1649
Association of serum uric acid with right cardiac chamber remodeling assessed by CMR-feature tracking in patients with connective tissue disease1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Synopsis
Keywords: Myocardium, Cardiovascular, Connective tissue disease, Serum uric acid, Hypouricemia, Cardiovascular resonance magnetic imaging, Feature tracking, Right atrial strain.
Motivation: To explore a common and low-cost indicator in patients with connective tissue disease (CTD) to determine the subclinical right cardiac chamber remodeling
Goal(s): Investigated the association of Serum uric acid (SUA) with right cardiac chamber remodeling assessed by cardiac magnetic resonance feature-tracking (CMR-FT) in CTD patients.
Approach: All individuals underwent CMR examinations and their SUA levels were recorded. CMR-FT was used to evaluate the right atrial and ventricular strain parameters.
Results: CTD patients had significantly right cardiac chamber remodeling and elevated SUA levels compared with controls. SUA may be a potential risk factor of right cardiac chamber remodeling in CTD patients.
Impact: Right heart remodeling is widespread in CTD patients. SUA is considered a potential independent risk factor for cardiovascular disease and elevated SUA levels are often observed in CTD patients.
Introduction
Given the potential impact of common complications like interstitial lung disease and pulmonary hypertension (PH) on right ventricular (RV) afterload and primary myocardial involvement, right cardiac chamber remodeling is widespread and plays an important role in the disease progression and prognosis in patients with connective tissue disease (CTD). Cardiac magnetic resonance feature-tracking (CMR-FT) is a promising technique that evaluates myocardial deformation and provides additional information for subclinical cardiac dysfunction1. Thus, right atrial (RA) and ventricular strain parameters may be more sensitive to assess the changes in right heart function and mechanics. Serum uric acid (SUA) is correlated with multiple cardiovascular risk factors and be considered an independent predictor for several adverse cardiovascular outcomes2. Previous studies demonstrated that elevated SUA level was a potential risk factor of cardiovascular damage in patients with CTD3,4. Elevated SUA levels not only increase the risk of developing PH and serve as a marker for screening PH in CTD5,6, but may also be predictors of clinical prognosis in patients with CTD-associated pulmonary arterial hypertension7. The present study aimed to evaluate the right cardiac chamber remodeling in patients with CTD and to investigate the association of SUA with impaired RV and RA strain parameters assessed by cardiac magnetic resonance feature-tracking.Methods
We consecutively and retrospectively recruited 104 patients with CTD and 40 age- and sex-matched healthy controls. All individuals underwent CMR imaging and measured SUA levels. Patients were divided into three subgroups based on the tertiles of SUA level in the present study. CMR-FT was used to evaluate the RA longitudinal strain and strain rate (SR) parameters as well as RV global systolic peak strain and strain rate in longitudinal and circumferential directions for each subject. Univariable and multivariable linear regression analyses were used to explore the association of SUA with RV and RA strain parameters.results
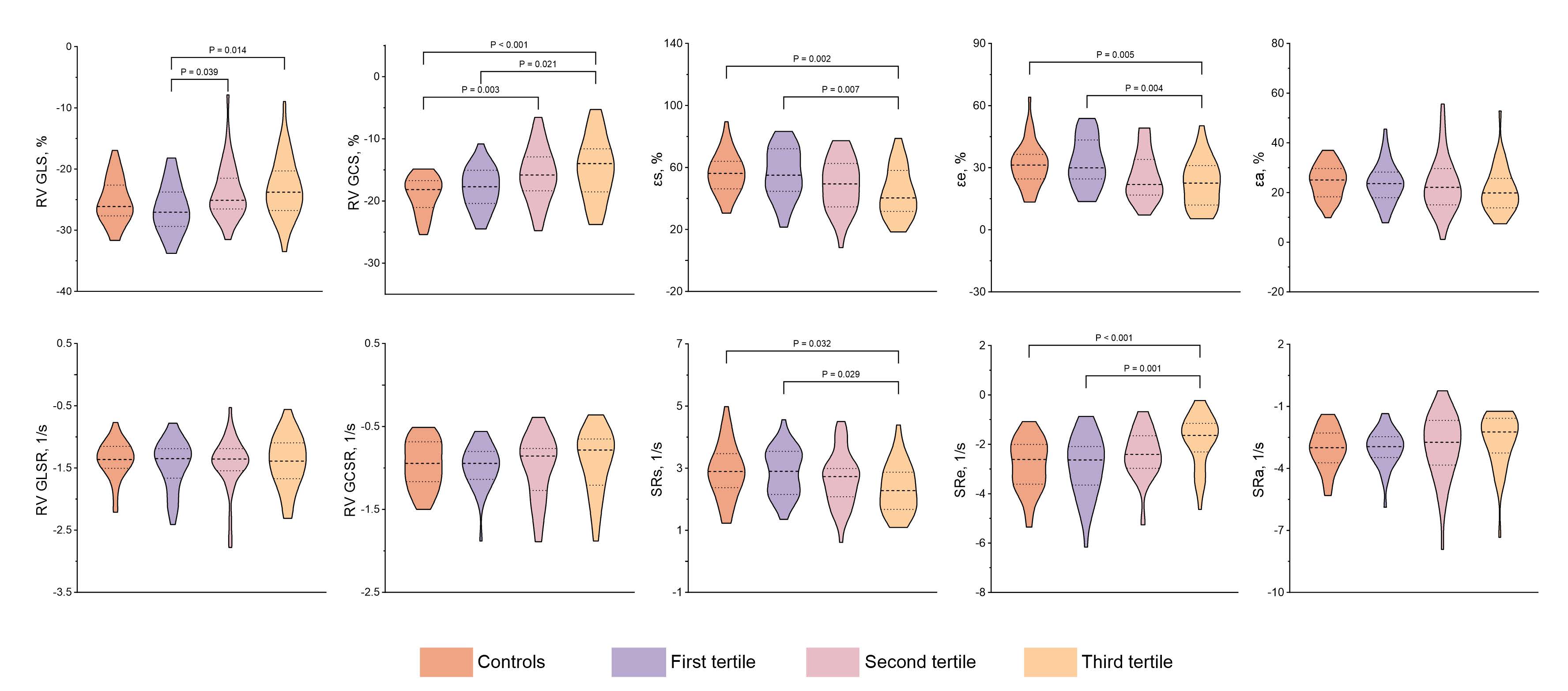
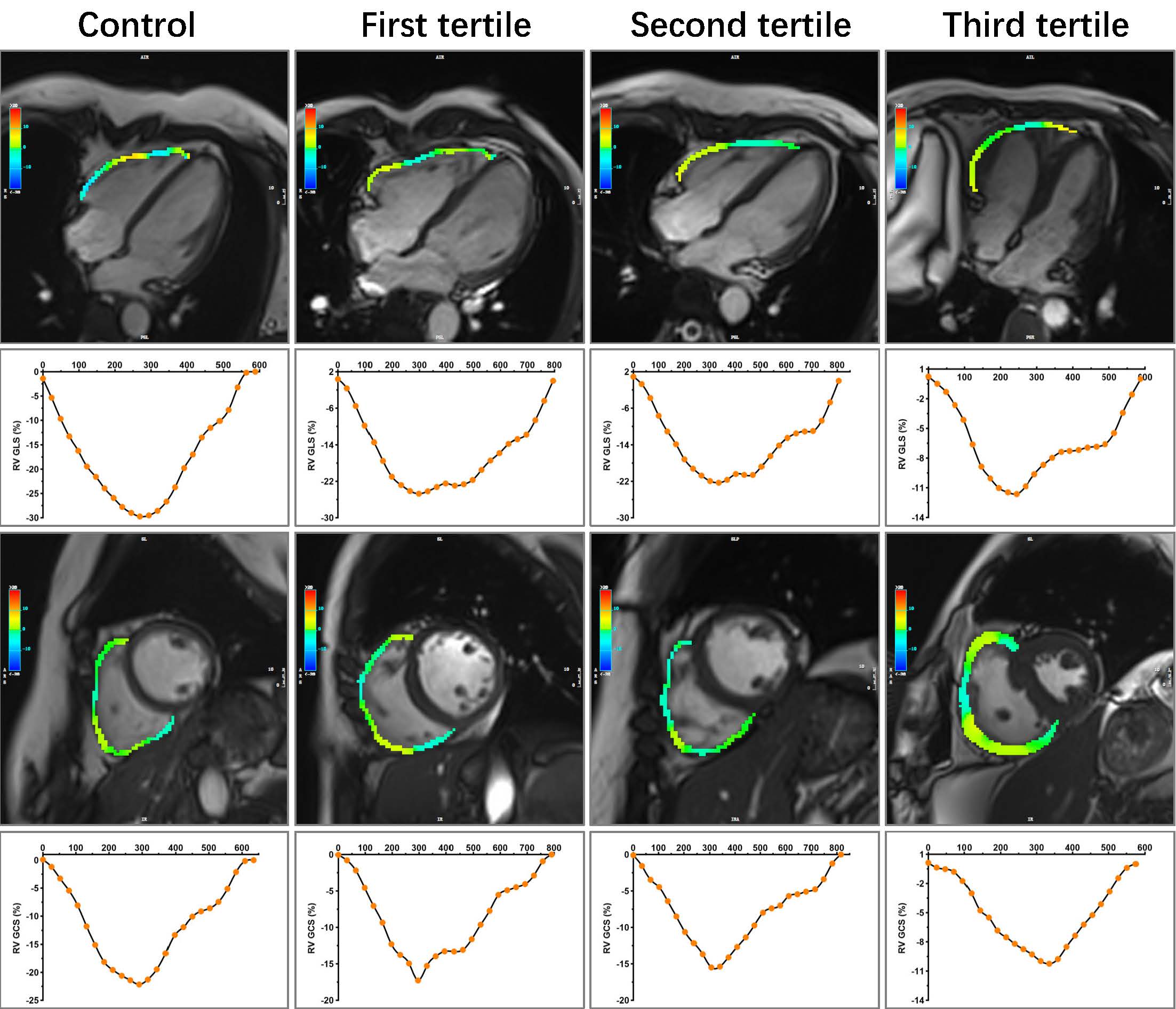
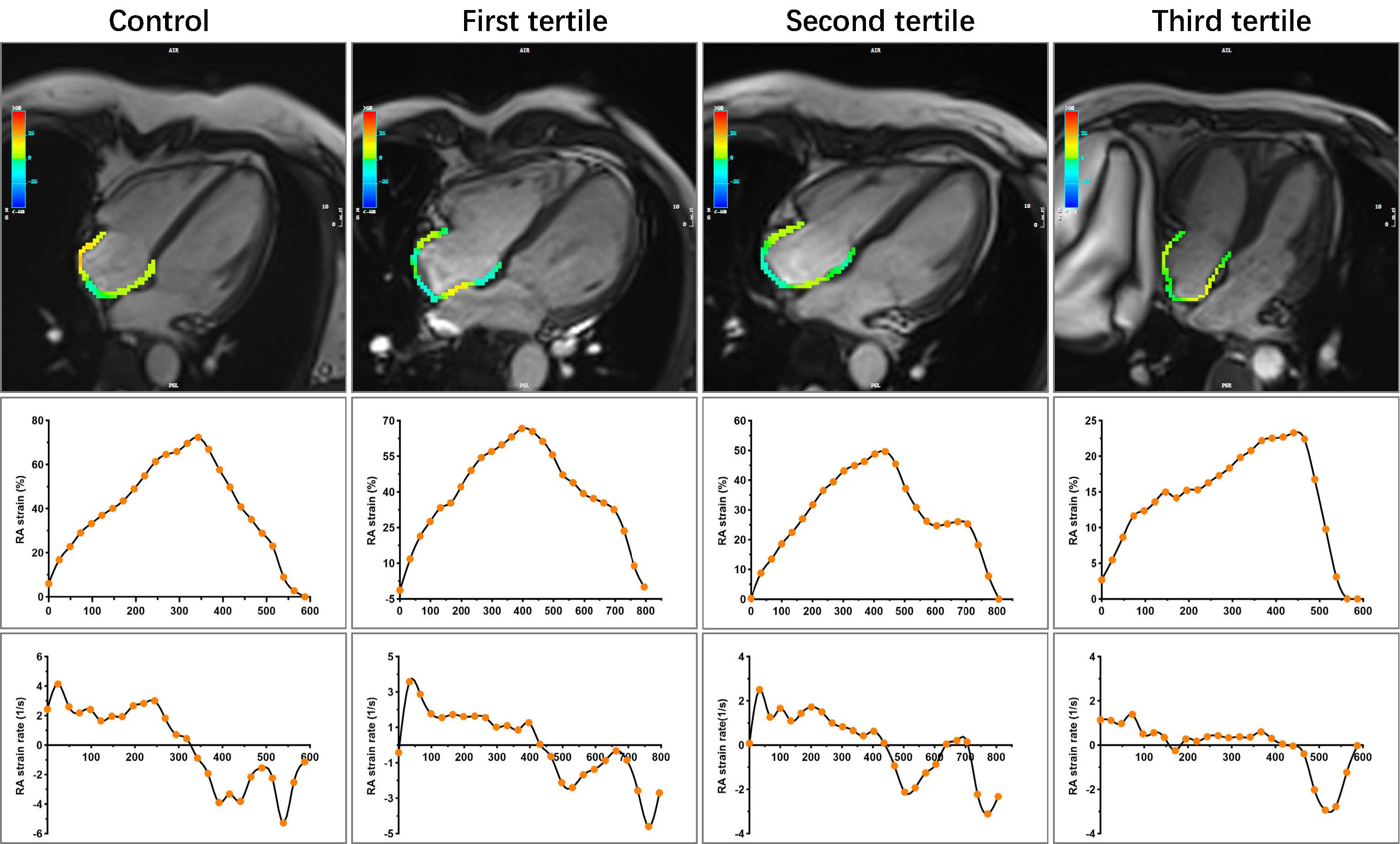
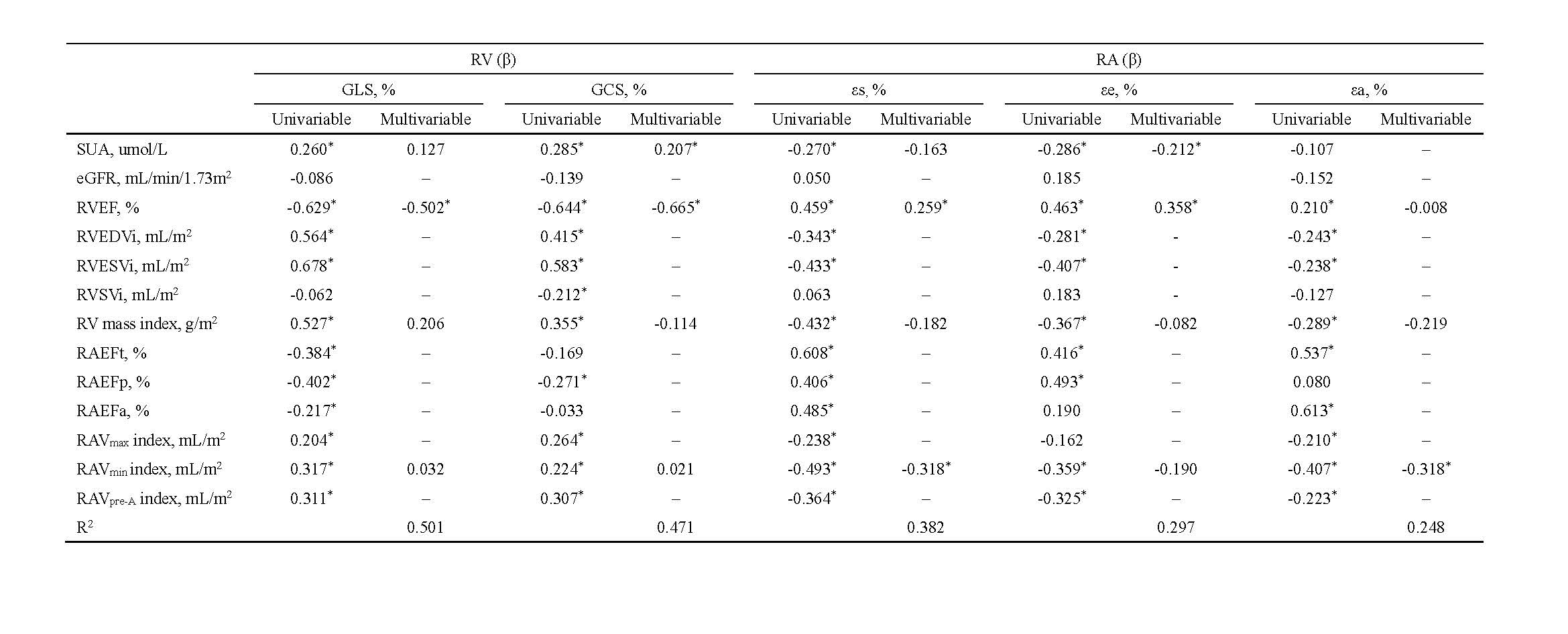
CTD patients had significantly higher SUA levels (308.5 [249.00, 357.800] vs. 265.00 [230.00, 297.60], P=0.002) and lower RA reservoir strain (εs), conduit strain (εe), conduit strain rate (SRe), as well as RV global circumferential strain (RV GCS) (all P<0.05) than healthy controls even when RA volume and ejection fraction is normal. Among subgroups, patients in the third tertile had significantly impaired RV global longitudinal strain (RV GLS), RV GCS, as well as RA reservoir and conduit strain parameters compared with those in the first tertile (all P<0.05)(Figure 1-3). The elevated SUA levels were correlated with impaired RV GLS, RV GCS, as well as RA reservoir and conduit strain and strain rates (absolute value of β= 0.250 to 0.293, all P<0.05). In multivariable linear regression analysis, the SUA level still was an independent determinant of εe (β=-0.212, P=0.035) and RV GCS (β=0.207, P=0.019)(Figure 4).Discussion
The elevated SUA levels may lead to right cardiac chamber remodeling by promoting the increased RV afterload in patients with CTD. Several studies found the SUA levels were significantly higher in CTD patients with PH than in those without PH 6,8,9. In CTD-PAH, the baseline SUA levels also had a positive correlation with pulmonary vascular resistance (PVR) and steady hyperuricemia may predict a worsen clinical prognosis 7. The elevated SUA level may promote pulmonary vascular remodeling through increased oxidative stress, depletion of nitric oxide, endothelial dysfunction, vasoconstriction and proliferation of vascular smooth muscle cells 2. In addition, inflammation may play a key role between elevated uric acid and right heart remodeling. Elevated SUA levels may enhance the inflammatory response and thus affect right cardiac chamber remodeling in patients with CTD. Even though SSc-PAH patients have similar PVR with idiopathic pulmonary hypertension patients, there was a worse RV function and prognosis in the former 10, the primary myocardial involvement derived by inflammation may be one of the potential causes 11. However, none of these mechanisms are independent. They reinforce and interact with each other, ultimately leading to right cardiac chamber remodeling.Conculsion
Patients with CTD had significantly higher SUA levels and more severe right cardiac chamber remodeling than controls. SUA may be a potential risk factor of right cardiac chamber remodeling and is independently associated with impaired εe and RV GCS in patients with CTD.Acknowledgements
Thanks to Ms Jinyang Wen for the measurement of parameters derived by CMR-FT. Thanks to Ms Zhoxia Yang who provided a professional statistical analysis method. Thanks to Dr Lu Huang and Dr Liming Xia who provided the idea of this retrospective study.References
1. Xu J, Yang W, Zhao S, et al. State-of-the-art myocardial strain by CMR feature tracking: clinical applications and future perspectives. Eur Radiol 2022;32(8): 5424-5435.
2. Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta 2018;484150-163.
3. Elera-Fitzcarrald C, Reategui-Sokolova C, Gamboa-Cardenas RV, et al. Serum uric acid is associated with damage in patients with systemic lupus erythematosus. Lupus Sci Med 2020;7(1): e000366.
4. Zou YW, Li QH, Zhu YY, et al. Prevalence and influence of hypouricemia on cardiovascular diseases in patients with rheumatoid arthritis. Eur J Med Res 2022;27(1): 260.
5. Castillo-Martínez D, Marroquín-Fabián E, Lozada-Navarro AC, et al. Levels of uric acid may predict the future development of pulmonary hypertension in systemic lupus erythematosus: a seven-year follow-up study. Lupus 2016;25(1): 61-66.
6. Kim KJ, Baek IW, Park YJ, et al. High levels of uric acid in systemic lupus erythematosus is associated with pulmonary hypertension. Int J Rheum Dis 2015;18(5): 524-532.
7. Wang J, Wang Y, Li X, et al. Serum uric acid is associated with disease severity and may predict clinical outcome in patients of pulmonary arterial hypertension secondary to connective tissue disease in Chinese: a single-center retrospective study. BMC Pulm Med 2020;20(1): 272.
8. Chikhoune L, Brousseau T, Morell-Dubois S, et al. Association between Routine Laboratory Parameters and the Severity and Progression of Systemic Sclerosis. J Clin Med 2022;11(17)
9. Simpson CE, Damico RL, Hummers L, et al. Serum uric acid as a marker of disease risk, severity, and survival in systemic sclerosis-related pulmonary arterial hypertension. Pulmonary circulation 2019;9(3): 2045894019859477.
10. Tedford RJ, Mudd JO, Girgis RE, et al. Right ventricular dysfunction in systemic sclerosis-associated pulmonary arterial hypertension. Circulation Heart failure 2013;6(5): 953-963.
11. Overbeek MJ, Mouchaers KT, Niessen HM, et al. Characteristics of interstitial fibrosis and inflammatory cell infiltration in right ventricles of systemic sclerosis-associated pulmonary arterial hypertension. International journal of rheumatology 2010;2010
Figures