1647
Rapid, Real-time Cine MRI Produces Clinically Acceptable Image Quality and Accurate Bi-Ventricular Functional Measures in CIED Patients1Department of Radiology, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 2Department of Radiology, Mayo Clinic, Rochester, MN, United States, 3Division of Cardiology, Internal Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 4Division of Cardiology, Internal Medicine, University of Virginia, Charlottesville, VA, United States
Synopsis
Keywords: Arrhythmia, Visualization
Motivation: Standard ECG-gated breath-held (BH) cine MRI often produces non-diagnostic image quality in CIED patients who have a high burden of arrhythmia.
Goal(s): The goal of this study is to produce diagnostic images using a free-breathing real-time cine MRI for those patients.
Approach: We proposed a new pulse sequence to meet our goal.
Results: Our proposed pulse sequence produced clinically acceptable images and accurate bi-ventricular and functional parameters compared with standard BH cine in patients with a CIED.
Impact: Our proposed pulse sequence will be useful for a shorter overall scan time while maintaining a diagnostically acceptable images in all CIED patients.
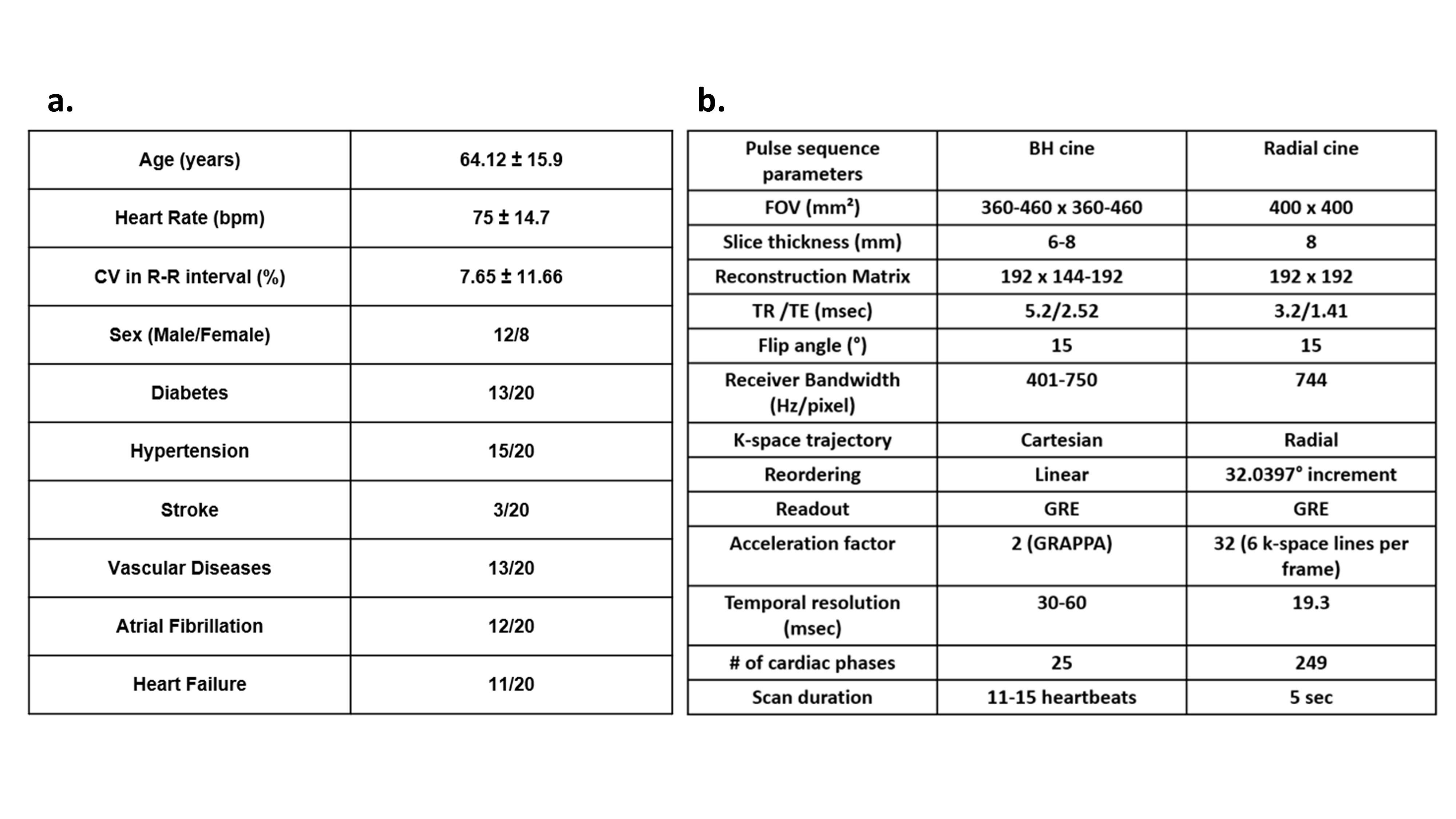
Methods: MRI: We enrolled 20 patients (8 females; mean age = 64.44 ± 16.44 yrs) with a CIED (see Table 1A for demographics) and performed two different cine scans on a 1.5T MRI scanner (Avanto,Siemens Healthineers): clinical BH cine and the proposed FB-RT [1]. The relevant imaging parameters are summarized in Table 1B.
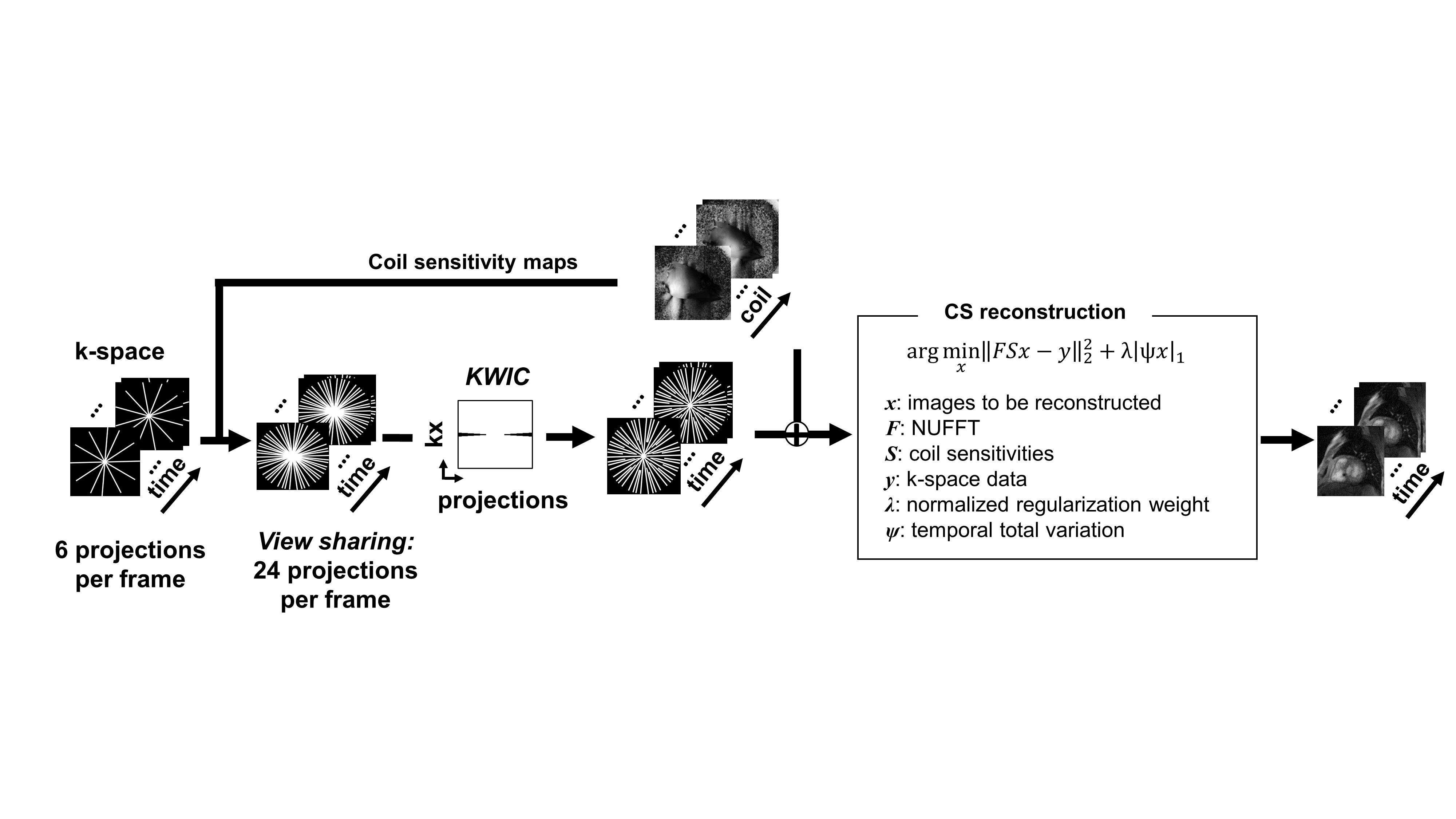
Image Reconstruction: For FB-RT cine, images were constructed on a GPU (2 x 32GB Tesla V100) workstation using the iterative Golden-angle Radial Sparse Parallel (GRASP) [4] framework adapted to reconstruct 6 radial spokes per frame supplemented by 18 shared spokes with KWIC [2] filtering to remove the center of shared k-space lines, as shown in Figure 1.
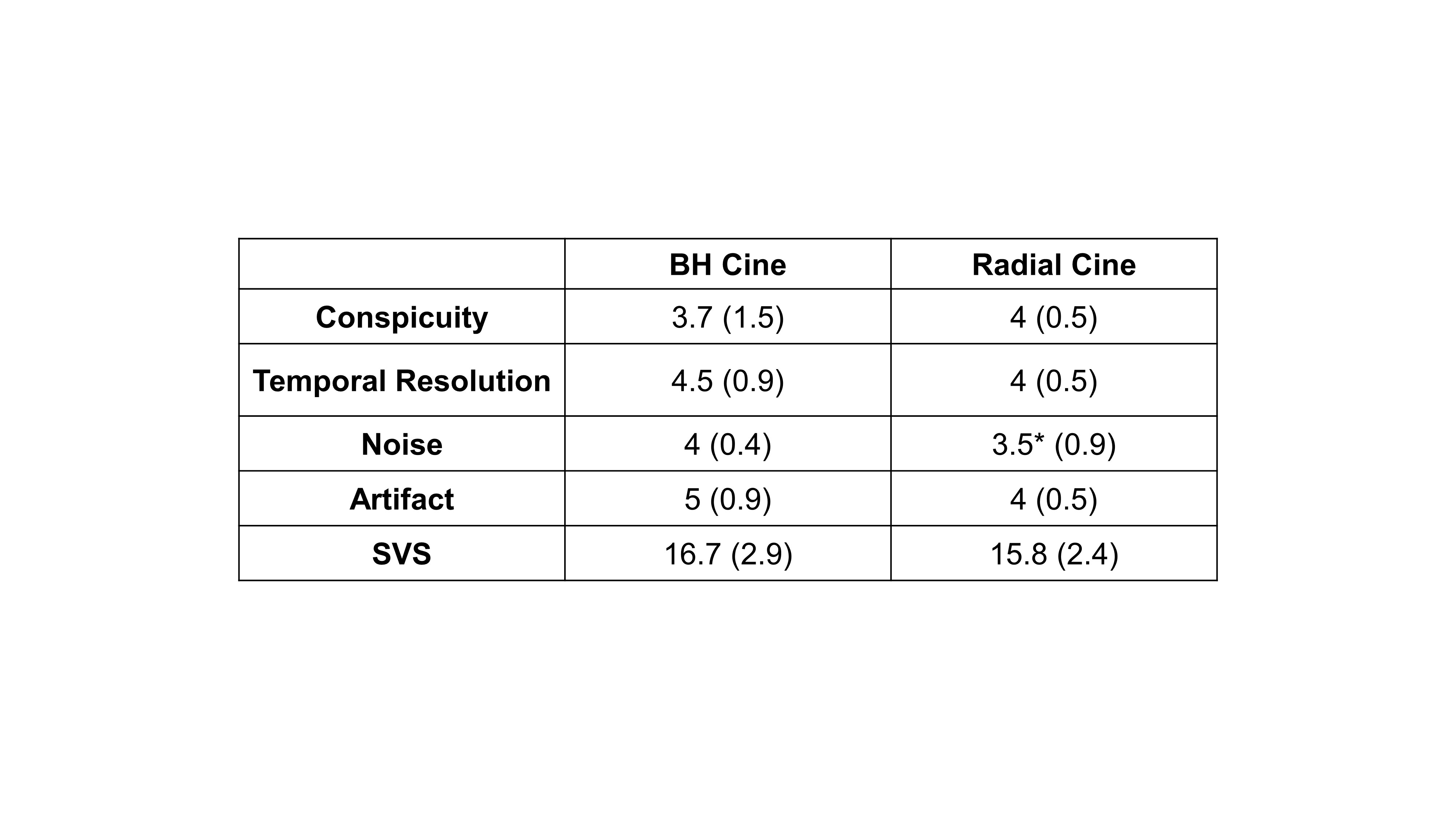
Image Analysis: LV and RV cardiac contours were segmented using the automatic AI tools followed by manual correction in Circle (cvi42,v5.13.9) for BH and FB-RT cine images. For FB-RT with multiple heartbeats per slice, we analyzed the representative (not short or long) heartbeat. Bi-ventricular volumes and functions were quantified. Bland-Altman analysis was conducted to determine the level of agreement between BH cine with FB-RT cine. Two attending cardiologists visually evaluated the image quality (randomly subsampled to 14 patients) using a 5-point Likert scale for each of four categories as shown in Table 2, where a score of 3 defines clinically acceptable. Summed visual score (SVS) is defined as the numerical sum of all scores, and SVS > 12 is defined as clinically acceptable.
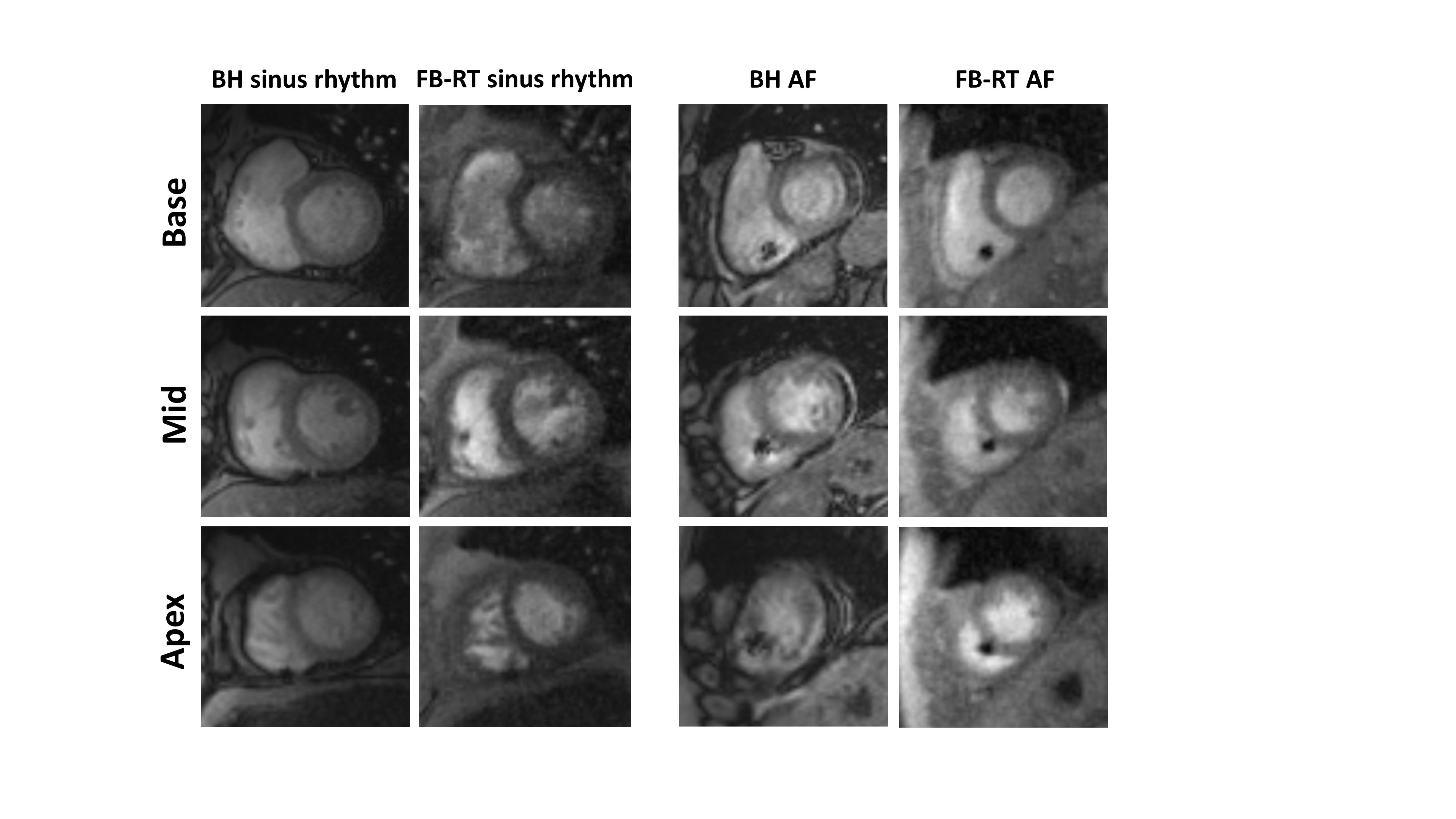
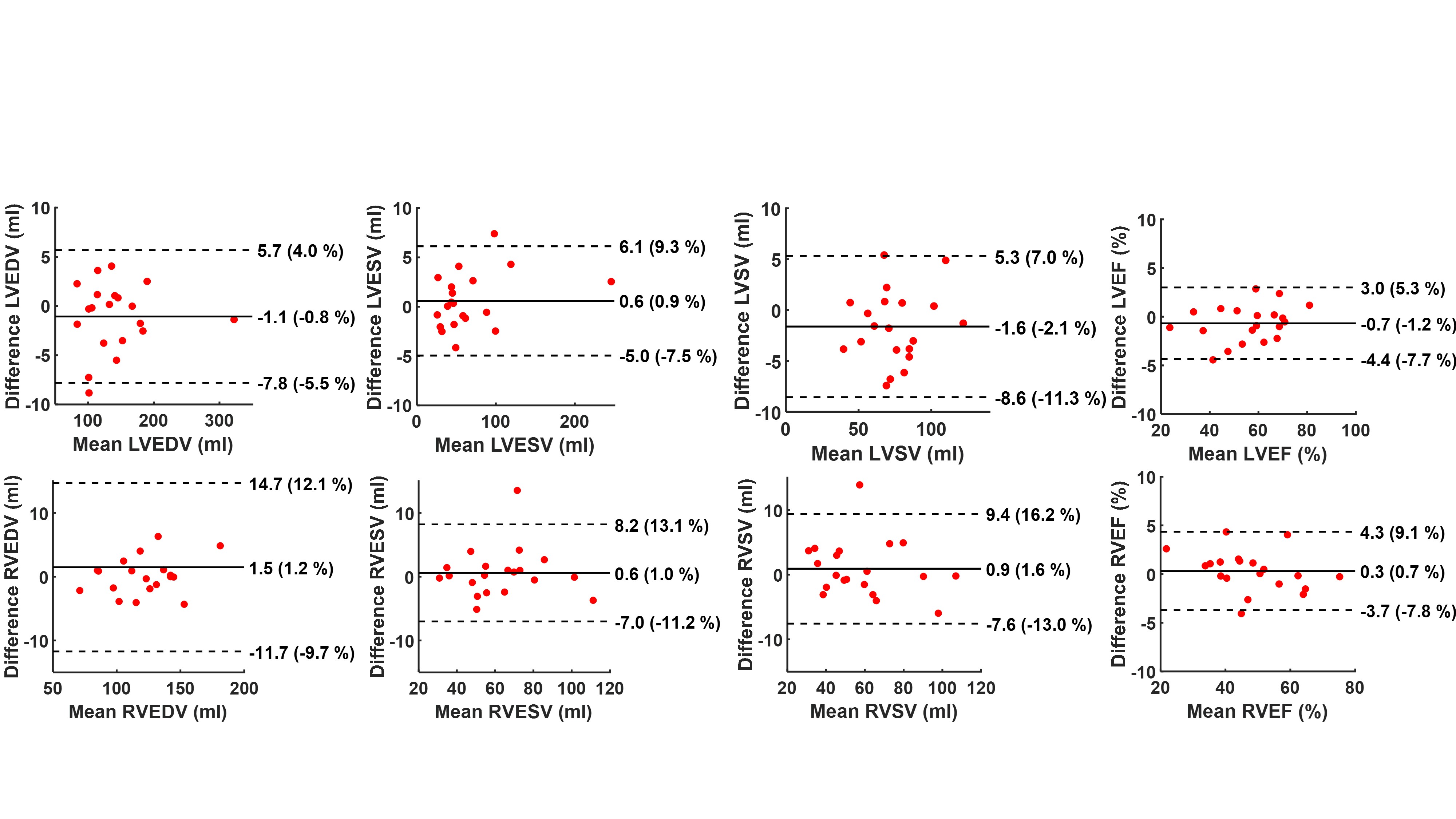
Results: Figure 2 shows representative three short-axis images of one patient in sinus rhythm (CV in R-R interval = 1.88%; see caption in Table 1 for definition of CV) and another patient in atrial fibrillation (CV in R-R interval = 33.22%). While BH cine produced ghosting artifacts in patients with arrhythmia, FB-RT cine produced good image quality in all patients. As shown in Figure 3, both the left ventricle (LV) and right ventricle (RV) parameters were in good agreement; mean difference ranged from -1.6 (-2.1% of mean) to 0.6 (0.9% of mean) for the LV and 0.3 (0.7% of mean) to 1.5 (1.2% of mean) for the RV; there was no systematic trend in any of the Bland-Altman plots. None of the functional parameters were significantly different (p>0.1). As summarized in Table 2, none of the individual image quality scores were significantly different (p>0.32) except for noise; however, all four individual scores were > 3.0 and SVS > 12 for FB-RT radial cine.
Conclusions: Our 32-fold accelerated radial FB-RT cine produced diagnostically acceptable image quality and relatively accurate bi-ventricular volumes and functional parameters compared with standard BH cine in patients with a CIED. This pulse sequence may be useful for shortening overall scan time and producing diagnostically useful images in all CIED patients, even those with arrhythmias and/or dyspnea.
Acknowledgements
The authors would like to thank funding support from the National Institutes of Health (R01HL116895, R01HL151079, R21EB030806A1, 1R01HL167148‐01A1), the American Heart Association (19IPLOI34760317, 949899), and the Radiological Society of North America (EILTC2302).References
1. Hong K, Fan L, Collins JD, Patel AR, Lee DC, and Kim D. Highly-accelerated Real-time Cine MRI with Radial k-space Sampling and View Sharing and KWIC Filtering in Patients with a Cardiac Implantable Electronic Device. SCMR 2023.
2. Song HK, Dougherty L. k-space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI. Magn Reson Med 2000;44(6):825-832.
3. Haji-Valizadeh H, Rahsepar AA, Collins JD, Bassett E, Isakova T, Block T, Adluru G, DiBella EVR, Lee DC, Carr JC, Kim D, Binders CKDOMw, Nicotinamid ESG. Validation of highly accelerated real-time cardiac cine MRI with radial k-space sampling and compressed sensing in patients at 1.5T and 3T. Magn Reson Med 2018;79(5):2745-2751.
4. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2014 Sep;72(3):707-17.
Figures