1643
Increased Cerebral Blood Flow after Catheter Ablation in Atrial Fibrillation: A Multi-delay ASL-based Study1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2Tiantan Neuroimaging Center of Excellence, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 3United Imaging Research Institute of Intelligent Imaging, Beijing, China, 4Cardiac Arrhythmia Center, Fuwai Hospital, National Center for Cardiovascular Diseases, National Key Laboratory, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 5Shanghai United Imaging Healthcare Co., LTD, Shanghai, China, 6Department of Cardiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Arrhythmia, Arterial spin labelling, Atrial Fibrillation
Motivation: Cerebral hypoperfusion may be a major link between atrial fibrillation (AF) and neuropathologic processes. Whether catheter ablation can effectively improve cerebral perfusion needs to be evaluated by noninvasive methods.
Goal(s): To assess the effects of catheter ablation on overall and regional cerebral blood perfusion in AF patients using multi-delay ASL.
Approach: Multi-delay ASL was performed before and after catheter ablation to calculate arterial transit time and cerebral blood flow. Whole and regional cerebral perfusion parameters before and after ablation were characterized and compared in paroxysmal and non-paroxysmal groups.
Results: Cather ablation significantly increased overall and regional cerebral blood perfusion, especially in non-paroxysmal AF.
Impact: Catheter ablation can improve cerebral perfusion and maintain brain health, which should be considered even in asymptomatic patients. Multi-delay ASL can be used to evaluate and monitor cerebral perfusion in AF and help with patient screening and therapeutic strategy development.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia and a well-known risk factor for stroke1. Over the past decade, there has been growing evidence suggesting that AF is also an independent risk factor for other neurological disorders, including cognitive dysfunction and dementia, regardless of the presence of stroke2,3. In addition to thrombosis, chronic cerebral hypoperfusion caused by beat-to-beat variability and subsequent reduced left ventricular output in AF may be another important link between AF and neuropathologic processes, leading to brain damage4. Therefore, it is reasonable to hypothesize that restoring sinus rhythm through catheter ablation may potentially improve cerebral perfusion and be crucial for brain function maintenance. However, there is still a lack of evidence to date. To advance therapeutic strategies and pinpoint the patient populations that might benefit from catheter ablation in the future, it is imperative to evaluate and monitor the efficacy of ablation therapy in improving whole-brain and regional cerebral blood flow using noninvasive methods. Multi-delay Arterial Spin Labeling (ASL) is a noninvasive technique capable of assessing multi-parametric perfusion parameters and providing more accurate perfusion information compared to traditional single-delay ASL5. This study aims to evaluate the effects of catheter ablation on perfusion changes in patients with AF using multi-delay ASL.Methods
Eligible patients aged 18 to 80 years who were diagnosed with AF and prepared for catheter ablation were enrolled in this study. Exclusion criteria included any previous ablation or surgical therapy for AF, previous organic or degenerative brain diseases (stroke, transient ischemic attack, neurodegenerative diseases, encephalitis, head trauma, hydrocephalus, brain tumor, epilepsy and dementia), intracranial or carotid atrial occlusion or stenosis >50% and depressive state or mental abnormality. A total of ten AF patients (six paroxysmal and four non-paroxysmal AF) were enrolled. Radiofrequency catheter ablation was performed according to the standard-of-care procedure. All patients were prescribed oral anticoagulants and continuously on anticoagulants after ablation therapy. MRI was performed before catheter ablation and repeated within seven days after ablation.MR imaging was performed on a 3.0T MR scanner (uMR Nx, United Imaging Healthcare, China) with a 64-channel head coil. Imaging sequences included 3D multi-delay pCASL and high-resolution T1-MPRAGE for image registration. The parameters of pCASL were detailed as follows: GRASE, TE/TR 14.02/5841ms, labeling time 1800ms, post labeling delay 700/1200/1700/2200/2700ms, resolution 3.5×3.5×3.5mm3, FOV 224×224×140mm3, scan time 6:59. The multi-delay ASL was analyzed on uOmnispace.MR (United Imaging Healthcare, China) to derive the cerebral blood flow (CBF), arterial transit time (ATT) and arterial cerebral blood volume (aCBV) maps. All of these cerebral maps were co-registered to MPRAGE images and registered to the MNI space. Global gray matter was then segmented into frontal, parietal, temporal, occipital, limbic lobes and subcortical regions for further analyses. Paired t-tests or Wilcoxon signed-rank tests were used for statistical analysis. Probability value of P<0.05 was considered significant.
Results
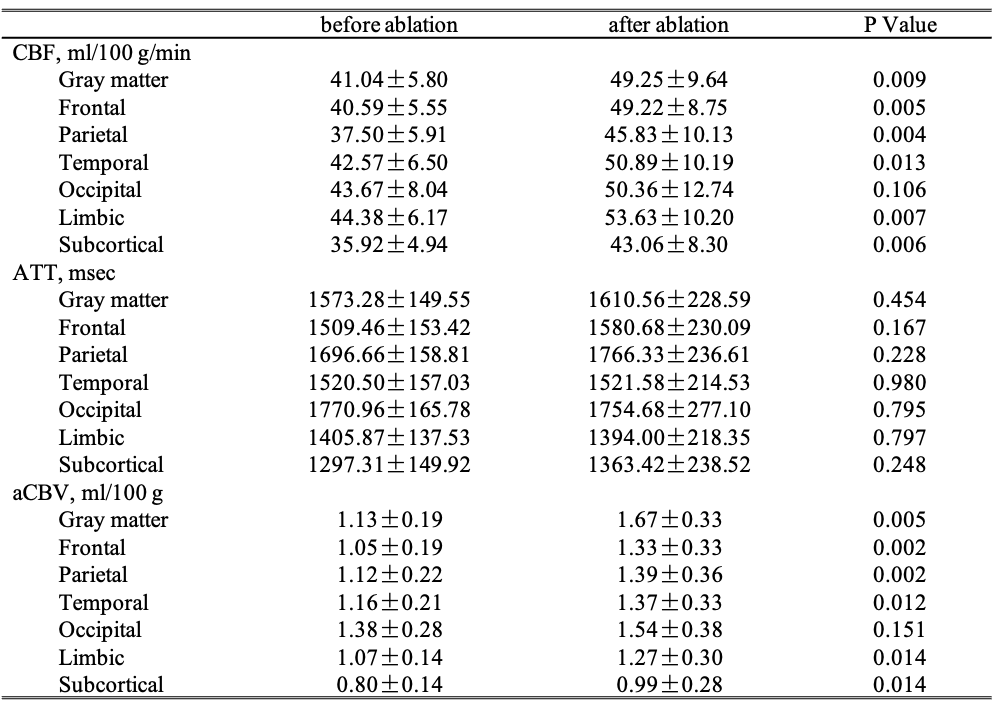
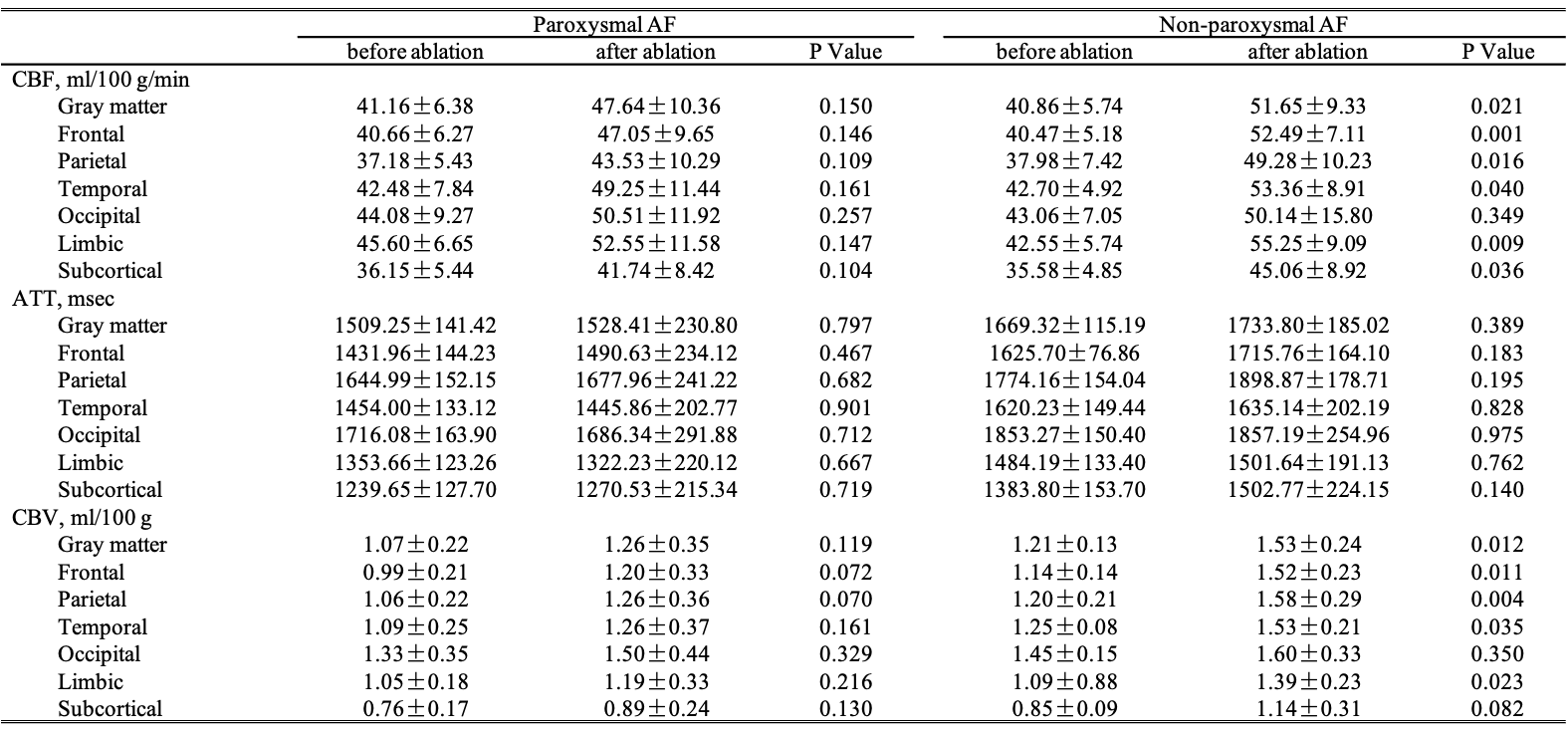
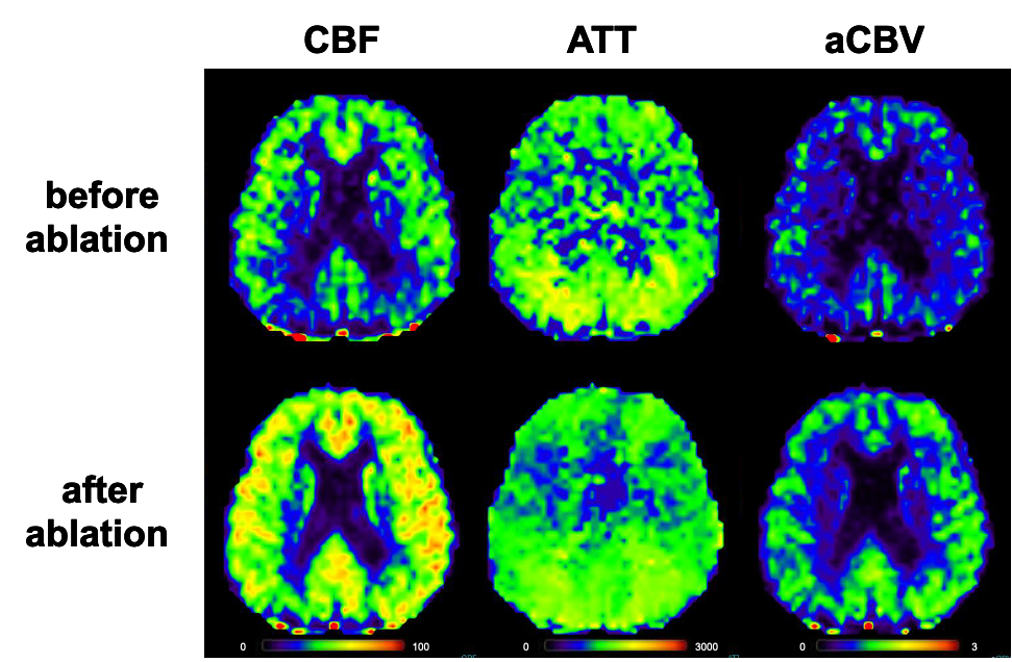
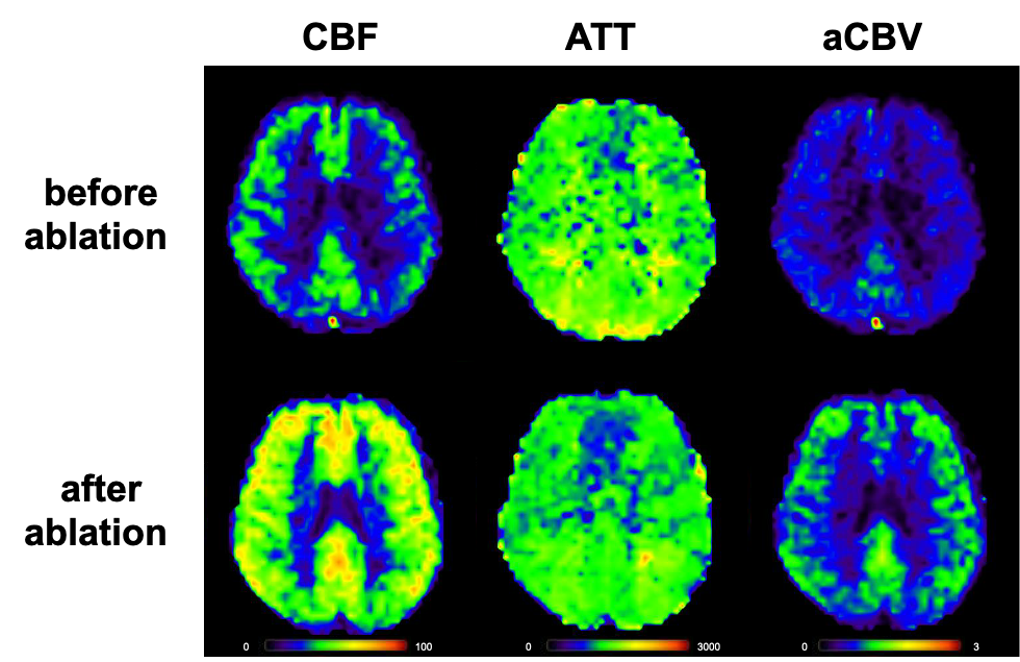
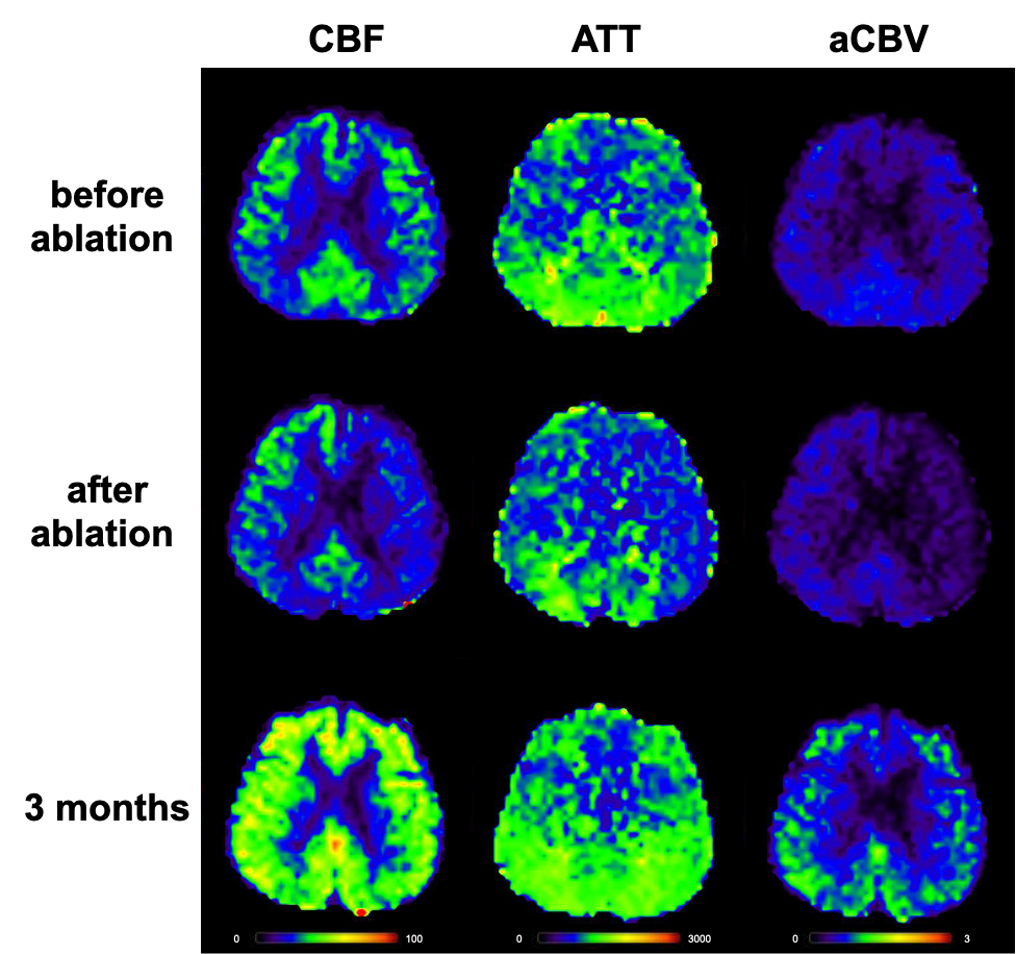
Table 1 showed that patients exhibited significantly increased overall CBF (49.25±9.64 vs. 41.04±5.80 [ml/100g/min], p=0.009) and aCBV (1.67±0.33 vs. 1.13±0.19 [ml/100g], P=0.005) after ablation. Specifically, CBF and aCBV displayed significant improvements in the frontal lobe (P1=0.005; P2=0.002), parietal lobe (P1=0.004; P2=0.002), temporal lobe (P1=0.013; P2=0.012), limbic lobe (P1=0.007; P2=0.014) and subcortical lobe (P1=0.006; P2=0.014). No significant difference was found in ATT. When patients were categorized according to the AF type, the results showed that non-paroxysmal AF patients had greater improvements in CBF after ablation (51.65±9.33 vs. 40.86±5.74 [ml/100g/min]) than paroxysmal AF patients (47.64±10.36 vs. 41.16±6.38 [ml/100g/min]) (Table 2). Representative images were shown in Figures 1-3(1: non-paroxysmal patient, 2: paroxysmal patient and 3: paroxysmal patient with an additional 3 months’ examination). Similar results were also found across different brain regions and in aCBV.Discussion
This study investigated whether catheter ablation can effectively improve overall and local cerebral blood perfusion using the multi-delay ASL method. Our preliminary results demonstrated significantly increased CBF and aCBV in the whole brain and in different brain regions in the short term after ablation, especially in non-paroxysmal AF patients. Paroxysmal AF patients can benefit most within three months after surgery. These findings imply that catheter ablation may be an effective therapeutic strategy for brain health maintenance, through restoring sinus rhythm and improving cerebral blood perfusion. Catheter ablation should be potentially considered in future guidelines and real-world clinical settings, even in asymptomatic AF patients. In addition, the application of multi-delay ASL in AF patients could be considered to evaluate/monitor the severity of hypoperfusion and screen for patients most likely to benefit from ablation therapy.Conclusion
Using multi-delay ASL, our study demonstrated significantly improved CBF and aCBV after catheter ablation therapy in patients with AF, especially in those with non-paroxysmal AF.Acknowledgements
NoneReferences
1. Elliott AD, Middeldorp ME, Van Gelder IC, Albert CM, Sanders P. Epidemiology and modifiable risk factors for atrial fibrillation. Nat Rev Cardiol. 2023;20:404-417. doi: 10.1038/s41569-022-00820-82.
2. Kogelschatz B, Zenger B, Steinberg BA, Ranjan R, Jared Bunch T. Atrial fibrillation and the risk of early-onset dementia and cognitive decline: An updated review. Trends Cardiovasc Med. 2023. doi: 10.1016/j.tcm.2023.01.0053.
3. Koh YH, Lew LZW, Franke KB, Elliott AD, Lau DH, Thiyagarajah A, Linz D, Arstall M, Tully PJ, Baune BT, et al. Predictive role of atrial fibrillation in cognitive decline: a systematic review and meta-analysis of 2.8 million individuals. Europace. 2022;24:1229-1239. doi: 10.1093/europace/euac0034.
4. Blum S, Conen D. Mechanisms and Clinical Manifestations of Cognitive Decline in Atrial Fibrillation Patients: Potential Implications for Preventing Dementia. Can J Cardiol. 2023;39:159-171. doi: 10.1016/j.cjca.2022.10.0135.
5. Fan X, Lai Z, Lin T, Li K, Hou B, You H, Wei J, Qu J, Liu B, Zuo Z, et al. Multidelay MR Arterial Spin Labeling Perfusion Map for the Prediction of Cerebral Hyperperfusion After Carotid Endarterectomy. J Magn Reson Imaging. 2023;58:1245-1255. doi: 10.1002/jmri.28634
Figures