1646
Preliminary Study of CMR Combined Myocardial Strain Imaging for Left Atrial Fibrosis Assessment in Atrial Fibrillation Patients1Department of Radiology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Arrhythmia, Arrhythmia, Atrial fibrillation (AF); Cardiac magnetic resonance (CMR); Three-dimensional late gadolinium enhancement (3D-LGE); Left atrial fibrosis (LAF)
Motivation: Left atrial (LA) function and structural remodeling in atrial fibrillation (AF) remains uncertain in the context of LA-CMR.
Goal(s): To investigate the effectiveness of 3D-LGE CMR and LA-strain techniques for assessing LA fibrosis in paroxysmal or persistent AF (PaAF, PeAF) patients.
Approach: Preoperative CMR was used to analyze LA-strain parameters. Quantitative assessments of LA wall enhancement utilized the Infarct-to-Interstitial Ratio (IIR) as a reference.
Results: Contrasted with PaAF, those with PeAF exhibited increased LA volumes, reduced LA function, and lower strain values. In 3D-LGE sequences, PeAF patients demonstrated more extensive myocardial enhancement, scar tissue, and interstitial fibrosis in comparison to PaAF patients.
Impact: Our research provides a promising imaging tool for the management of AF patients, with potential translational applications focused on quantitatively and visually assessing LA function and structural remodeling, personalizing treatment, assisting intraoperative navigation, and enabling long-term monitoring.
Introduction
Atrial fibrillation (AF), is a prevalent and prominent cardiac arrhythmia characterized by irregular and rapid electrical activity in the left atria (LA) [1-3]. Despite the development of various treatment strategies, the recurrence of AF remains a concern [2, 4]. LA remolding, encompassing functional, structural, and electrical alterations, constitutes the cornerstone of AF development [5, 6]. Left atrial fibrosis (LAF), characterized by the accumulation of excessive fibrous or scar tissue in the atrial walls, represents a key structural alteration in patients with AF. Recently, the use of delayed gadolinium-enhanced cardiac magnetic resonance (LGE-CMR) has allowed for the visualization and quantification of gadolinium[5, 7]. This technology enables the estimation of extracellular matrix volume, serving as a surrogate marker for myocardial fibrosis [8]. Nonetheless, the utility of employing 3D-LGE CMR along with LA strain technology to evaluate AF patients, spanning from LA function to structural remodeling, remains uncertain. Hence, our objective was to investigate the effectiveness of 3D-LGE CMR in conjunction with LA strain techniques for assessing LAF in patients suffered from AF.Methods
A total of 80 patients with paroxysmal and persistent AF (PaAF and PeAF) who were scheduled for ablation from January 2022 to May 2023 at our institution were retrospectively enrolled. All patients underwent preoperative 3D-LGE CMR examination, and LA storage function, conduit function, booster pump function, total strain (εs), passive strain (εe), active strain (εa), and corresponding strain rates (SRs, SRe, SRa) were analyzed. The extent and degree of LA wall enhancement were quantitatively analyzed using the ratio of signal intensity between LA wall and blood pool (IIR) as a reference. Independent t-tests, Mann-Whitney U tests, and multivariate logistic regression were used to stratify AF categories and develop models.Results
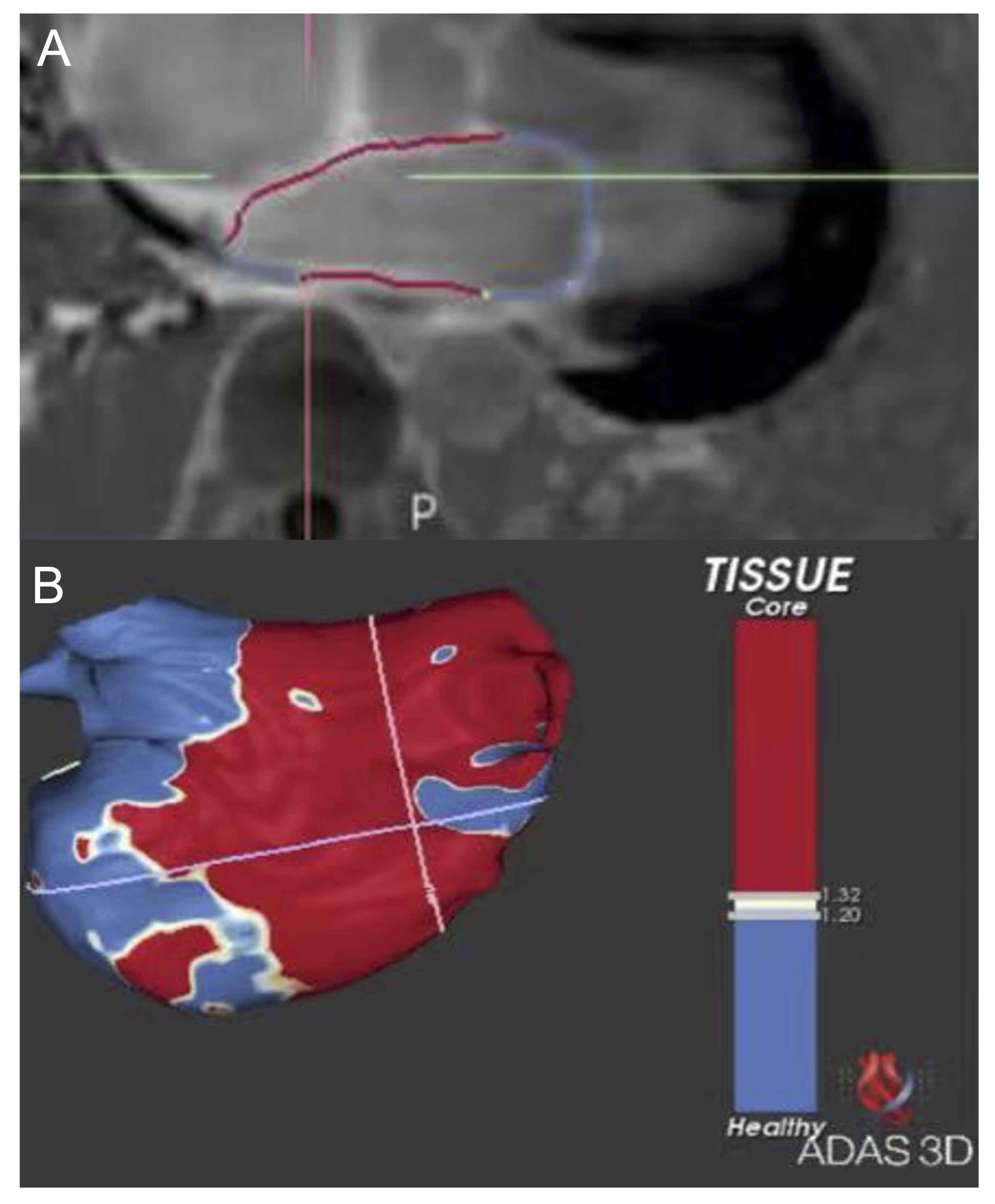
Compared to PaAF, PeAF exhibited significantly increased total volume, sphericity, end-diastolic volume, and end-systolic volume (P<0.05). LA storage function, conduit function, booster pump function, εs, εe, εa, SRs, SRe, and SRa were significantly reduced in PeAF (P<0.001). In the 20-minute and 30-minute 3D-LGE sequences, the PeAF group displayed a higher area and proportion of enhanced myocardium (IIR > 1.2), scar tissue (IIR > 1.32), and interstitial fibrosis (IIR 1.2~1.32) compared to the PaAF group. Multivariate logistic regression revealed that in the clinical subgroup, BMI (OR 1.195, 95% CI 1.039-1.374, P=0.012) and CHA2DS2-VASc score (OR 1.471, 95% CI 1.105-1.958, P=0.008) were independent risk factors for PeAF, yielding an AUC of 0.753 (95% CI 0.637-0.870, P<0.001). In the myocardial strain subgroup, εs (OR 0.749, 95% CI 0.647-0.867, P<0.001) and LA conduit function (OR 1.079, 95% CI 1.004-1.159, P=0.038) were independent predictors of AF classification, with an AUC of 0.927 (95% CI 0.865-0.988, P<0.001). In the 3D-LGE subgroup, the 20-minute LA enhancement total area (OR 1.080, 95% CI 1.041-1.121, P<0.001) and interstitial fibrosis percentage (OR 1.377, 95% CI 1.004-1.887, P<0.001) were independent risk factors for stratifying PeAF and PaAF (AUC=0.933, 95% CI 0.875-0.991, P<0.001). After integrating aforementioned parameters, the comprehensive model achieved an AUC of 0.957 (95% CI 0.909-1.000, P<0.001), with εa (OR 0.709, 95% CI 0.526-0.955, P=0.024) and 30-minute LA enhancement total area (OR 1.060, 95% CI 1.017-1.104, P=0.005) as independent predictors.Discussion
In this study, our aim was to evaluate the utility of combining 3D-LGE CMR with strain imaging for the quantitative assessment of LAF in patients with AF. The results indicated significant differences between patients with PeAF and PaAF. Specifically, patients with PeAF exhibited increased LA volumes and decreased LA function and strain values, which were consistent with the functional outcomes observed in echocardiographic imaging for stratifying PeAF and PaAF[9]. In the 3D-LGE sequences, PeAF patients displayed more extensive myocardial enhancement, scar tissue, and interstitial fibrosis compared to PaAF ones, in line with a prior 3D-LGE study[1]. Furthermore, our analysis revealed independent risk factors for PeAF within clinical, myocardial strain, and 3D-LGE subgroups. Parameters such as BMI, CHA2DS2-VASc score, LA strain values, and the extent of LA wall enhancement were identified as significant predictors, partly in agreement with previous research[1, 9-11]. In summary, our findings support the potential of preoperative 3D-LGE CMR with strain techniques for providing both quantitative and visual assessments of LAF in AF patients. This approach offers valuable imaging evidence for surgical planning and intraoperative electrophysiological navigation fusion, thereby aiding in the management of AF and its associated structural changes.Conclusion
Preoperative 3D-LGE CMR with strain techniques can provide quantitative and visual assessment of LAF, offering crucial imaging evidence for surgical planning and intraoperative electrophysiological navigation fusion.Acknowledgements
No acknowledgement found.References
[1] LEE D K, SHIM J, CHOI J I, et al. Left Atrial Fibrosis Assessed with Cardiac MRI in Patients with Paroxysmal and Those with Persistent Atrial Fibrillation [J]. Radiology, 2019, 292(3): 575-582.
[2] MCGANN C, AKOUM N, PATEL A, et al. Atrial fibrillation ablation outcome is predicted by left atrial remodeling on MRI [J]. Circ Arrhythm Electrophysiol, 2014, 7(1): 23-30.
[3] CHUNG M K, REFAAT M, SHEN W K, et al. Atrial Fibrillation: JACC Council Perspectives [J]. J Am Coll Cardiol, 2020, 75(14): 1689-1713.
[4] MARROUCHE N F, WILBER D, HINDRICKS G, et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study [J]. JAMA, 2014, 311(5): 498-506.
[5] HABIBI M, CHRISPIN J, SPRAGG D D, et al. Utility of Cardiac MRI in Atrial Fibrillation Management [J]. Card Electrophysiol Clin, 2020, 12(2): 131-139.
[6] JANUARY C T, WANN L S, ALPERT J S, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society [J]. Circulation, 2014, 130(23): 2071-2104.
[7] BENITO E M, CARLOSENA-REMIREZ A, GUASCH E, et al. Left atrial fibrosis quantification by late gadolinium-enhanced magnetic resonance: a new method to standardize the thresholds for reproducibility [J]. Europace, 2017, 19(8): 1272-1279.
[8] AMBALE-VENKATESH B, LIMA J A. Cardiac MRI: a central prognostic tool in myocardial fibrosis [J]. Nat Rev Cardiol, 2015, 12(1): 18-29.
[9] GUPTA D K, SHAH A M, GIUGLIANO R P, et al. Left atrial structure and function in atrial fibrillation: ENGAGE AF-TIMI 48 [J]. Eur Heart J, 2014, 35(22): 1457-1465.
[10] MANCIO J, SOUSA-NUNES F, MARTINS R, et al. Decoding the radiomic and proteomic phenotype of epicardial adipose tissue associated with adverse left atrial remodelling and post-operative atrial fibrillation in aortic stenosis [J]. Eur Heart J Cardiovasc Imaging, 2022,
[11] PARWANI A S, MORRIS D A, BLASCHKE F, et al. Left atrial strain predicts recurrence of atrial arrhythmias after catheter ablation of persistent atrial fibrillation [J]. Open Heart, 2017, 4(1): e000572.
Figures