1654
CMR-based left ventricular strain reflects the therapeutic effect of stem cells in chronic ischemic heart disease1Department of Radiology, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, No. 321 Zhongshan Road, Nanjing, 210008, China., NanJing, China, 2Department of Radiology, Nanjing Central Hospital, No. 116Chengxian Street , Nanjing, 210018 China., NanJing, China, 3Department of Cardio-Thoracic Surgery, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, Jiangsu, 210008, China., NanJing, China, 4Philips Healthcare, Beijing, China, 5Philips Healthcare, Shanghai, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: CMR left ventricular strain analysis is a crucial tool for assessing myocardial status, capable of identifying and evaluating regional myocardial dysfunction caused by coronary artery disease.
Goal(s): This study aims to evaluate the efficacy of cellular therapy in patients with chronic ischemic heart disease using left ventricular strain indices.
Approach: 38 patients scheduled for coronary artery bypass grafting were randomly assigned to receive cellular therapy or serve as controls, followed by CMR imaging and strain analysis of various left ventricular views.
Results: Preliminary results indicate improvements in some CMR-derived strain indices in the cellular therapy group post-treatment, especially notable at 6 months post-operation.
Impact: This study provides new insights into the assessment of cellular therapy efficacy using CMR left ventricular strain indices, offering a more profound understanding and evaluation method for cellular therapy in patients with chronic ischemic heart disease.
Introduction
Cell-based therapies have been validated for safety and feasibility in treating myocardial infarction and ischemic heart disease [1]. These therapies, delivered to the heart through various methods, aim to repair damaged myocardial tissue and stimulate the body’s own healing mechanisms. Cardiac magnetic resonance (CMR) has become an indispensable tool in this context, particularly for evaluating left ventricular strain.Utilizing CMR to monitor changes in left ventricular mechanics offers a non-invasive way to quantify the therapeutic benefits and guide personalized treatment for ischemic heart conditions.Method
The study enrolled patients with chronic ischemic heart disease (CIHD) having a left ventricular ejection fraction (LVEF) ≤ 45%, as determined by three-dimensional echocardiography, who were indicated for coronary artery bypass grafting (CABG) but were ineligible for percutaneous coronary intervention (PCI). Participants were randomly assigned to receive human umbilical cord mesenchymal stem cells (hUC-MSCs) at a dose of 1x108 cells in 2.5 ml of phosphate-buffered saline in conjunction with CABG (cell therapy group), or to undergo CABG alone (control group). During the open-heart procedure, the cells and/or hydrogel were injected at multiple sites—centrally and peripherally within the myocardium—at the end of bypass surgery and before chest closure, between 5 and 10 injections in total. Post-procedure, the patients' cardiac magnetic resonance (CMR) images were analyzed for left ventricular strain using software from Medis Medical Imaging Systems, based in Leiden, the Netherlands. The analysis focused on feature-tracking measurements of the left ventricle, including two-chamber, three-chamber, and four-chamber views. This comprehensive approach allows for the evaluation of both regional and global myocardial mechanical function, offering insights into the effectiveness of stem cell therapy in conjunction with surgical intervention.Results
Changes in Cardiac Strain Indicators Post-TreatmentAfter the treatment, there was an observable increase in the mean values of multiple cardiac magnetic resonance-derived strain indicators in both the stem cell-treated (cell group) and the control group. At the 6-month follow-up, the cell group showed a more pronounced trend of improvement across several strain parameters, although no significant differences between the two groups were evident. Specifically, for SAXEndoGCS, SAXGRS, LAXMyoGCS, LVMyoGLS, LAXEndoGCS, LVEndoGLS, LAXGRS, and ApexBase, the confidence intervals (95% CI) and P-values did not demonstrate statistical significance (P > 0.05 for all mentioned parameters).
Significant Within-Group Differences in LVEF and Left Ventricular Strain Parameters
Comparing pre-treatment and post-treatment changes within each group revealed significant differences in the left ventricular ejection fraction (LVEF) and some left ventricular strain parameters in the cell group at both 3 and 12 months post-operation. The cell group exhibited significant improvements in SAXEndoGCS at both 3 and 12 months (P = 0.013 and P = 0.002, respectively) and in SAXmyoGCS at the same time points (P = 0.016 and P = 0.006, respectively). Additionally, LAXMyoGLS also showed significant improvement within the cell group at 3 and 12 months (P = 0.018 and P = 0.029, respectively), while LVEndoGLS indicated significant improvement at 3 months post-treatment (P = 0.008). Conversely, the control group did not exhibit statistically significant changes at these time points. In terms of LVEF, there were notable improvements in the cell group at 3 and 12 months (P = 0.009 and P = 0.001, respectively), in contrast to the control group, which did not demonstrate statistically significant changes (P = 0.141 at 3 months and P = 0.369 at 12 months).
Discussion
This study investigated the impact of stem cell therapy on cardiac function. Our findings indicate that within the first 6 months post-treatment, there was an observable increase in several cardiac strain indices derived from magnetic resonance imaging in the treatment group, with the cell group showing a more pronounced improvement trend than the control group. However, the differences between the groups were not statistically significant. These observations align with previous studies that have reported similar outcomes [2-4]. At the 12-month mark, these differences appeared to dissipate, suggesting that cardiac function between the two patient groups may converge or the effect of the treatment on both groups may diminish. These findings suggest that the initial benefits of stem cell therapy, as observed through improvements in strain parameters, might not be sustained over a more extended period, at least in a manner detectable by the current study design and methods.Conclusion
Our findings may have clinical significance in understanding the impact of stem cell therapy on cardiac function across different patient populations, aiding in the formulation of future therapeutic strategies and personalized treatment approaches.Acknowledgements
No acknowledgement found.References
- He, X., Wang, Q.,Zhao, Y., Zhang, H., Wang, B., Pan, J., Li, Jie., Yu. H., Wang, L., Dai, J. *, Wang, D. *, Effect ofIntramyocardial Grafting Collagen Scaffold With Mesenchymal Stromal Cells inPatients With Chronic Ischemic Heart Disease: A Randomized Clinical Trial. JAMA Network Open. 2020; 3(9):e2016236.
- Bartunek J, Terzic A, Davison BA, et al; CHART Program. Cardiopoietic cell therapy for advanced ischaemic heart failure: results at 39 weeks of the prospective, randomized, double blind, sham-controlled CHART-1 clinical trial. Eur Heart J. 2017;38(9):648-660. doi:10.1093/eurheartj/ehw543.
- Gyöngyösi M, Wojakowski W, Navarese EP, Moye LÀ; ACCRUE Investigators. Meta-analyses of human cellbased cardiac regeneration therapies: controversies in meta-analyses results on cardiac cell-based regenerative studies. Circ Res. 2016;118(8):1254-1263. doi:10.1161/CIRCRESAHA.115.307347 .
- Gyöngyösi M, Wojakowski W, Lemarchand P, et al; ACCRUE Investigators. Meta-analysis of cell-based cardiac studies (ACCRUE) in patients with acute myocardial infarction based on individual patient data. Circ Res. 2015; 116(8):1346-1360. doi:10.1161/CIRCRESAHA.116.304346.
Figures
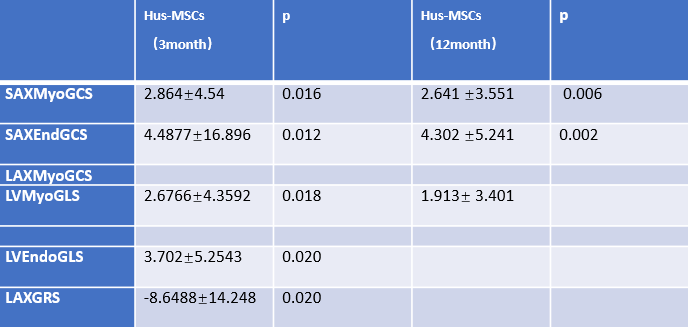
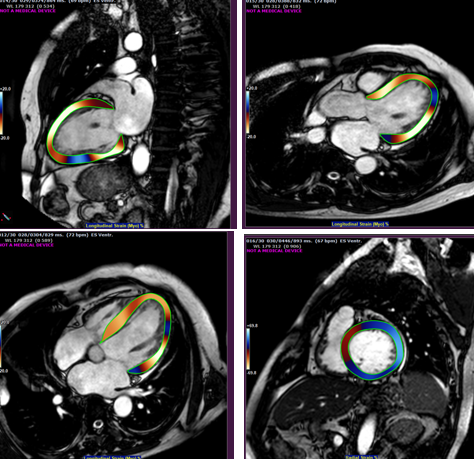
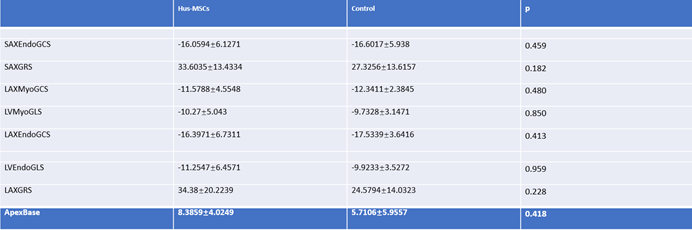
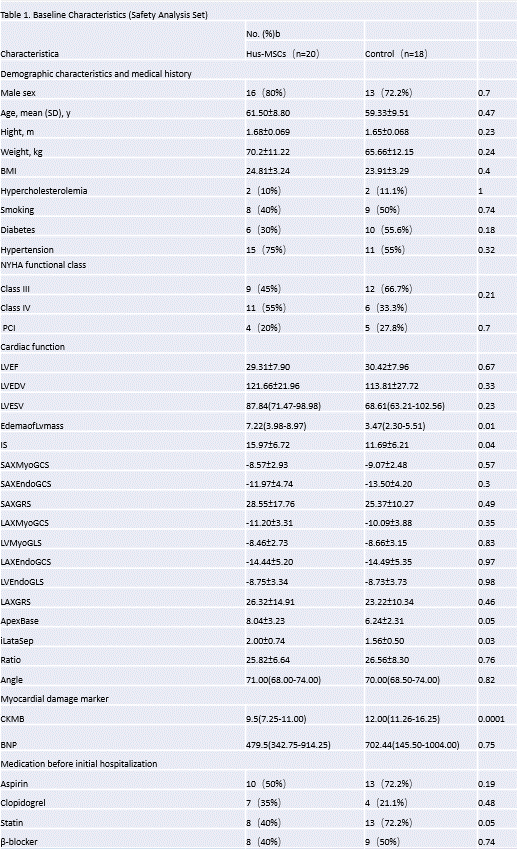
Table 1.Baseline Characteristics (Security Analysis Set)
Abbreviation: ACE inhibitor, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blockers; CK-MB, creatine kinase-myocardial band; CMR, Cardiac Magnetic Resonance Imaging; cTnT, cardiac troponin T; hUC-MSC, human umbilical cord derived mesenchymal stromal cells; IQR, interquartile range; Left ventricle, left ventricle ejection fraction; NYHA, New York Heart Association; PCI, percutaneous coronary artery Intervention. aAll values Unless otherwise stated, they are expressed in numbers and percentages. Median and IQR It is given for values that are unevenly distributed. CB is calculated by weight Divide the height in kilograms by meters squared.