1648
Sonic DL Cardiac Cine MRI at 3T: Comparison with Conventional Segmented Cine MRI1Fujian Medical University Union Hospital, FuZhou, China
Synopsis
Keywords: Arrhythmia, Arrhythmia
Motivation: This study aimed to explore the feasibility and accuracy of Sonic DL cardiac magnetic resonance cine technology.
Goal(s): We aimed to assess the performance of Sonic DL cine MRI at 3T for left ventricular (LV) volume and mass measurement, especially patients with arrhythmia and/or difficulty in breath-holding.
Approach: 48 patients were consecutively enrolled. EDV, ESV, SV, EF, and LV mass were measured. The agreement and correlation of the parameters were assessed. Image quality was evaluated and structure visibility rating.
Results: Good agreements and correlations were found between the techniques for measuring left ventricular function.
Impact: Sonic DL cardiac cine MRI allowed the assessment of LV volume with high accuracy and showed a significantly better image quality.
INTRODUCTION
Segmented Cine MRI is considered to be the gold standard test for the assessment of cardiac function. It is typically based on a breath-held, segmented data acquisition. Breath holding is particularly difficult for patients with congestive heart failure or in pediatric cases. Sonic DL cardiac cine is a novel combined parallel imaging and deep-learning (DL) based reconstruction framework for accelerating cardiac cine MR acquisitions.It is designed to deliver up to a factor of 12, enabling an acquisition in a single heartbeat per slice, making the patient more comfortable and without the need to undergo multiple breathholds to obtain a diagnostic cardiac exam1. We aimed to assess the performance of Sonic DL cine MRI at 3T for left ventricular (LV) volume and mass measurement, especially patients with arrhythmia and/or difficulty in breath-holding.METHODS
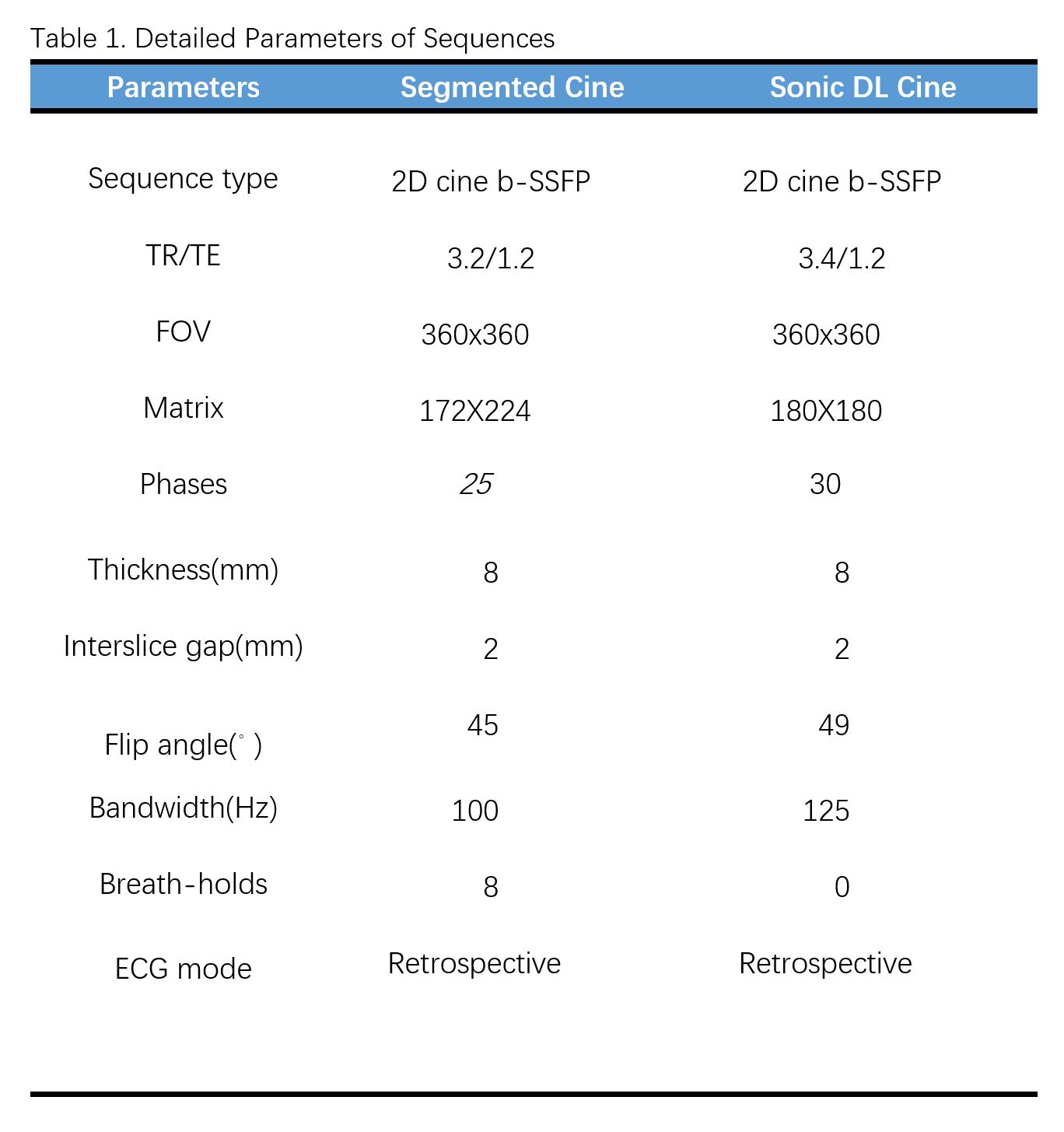
Forty eight patients were consecutively enrolled. Cardiac cine MRI was a part of the conventional MRI protocol. Two patients for whom MRI was contraindicated were excluded. Difficulty in breath-holding was considered to be present when an unstable respiratory curve was observed on the physiology display panel in the user interface of the scanner. The patients were divided into two groups: group 1 (n = 30), patients without arrhythmia or imperfect breath holding; and group 2 (n = 16), patients with arrhythmia and/or difficulty in breath-holding. MRI scan was performed on a clinical 3T MR scanner (Preimier, GE Healthcare). Patients were scanned in the supine position using a 30 chanel phased-array Air body coil (GE Healthcare). MR compatible ECG electrodes and leads were used to obtain an ECG signal for cardiac synchronization. MRI were acquired during breath-holding in end expiration. Subsequently, a series of standard LV short-axis cines were acquired using the segmented balanced steady-state free precession sequence with retrospective ECG gating in a stack of 8 contiguous slices spanning the entire left ventricle from the base to apex. Typical imaging parameters are presented in Table 1. A series of short-axis cine images covering the entire left ventricle using both segmented and Sonic DL balanced steady-state free precession cardiac cine MRI were obtained. Cardiac Volumetric and Mass Analysis The EDV, end-systolic volume (ESV), stroke volume (SV), ejection fraction (EF), and LV mass were measured using the software of CVI 42 (Circle Cardiovascular Imaging Inc., Calgary, Canada). All the short-axis cine images were analyzed in a randomized and blinded manner. A functional analysis of all participants was performed by a cardiovascular radiologist with 10 years of experience. To test intraobserver variability, the functional analysis was repeated by the same radiologist in a subset of 15 randomly selected participants two months later. The interobserver variability was also tested in the same subset of participants by another radiologist with 6 years of experience. End-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), ejection fraction (EF), and LV mass were measured. The agreement and correlation of the parameters were assessed. Additionally, image quality was evaluated using European CMR Registry (Euro-CMR) score and structure visibility rating.RESULTS
In patients without difficulty in breath-holding or arrhythmia, no significant difference was found in Euro-CMR score between the two techniques (0.3 ± 0.7 vs. 0.3 ± 0.5, p > 0.05). Good agreements and correlations were found between the techniques for measuring EDV, ESV, EF, SV, and LV mass. In patients with difficulty in breath-holding or arrhythmia, segmented cine MRI had a significant higher Euro-CMR score (2.8 ± 1.5 vs. 0.4 ± 0.5, p < 0.001).CONCLUSION
Sonic DL cardiac cine MRI at 3T allowed the assessment of LV volume with high accuracy and showed a significantly better image quality compared to that of segmented cine MRI in patients with difficulty in breath-holding and arrhythmia.Acknowledgements
No acknowledgement found.References
1.Sandino CM, Lai P, Vasanawala SS, Cheng JY. Accelerating cardiac cine MRI using a deep learning-based ESPIRiT reconstruction. Magn Reson Med. 2021;85(1):152-167.
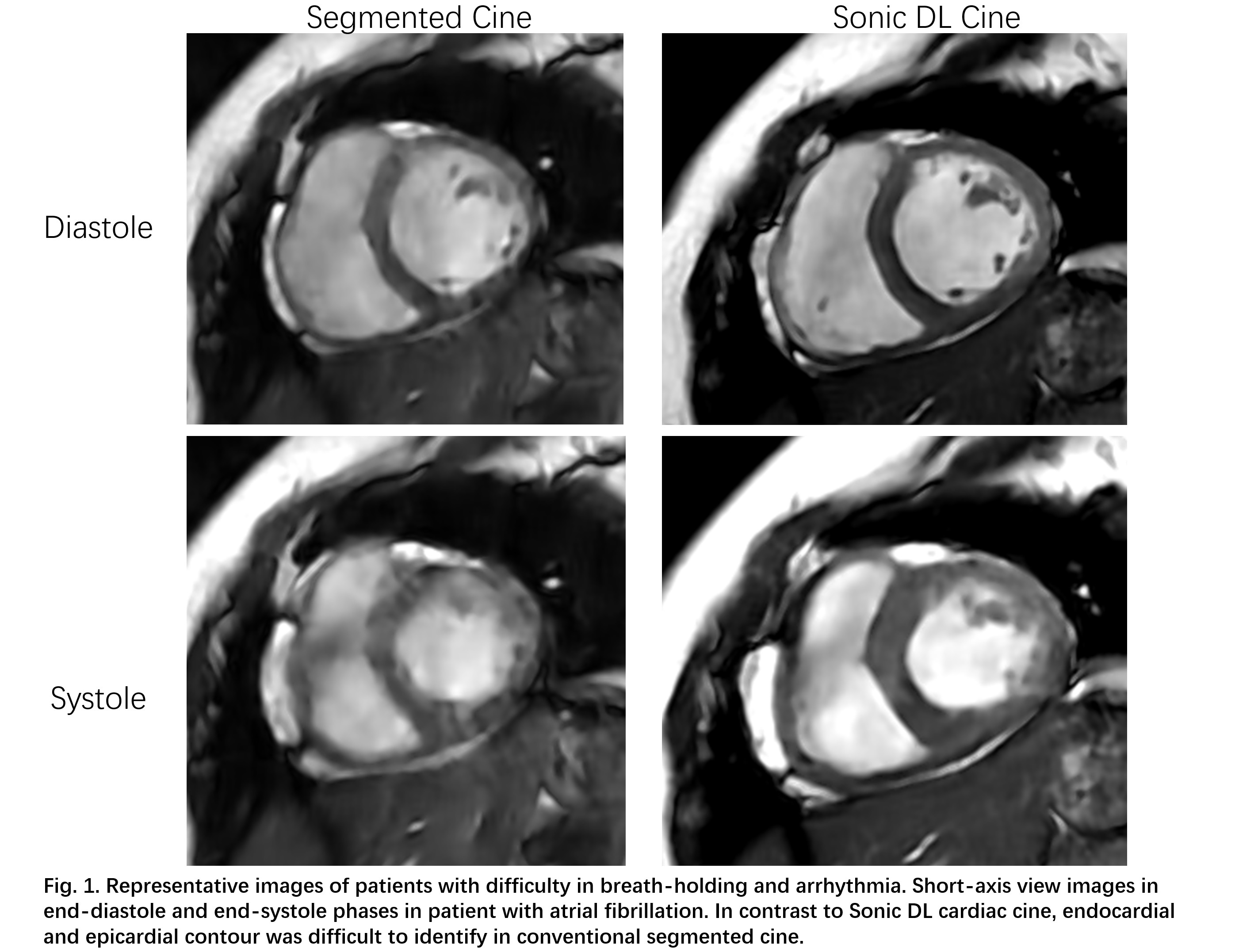
Figures