1650
Prognostic Value of Global and Segmental LV Myocardial Strain Parameters Derived from CMR-FT Technique in AL-CA Patients: A Pilot Study.1Peking University First Hospital, Peking, China, 2Philips Healthcare, Peking, China
Synopsis
Keywords: Myocardium, Myocardium
Motivation: Early detection of cardiac involvement and continuous monitoring of disease progression could benefit patients with light-chain amyloidosis. The application of left ventricular strain by Cardiac magnetic resonance feature tracking imaging has emerged as an excellent noninvasive imaging modality.
Goal(s): This study is dedicated to exploring the prognostic implications of myocardial strain in distinct myocardial segments.
Approach: The assessment of both global and segmental myocardial strain was conducted through the application of steady-state free precession (SSFP) cine sequences.
Results: Global radial strain (RSglobal), RS in the basal lateral segment (RSbas-lateral) and B-type natriuretic peptides (BNP) are independently associated with all-cause mortality.
Impact: Quantification of LV strain could be employed to monitor the progression of amyloid light-chain (AL) amyloidosis. Global radial strain and radial strain in the basal lateral segment may prove valuable for risk stratification in patients with AL amyloidosis.
Introduction
Amyloidosis is characterized by systemic amyloid deposition, with light-chain amyloidosis being common and impacting multiple organs1,2. Cardiac involvement is a critical factor in patient survival3. Cardiac Magnetic Resonance (CMR) has emerged as a valuable modality for diagnosing and predicting outcomes in patients with cardiac amyloidosis. Feature tracking (CMR-FT) has gained prominence due to its simplicity and reliability in quantifying left ventricular (LV) strain using SSFP sequences4. Notably, myocardial strain has demonstrated superior prognostic value in specific clinical contexts involving patients with AL-CA5. Despite advancements, the research on prognostic implications of myocardial strain in various segments of cardiac amyloidosis remains limited.Methods
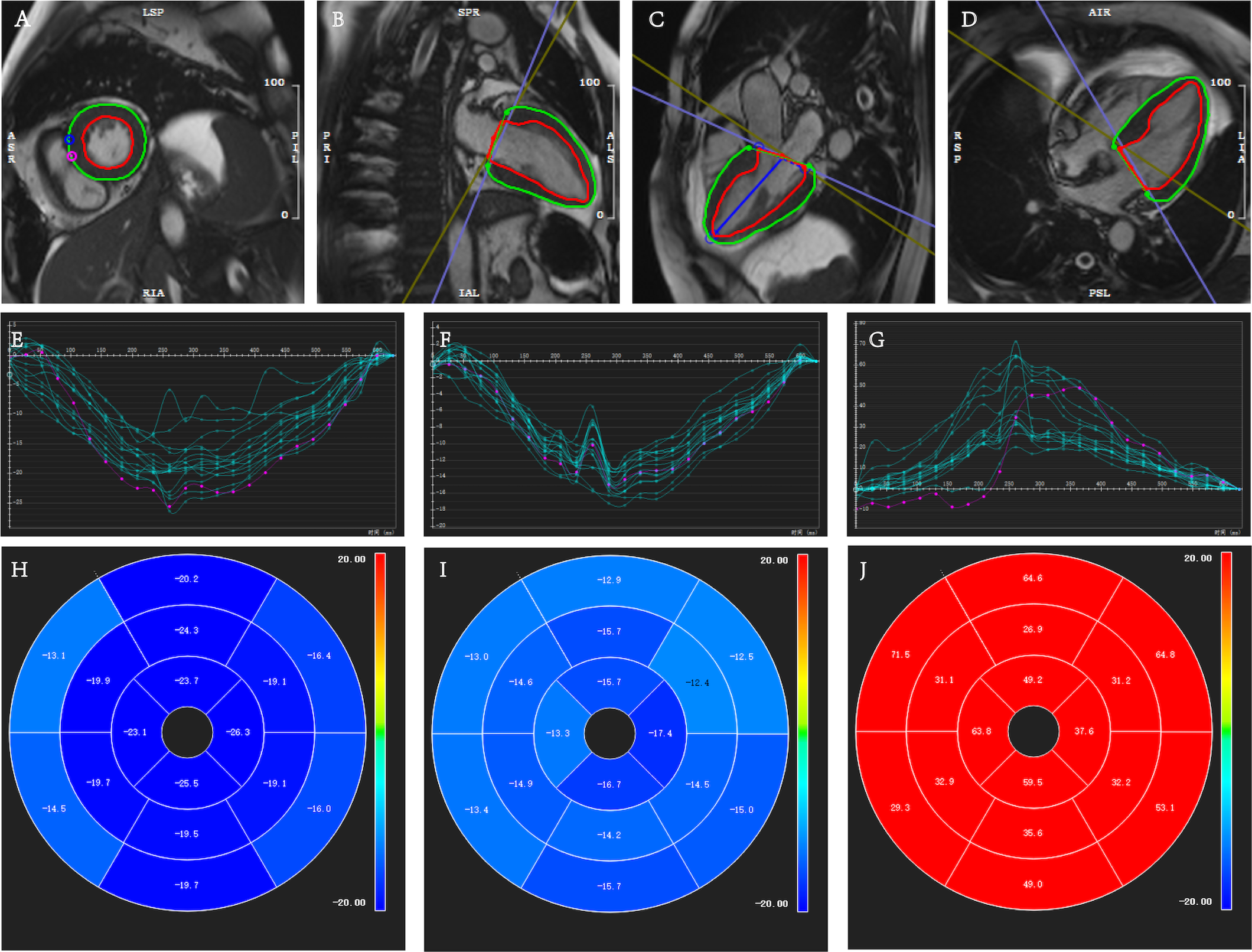
Seventy-five consecutive patients, comprising 50 males with an average age of 55.6 ± 10.0 years, who had undergone CMR examinations and were histologically confirmed to have systemic AL-CA, were enrolled from January 2014 to November 2022. CMR scans were performed using both 3.0-T scanners (Philips Ingenia, GE Discovery MR750, SIEMENS MAGNETOM Prisma) and 1.5-T scanners (SIEMENS MAGNETOM Aera), employing either cardiac or abdominal coils. Subsequently, CMR images were imported into CVI42 v5.14.2 software for in-depth analysis.To assess myocardial function, global and segmental longitudinal strain (LS), circumferential strain (CS), and radial strain (RS) of the left ventricle were quantified using SSFP cine sequences. This analysis including the basal, middle, and apical segments, in line with the American Heart Association's 16-segment model for segmental myocardial motion evaluation (Figure 1). The period between the CMR examination date and the occurrence of a patient's demise was regarded as the event time, divided into survivors and non-survivors groups. The prognostic significance of LV strain parameters was assessed using Cox proportional hazards regression and visually depicted through Kaplan–Meier curves.
Results
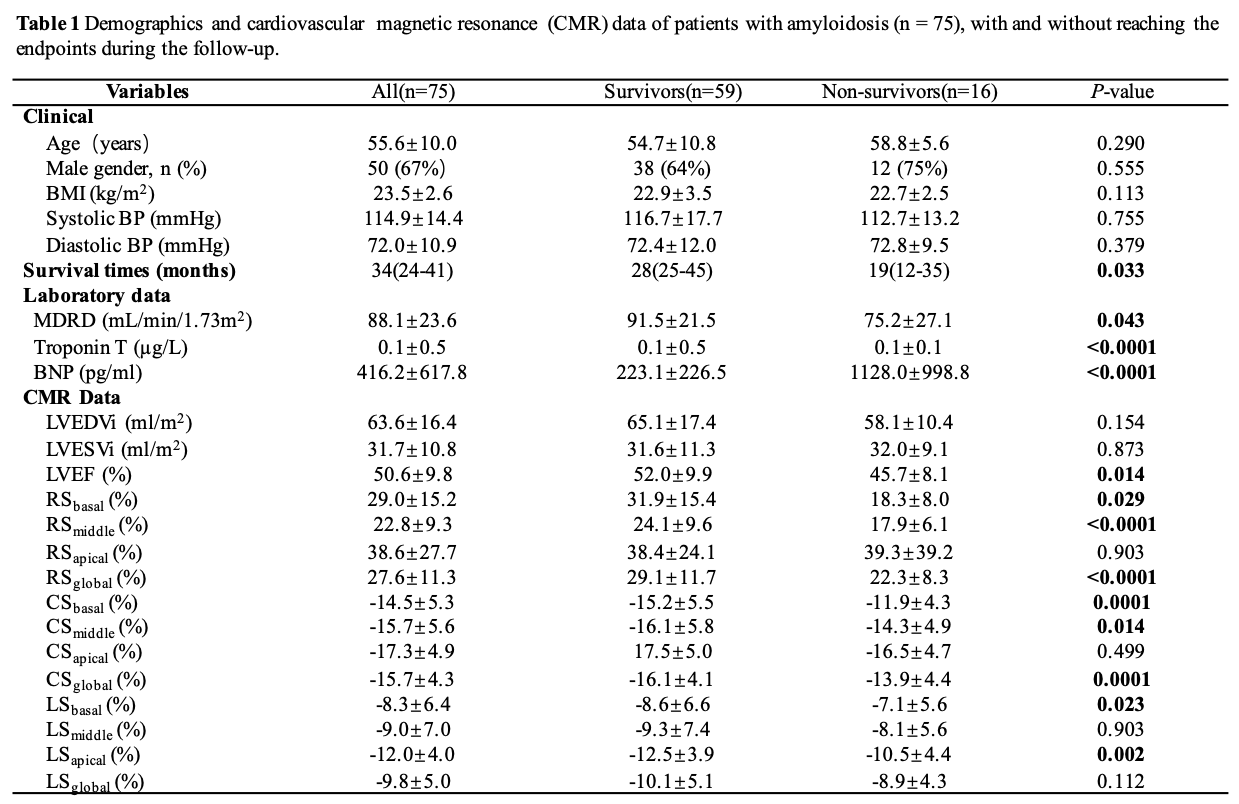
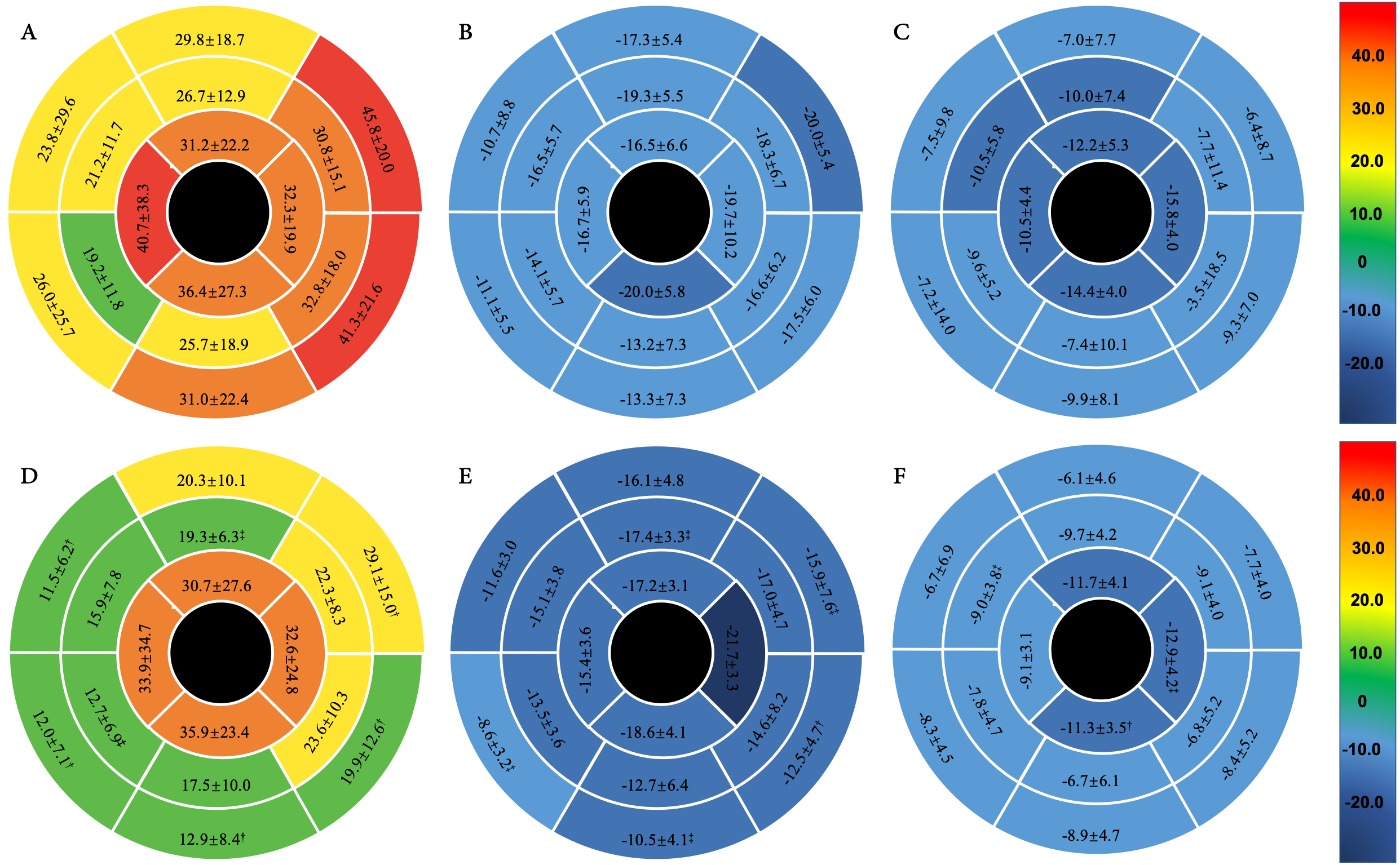
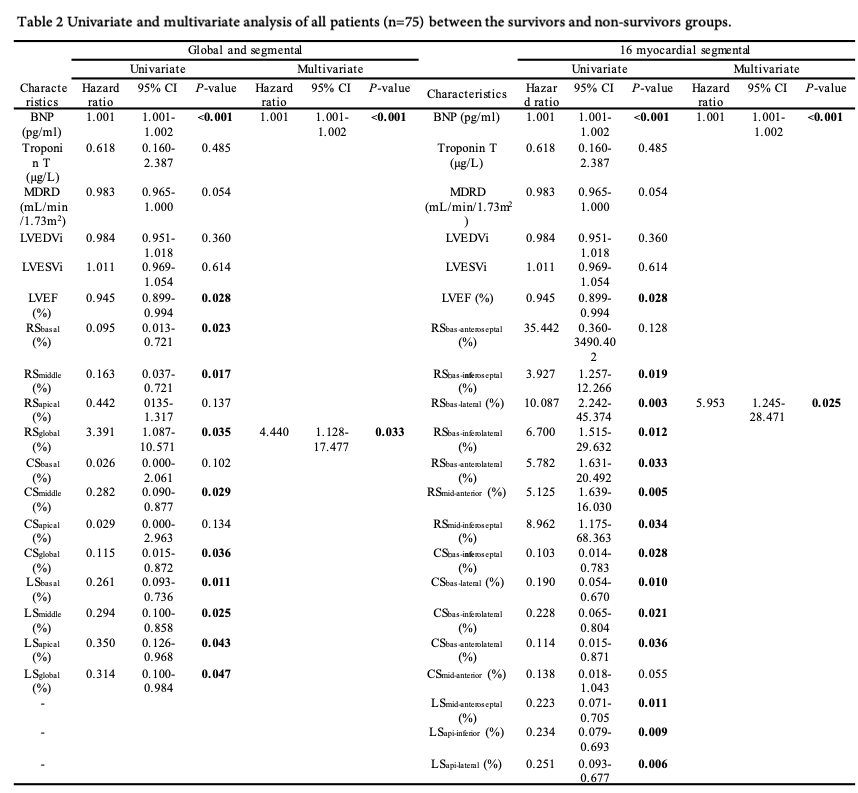
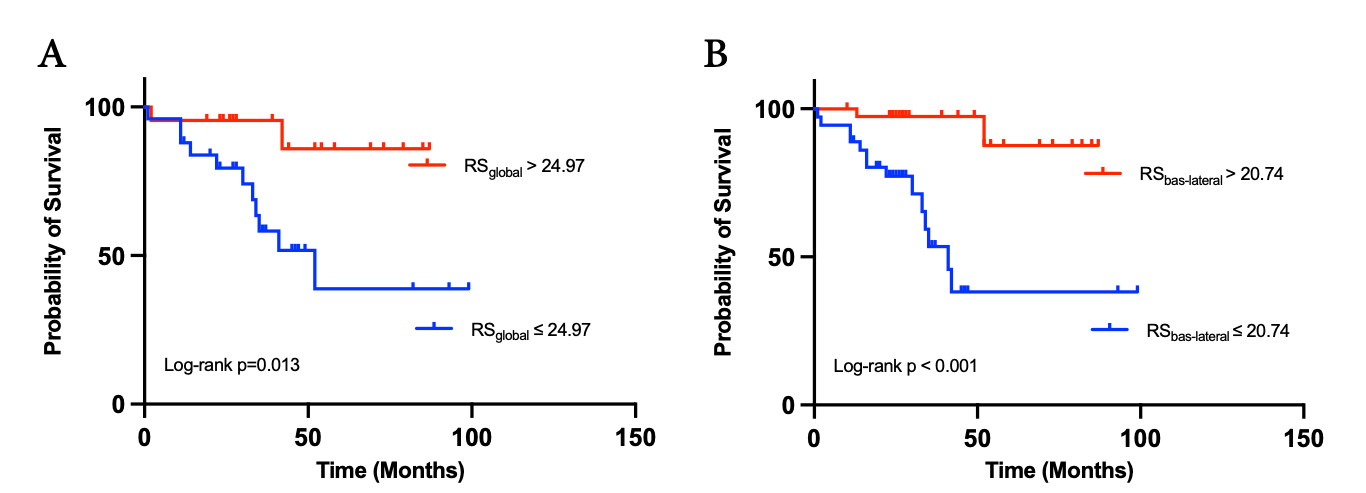
After a median follow-up period of 34 months, 16 out of 75 patients reached the endpoint of mortality, who classified into survivor and non-survivor groups. Baseline and CMR characteristics of patients with AL amyloidosis were summarized in Table 1. Among these patients, there was a notable change in LV strain parameters when compared survivor with non-survivor groups, including RSglobal, CSglobal, RSbasal, RSmiddle, CSbasal, CSmiddle, LSbasal, and LSapical, P < 0.05 for all (Table 1). Furthermore, significant variations in strain measurements were observed within specific myocardial segments (Figure 2).In a multivariate Cox analysis, BNP (hazard ratio, 1.001; 95% CI: 1.001, 1.002; p < 0.001), RSglobal (hazard ratio, 4.440; 95% CI: 1.128, 17.477; p = 0.003), and RS in the basal lateral segment (RSbas-lateral) (hazard ratio, 5.953; 95% CI: 1.245, 28.471; p = 0.025) remained significant as independent predictors of all-cause mortality (Table2). The cut-off values were identified as 354.5 for BNP, 24.97% for RSglobal, and 20.97% for RSbas-lateral. After categorizing AL patients into two groups by using the defined cut-off values, Kaplan-Meier survival curves revealed significantly reduced event-free survival for individuals in the lower cut-off groups for RSglobal and RSbas-lateral (P = 0.013, P < 0.001, respectively) (Figure 3).
Discussion
In patients who reached the study endpoint, notable alterations in myocardial strain patterns were observed, characterized by reduced radial strain coupled with increased circumferential and longitudinal strains in the basal myocardial segments. These findings corroborate existing research in the field6,7. Moreover, distinctions in radial and circumferential strains at the apical segments between survivors and non-survivors were relatively minimal, with the exception of longitudinal strains. It is evident that basal segments are more susceptible to involvement, and the change in strains in these segments may serve as an early indication of amyloid infiltration8,9. Intriguingly, significant disparities in segmental strains across the 16 myocardial segments were identified between the two groups, with a pronounced emphasis on the septal and lateral walls, necessitating further exploration of the underlying mechanisms. The study's results unveiled the independent associations of RSglobal, RSbas-lateral, and BNP with all-cause mortality. RSglobal, reflecting myocardial fiber deformation toward the heart's central cavity, exhibited a correlation with changes in myocardial fiber thickness10. The novel contribution of this study lies in the potential utility of RSbas-lateral for risk stratification in AL amyloidosis patients. This suggests that the lateral wall might be particularly susceptible to experiencing early or intensified pathological structural and functional changes11. Nonetheless, the comprehensive mechanistic understanding of this phenomenon remains to be elucidated. Consequently, it is important to highlight that the measurement of RSbas-lateral remains a valuable approach for routine assessment of AL-CA prognosis.Conclusions
Global radial strain and radial strain in the basal lateral segment, assessed through CMR, exhibit potential as noninvasive markers for independently predicting all-cause mortality in AL amyloidosis patients.Acknowledgements
NoneReferences
1. Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. The Lancet 2016;387(10038):2641-2654.2. Giampaolo M, Giovanni P. Light chain amyloidosis: the heart of the problem. Haematologica 2013;98(10):1492-1495.
3. Falk RH, Alexander KM, Liao R, Dorbala S. AL (Light-Chain) Cardiac Amyloidosis: A Review of Diagnosis and Therapy. Journal of the American College of Cardiology 2016;68(12):1323-1341.
4. Chirinos JA, Sardana M, Ansari B, et al. Left Atrial Phasic Function by Cardiac Magnetic Resonance Feature Tracking Is a Strong Predictor of Incident Cardiovascular Events. Circulation: Cardiovascular Imaging 2018;11(12):e007512.
5. Faganello G, Collia D, Furlotti S, et al. A new integrated approach to cardiac mechanics: reference values for normal left ventricle. The International Journal of Cardiovascular Imaging 2020;36(11):2173-2185.
6. Li R, Yang Z-g, Wen L-y, et al. Regional myocardial microvascular dysfunction in cardiac amyloid light-chain amyloidosis: assessment with 3T cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance 2016;18(1):16.
7. Wan K, Sun J, Yang D, et al. Left Ventricular Myocardial Deformation on Cine MR Images: Relationship to Severity of Disease and Prognosis in Light-Chain Amyloidosis. Radiology 2018;288(1):73-80.
8. Baccouche H, Maunz M, Beck T, et al. Differentiating Cardiac Amyloidosis and Hypertrophic Cardiomyopathy by Use of Three-Dimensional Speckle Tracking Echocardiography. Echocardiography 2012; 29 (6): 668-677.
9. Ternacle J, Bodez D, Guellich A, et al. Causes and Consequences of Longitudinal LV Dysfunction Assessed by 2D Strain Echocardiography in Cardiac Amyloidosis. JACC: Cardiovascular Imaging 2016; 9 (2): 126-138.
10. Wu Y, Pu C, Zhu W, et al. A Risk Score to Diagnose Cardiac Involvement and Provide Prognosis Information in Patients at Risk of Cardiac Light-Chain Amyloidosis. Frontiers in Cardiovascular Medicine 2022; 9.
11. Kermer J, Traber J, Utz W, et al. Assessment of diastolic dysfunction: comparison of different cardiovascular magnetic resonance techniques. ESC Heart Failure 2020; 7 (5): 2637-2649.
Figures