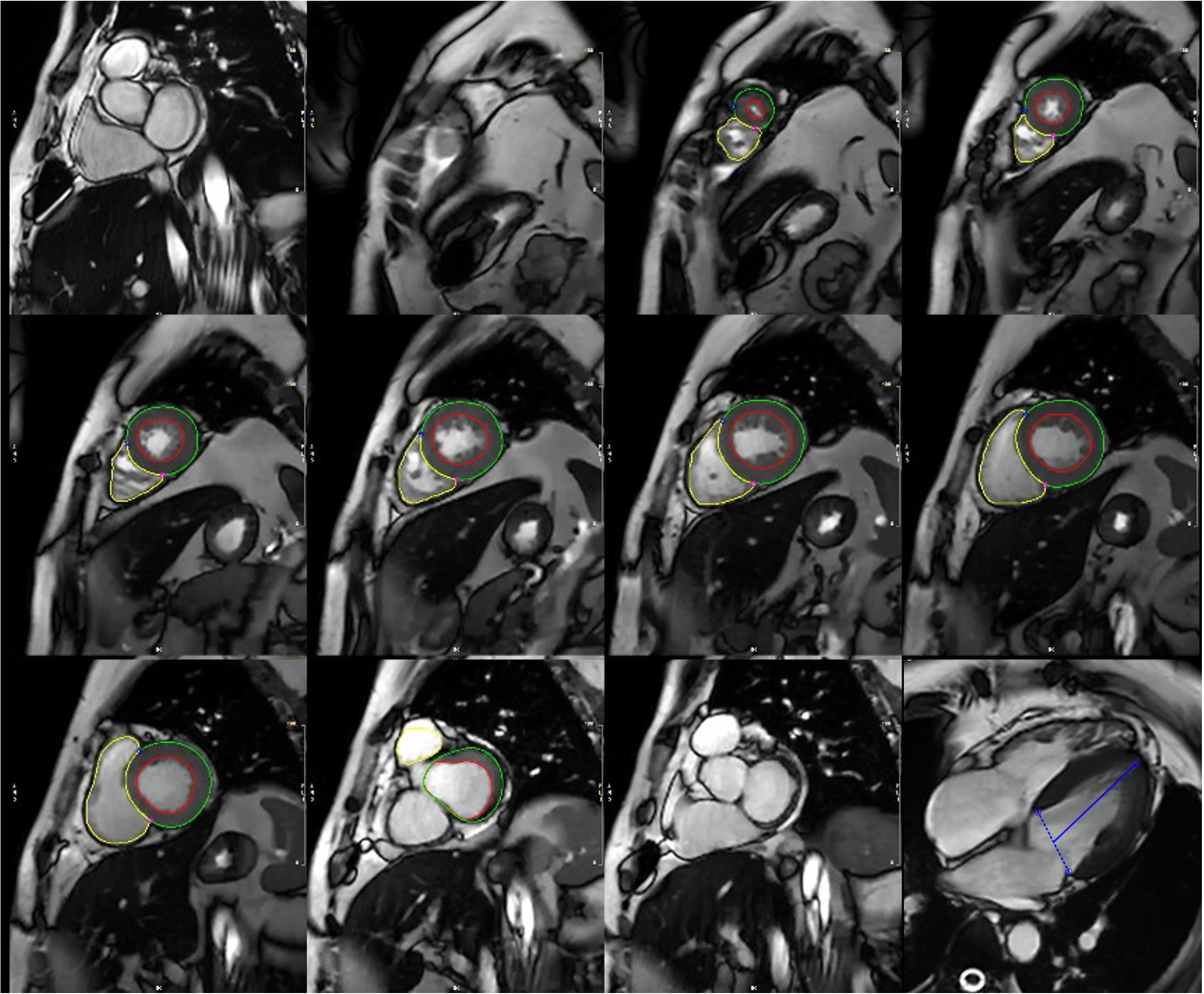
We retrospectively enrolled participants consecutively undergoing CMR between May 2014 and July 2023. CMR examinations were conducted using a 3.0-Tesla scanner (Ingenia; Philips Healthcare, Best, the Netherlands) and analyzed by CVI software (cvi42, Circle Cardiovascular Imaging Inc., Calgary, Alberta, Canada). DCM patients were systematically divided into genetic and secondary groups5. Feature tracking assessed left ventricular myocardial strain parameters, involving manual contouring of endocardial and epicardial borders in end-diastolic images (Figure 1). A deformable model was created from the reference phase, employing a proprietary cost function to determine estimated borders across phases, optimizing the fit via forward and backward approaches by inline module. The software then automatically computed voxel-wise parameters. Statistical analysis utilized IBM SPSS Statistics (version 29.0; SPSS, Chicago, Illinois). Normally distributed continuous variables were compared using Student’s t-test, while non-normally distributed continuous variables were assessed with the Mann-Whitney U test. A P value of <0.05 was deemed statistically significant.Result
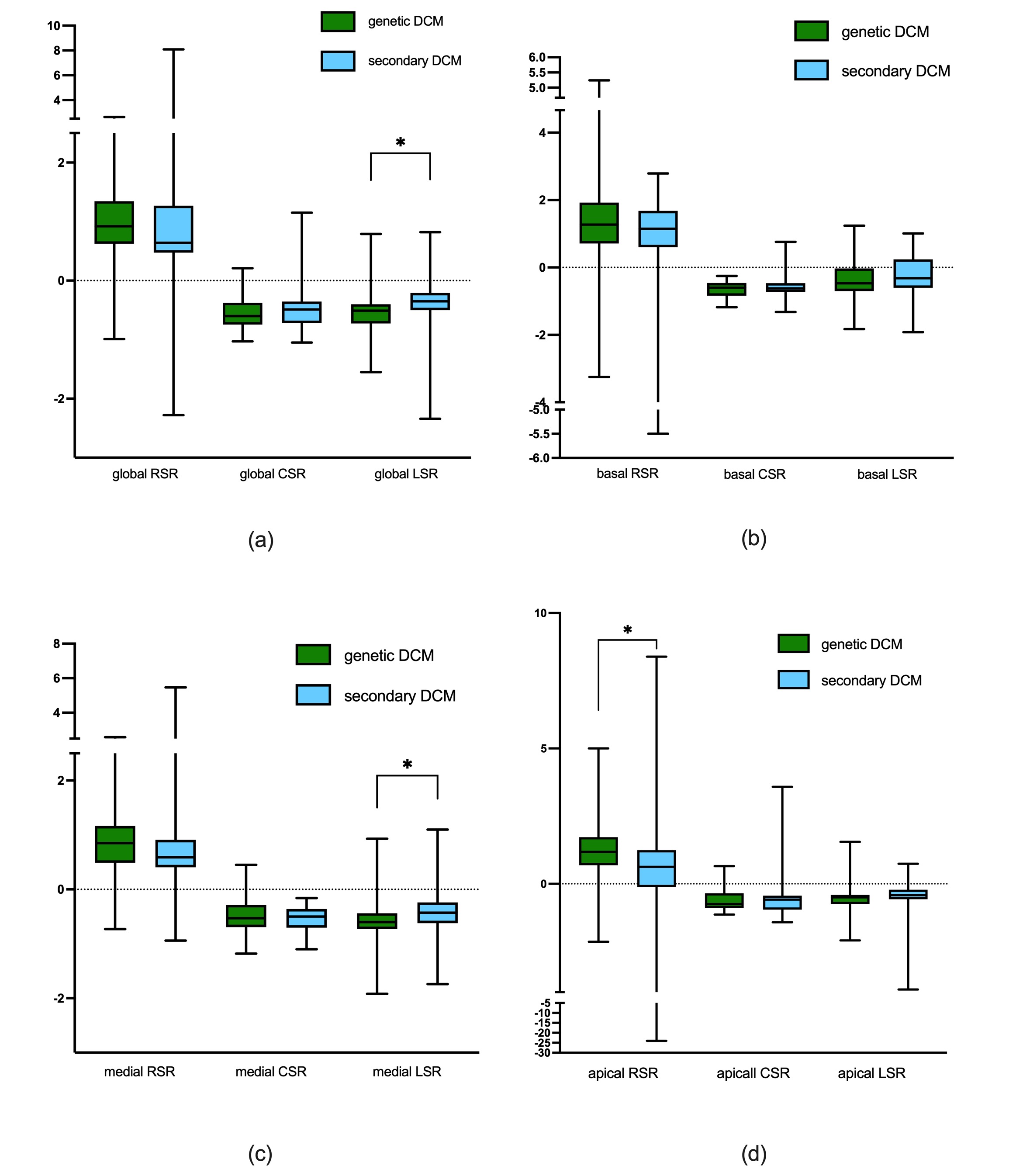
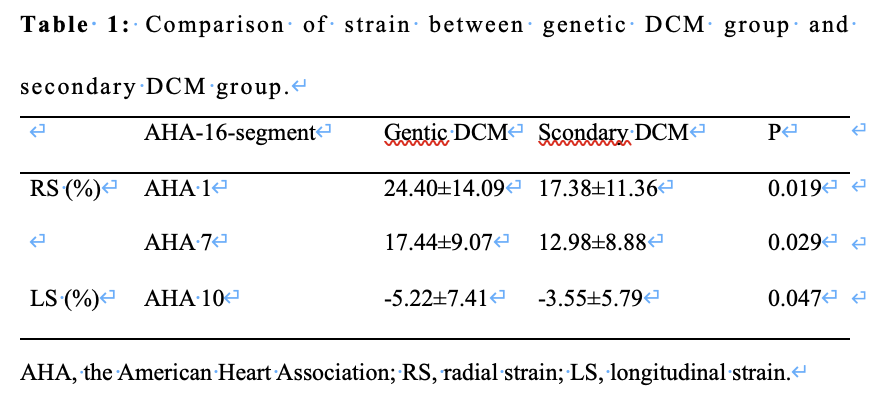
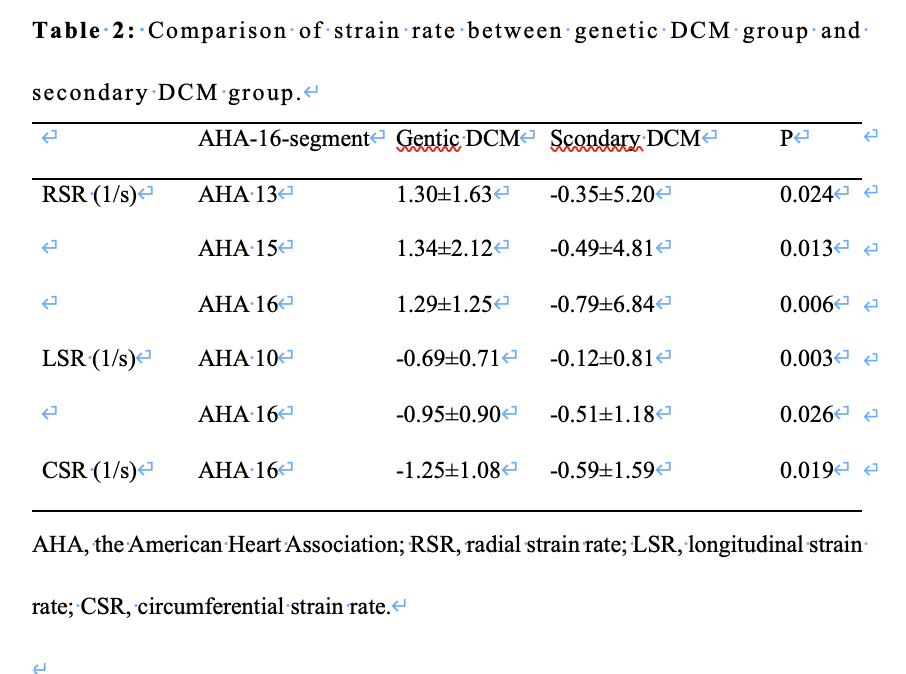
In this study, we enrolled a total of 29 patients with genetic DCM (19.00±11.02 years, 82.76% male) and 33 patients with secondary DCM (26.54±11.99 years, 60.61% male). Compared to individuals with secondary DCM, those with genetic DCM were younger (P < 0.05) and had a comparable gender ratio (P = 0.055). The global radial, circumferential, and longitudinal strain (RS, CS, and LS) of the left ventricle showed no significant differences between the two groups. However, when segmenting the left ventricle according to the 16-segment model proposed by the American Heart Association (AHA), RS in AHA 1 and AHA 7, as well as LS in AHA 10, were significantly impaired in the secondary DCM group compared to the genetic group (P < 0.05) (Table 1). Regarding strain rate, the left ventricle's global longitudinal strain rate (LSR), medial LSR, and apical radial strain rate (RSR) were notably impaired in the secondary group compared to the genetic group (P < 0.05) (Figure 2). Additionally, the secondary group exhibited lower LSR in AHA 10 and 16, lower RSR in AHA 13, 15, and 16, and lower circumferential strain rate (CSR) in AHA 16 (P < 0.05) (Table 2).Discussion
This study elucidates unique strain patterns in genetic and secondary DCM patients, providing valuable insights into their pathophysiological distinctions. Segmentation analysis based on the AHA's 16-segment model revealed significant impairments in RS in AHA 1 and AHA 7, as well as LS in AHA 10, in the secondary DCM group compared to the genetic DCM group. These findings suggest regional heterogeneity in myocardial deformation, influenced by the distinct etiologies of genetic and secondary DCM. Disparities in strain rate parameters, especially lower LSR in AHA 10 and 16, reduced RSR in AHA 13, 15, and 16, and diminished CSR in AHA 16 within the secondary DCM group, contribute to our understanding of complex myocardial mechanics in DCM. These differences may reflect varying disease progression, treatment responses, or genetic predispositions. Clinical relevance lies in the potential for personalized treatment strategies based on identified strain impairments in specific AHA segments, enhancing precision in therapeutic approaches and improving outcomes for DCM patients. Acknowledging study limitations, including sample size and retrospective analysis, future research with larger cohorts and prospective designs is warranted to validate and extend these findings.Conclusion
In conclusion, this study advances our understanding of regional strain variations in genetic and secondary DCM, offering opportunities for targeted therapeutic interventions and improving patient management.Acknowledgements
NoneReferences
1. Orphanou N, Papatheodorou E, Anastasakis A. Dilated cardiomyopathy in the era of precision medicine: latest concepts and developments. Heart Fail Rev. 2022;27(4):1173-1191. doi:10.1007/s10741-021-10139-02. Pan J, Wan Q, Li J, et al. Strain Values of Left Ventricular Segments Reduce Non-homogeneously in Dilated Cardiomyopathy with Moderately and Severely Deteriorated Heart Function Assessed by MRI Tissue Tracking Imaging. Int Heart J. 2018;59(6):1312-1319. doi:10.1536/ihj.17-558
3. Raafs AG, Vos JL, Henkens MTHM, et al. Left Atrial Strain Has Superior Prognostic Value to Ventricular Function and Delayed-Enhancement in Dilated Cardiomyopathy. JACC Cardiovasc Imaging. 2022;15(6):1015-1026. doi:10.1016/j.jcmg.2022.01.016
4. Grothues F, Smith GC, Moon JC, et al. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90(1):29-34. doi:10.1016/s0002-9149(02)02381-0
5. Reichart D, Magnussen C, Zeller T, Blankenberg S. Dilated cardiomyopathy: from epidemiologic to genetic phenotypes: A translational review of current literature. J Intern Med. 2019;286(4):362-372. doi:10.1111/joim.12944
Figures