1642
Dynamic, Regularized, Adaptive Cluster Optimization (DRACO) for Free-breathing Cardiac Cine MRI in Patients with Atrial Fibrillation1Physics and Biology in Medicine Graduate Program, University of California, Los Angeles, Los Angeles, CA, United States, 2Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 3Division of Cardiology, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, Los Angeles, CA, United States, 4Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 5Department of Radiation Oncology, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
Keywords: Arrhythmia, Arrhythmia
Motivation: Irregular cardiac motion can degrade image quality and preclude the use of conventional segmented cine MRI for quantitative evaluation of cardiac function. And it can be difficult for some patients to do multiple breath holds.
Goal(s): To evaluate a cluster-based algorithm and reconstruction approach for cine MRI in patients with atrial fibrillation under free-breathing condition.
Approach: Ten atrial fibrillation patients were scanned under breath-held and free-breathing conditions. Image quality, SNR, CNR, and edge sharpness were assessed.
Results: No significant difference in image quality scores, SNR, CNR, and edge sharpness were found for images obtained under breath-held and free-breathing conditions.
Impact: Adaptive cluster-based motion binning with temporal total variation reconstruction is effective at handling irregular cardiac motion and enables high quality, free-breathing cine MRI in patients with atrial fibrillation.
Introduction
Segmented cardiac cine MRI[1] is the default technique for quantitative evaluation of cardiac morphology and function. However, gating approaches that assume a regular rhythm[2-5] are prone to failure in the setting of chaotic arrhythmias, especially atrial fibrillation. A data-driven clustering algorithm[6] with higher robustness against irregular cardiac motion was recently developed. By adding a cluster-based total variation reconstruction step, Dynamic Regularized Adaptive Cluster Optimization (DRACO)[7] enhanced image quality and temporal continuity in arrhythmia patients under breath-held conditions. We aim to assess the performance of DRACO in patients with atrial fibrillation under free-breathing conditions.Methods
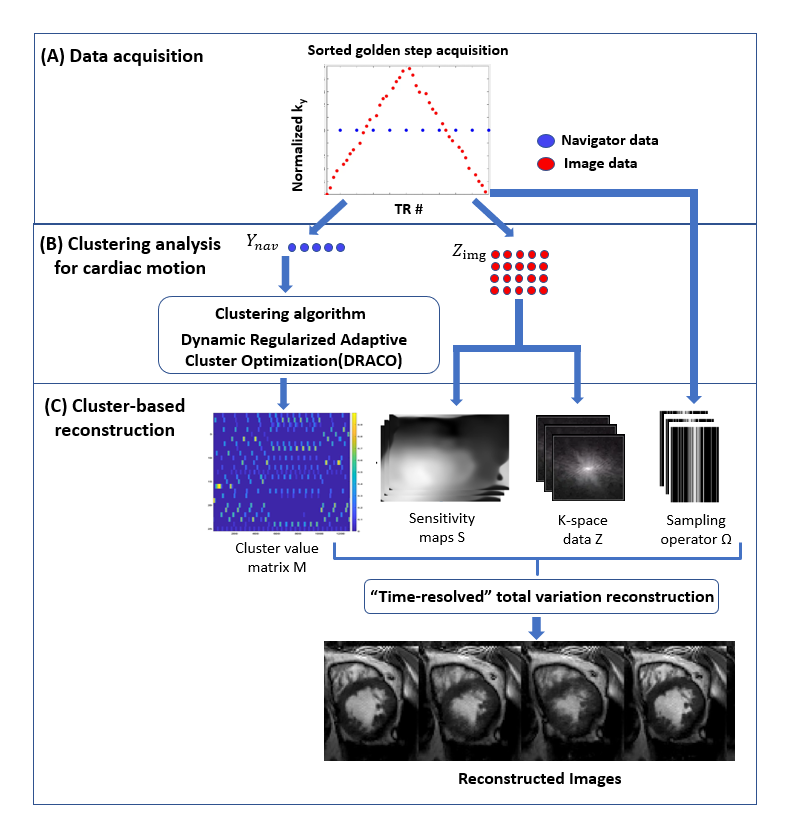
Ten patients (age 73±11 years; heart rate 64±13 bpm) with atrial fibrillation were scanned on a clinical 3.0T scanner (Skyra, Siemens) using a modified segmented golden step bSSFP sequence (FA = 55°, matrix size = 208*172, spatial resolution = 1.8mmx1.8mmx8mm, TE/TR = 1.7ms/3.4ms). Ventricular short-axis cine slices were first acquired with the sequence during breath-holding. To test DRACO’s performance under free-breathing, a mid ventricular short-axis slice was also acquired under free-breathing for comparison. Clustered-based motion binning and image reconstruction were completed using DRACO (Figure 1). The DRACO algorithm optimizes Eq. 1 (Figure 2) to obtain a cluster matrix M and cluster centroid C for motion state representation. Y is the acquired motion signal. Ω, F, S, and Z are the under-sampling operator, Fourier transform operator, coil sensitivity maps, and k-space data, respectively. RM is the continuous regularization term for M along the time dimension, RC is the continuity regularization term for C along the cluster dimension and TV is the temporal total variation penalty term for the pseudo-real-time images. M is applied to reconstruct pseudo-real-time images IK according to Eq.2.(Figure 2)When generating image results for the breath-held and free-breathing data, the same λ values in Eq.2 were used to do a direct comparison between the two conditions. To compare DRACO’s performance under breath-held and free-breathing conditions, we calculated the SNR, CNR, image sharpness, and image quality of the images in the systole and diastole phases. The image sharpness was measured with the average slope of a line profile across the interventricular septum. Image quality was evaluated using a 4-point Likert scale score (1=non-diagnostic, 2=diagnostic, 3=good image quality with few artifacts that do not obscure the cardiac borders, 4=excellent image quality). Paired t-tests were used to compare SNR, CNR, and image sharpness. The Wilcoxon signed-rank test was used to compare image quality scores.
Results and Discussion
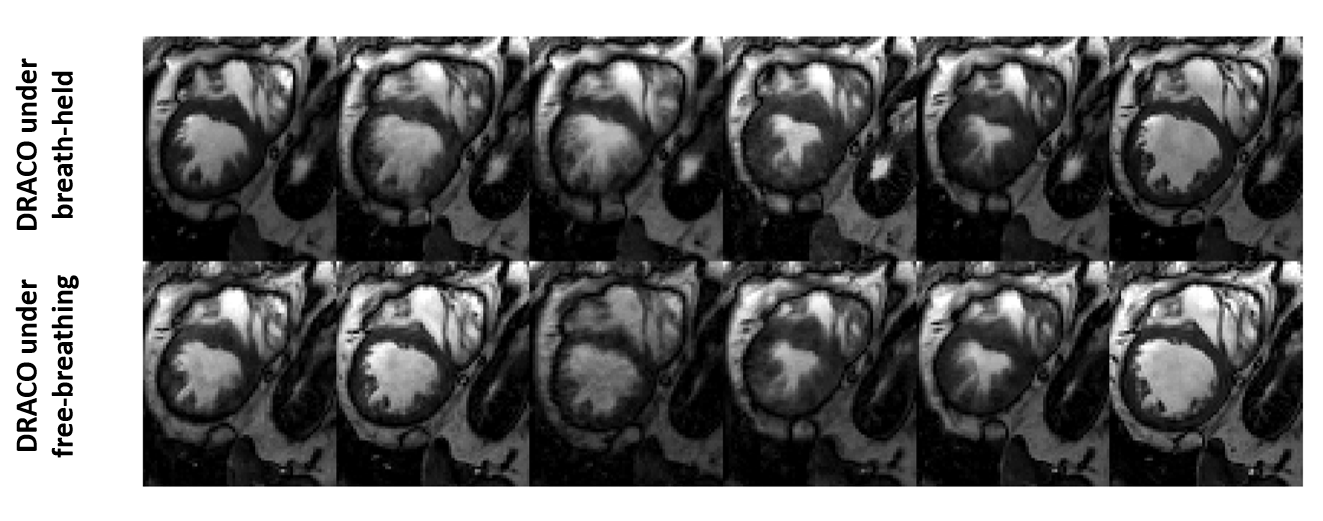
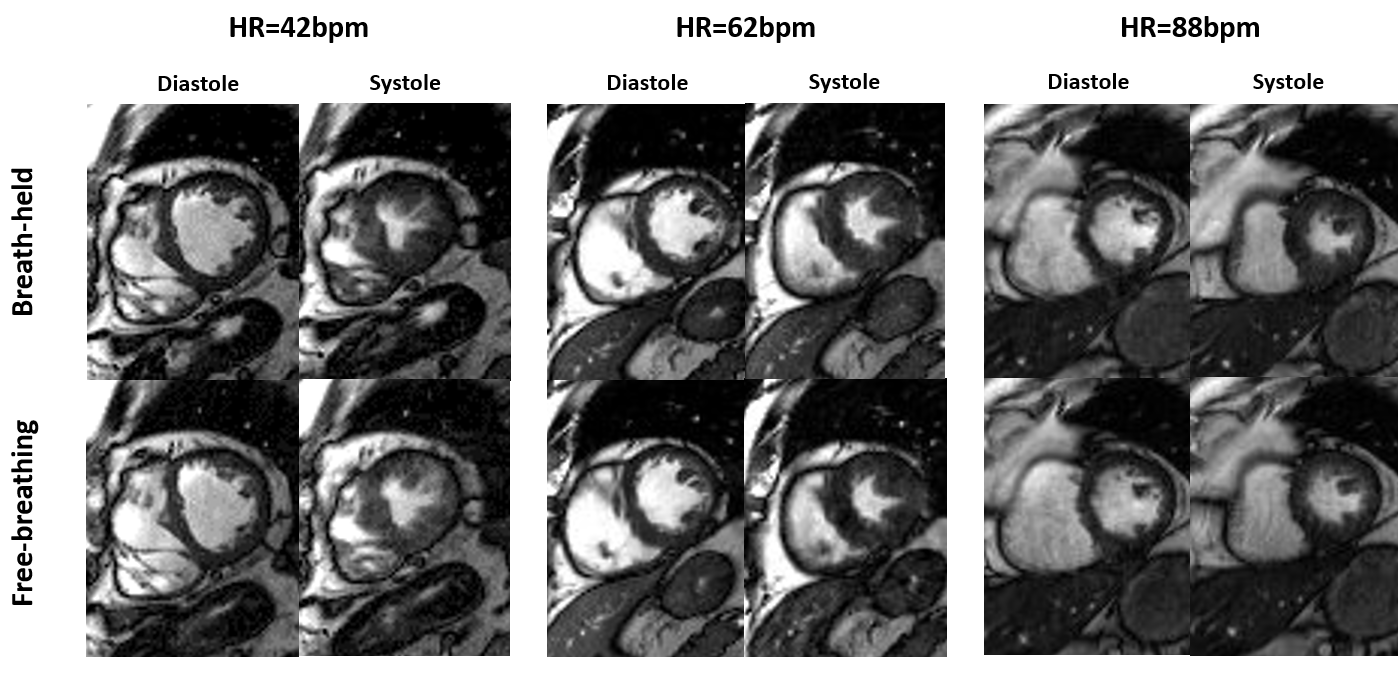
The SNR and CNR values of images obtained under breath-held and free-breathing conditions were not significantly different (SNR 7.41±1.79 vs 6.92±1.48, p=0.36; CNR 5.42±1.42 vs 5.10±1.24, p=0.46). Image sharpness was also not significantly different between breath-held and free-breathing (1.24±0.43 vs 1.16±0.39, p=0.60). No significant difference in image quality scores for breath-held and free-breathing images was noted (p=0.99). 100% of breath-held images received image quality scores >=3, whereas 70% of the images received a score of 4. 100% of free-breathing images received scores >=3, whereas 65% of the images received a score of 4. Both breath-held and free-breathing images reconstructed using the DRACO approach had good image quality (Figure 3) and showed comparable quality and sharpness at similar cardiac phases. Diastolic and systolic images belonging to three patients with atrial fibrillation and variable heart rates are shown in Figure 4. Both breath-held and free-breathing images obtained between 42-88 bpm had excellent image quality (score=4). These findings suggest DRACO’s robustness against respiration motion as well as atrial fibrillation pattern and heart rates.Conclusion
The proposed DRACO approach is robust to respiration motion and can be used for free-breathing cardiac cine MRI of patients with atrial fibrillation. Confirmation of these findings in a larger set of patients with a wider range of heart rates will be needed.Acknowledgements
This work was supported by the National Institutes of Health (R01HL148182, R01HL127153) and the Veterans Health Administration (I01CX001901). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.References
1. Atkinson, Dennis J., and R. R. Edelman. "Cineangiography of the heart in a single breath hold with a segmented turboFLASH sequence." Radiology 178.2 (1991): 357-360.
2. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD‐GRASP: golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. Magnetic resonance in medicine. 2016;75(2):775-88.
3. Han F, Zhou Z, Han E, Gao Y, Nguyen KL, Finn JP, et al. Self‐gated 4D multiphase, steady‐state imaging with contrast enhancement (MUSIC) using rotating cartesian K‐space (ROCK): validation in children with congenital heart disease. Magnetic resonance in medicine. 2017;78(2):472-83.
4. Pang J, Sharif B, Fan Z, Bi X, Arsanjani R, Berman DS, et al. ECG and navigator‐free four‐dimensional whole‐heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magnetic resonance in medicine. 2014;72(5):1208-17.
5. Roy CW, Di Sopra L, Whitehead KK, Piccini D, Yerly J, Heerfordt J, et al. Free-running cardiac and respiratory motion-resolved 5D whole-heart coronary cardiovascular magnetic resonance angiography in pediatric cardiac patients using ferumoxytol. Journal of Cardiovascular Magnetic Resonance. 2022;24(1):1-12.
6. Ming Z, Pogosyan A, Christodoulou AG, Finn JP, Ruan D, Nguyen KL. Data-driven clustering for ECG-free cine MRI with robustness against irregular cardiac motion. Proceedings of the 32nd International Society for Magnetic Resonance in Medicine (ISMRM), 5123.
7. Ming Z, Pogosyan A, Christodoulou AG, Finn JP, Ruan D, Nguyen KL. Dynamic Regularized Adaptive Cluster Optimization (DRACO) for Cardiac Cine MRI in Complex Arrhythmias. SCMR 2024
Figures