1639
Cardiac and respiratory self-gating based on PCA of selected points from coil arrays1School of Biomedical Engineering, ShanghaiTech University, Shanghai, China, 2United Imaging Healthcare, Shanghai, China, 3Diagnostic Imaging Center, Shanghai Children’s Medical Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Synopsis
Keywords: Arrhythmia, Precision & Accuracy, cardiac and respiratory self-gating
Motivation: ECG-gating for cardiac MR Imaging may fail, especially at high field, and the conventional self-gating method is insufficient to effectively extract the cardiac signal in 3D cardiac MR cine with high precision (previous precision 20-30ms).
Goal(s): Our goal was to achieved a reliable cardiac self-gating technique with the precision of 10ms level.
Approach: We proposed a two-step selective PCA self-gating method by first selecting the heart beating or respiration sensitive points and then performing PCA.
Results: The proposed method achieved a temporal precision of 11ms for 3D cardiac cine images.
Impact: The proposed selective PCA self-gating technique can be applied in poor ECG-gating MR scans, such as patients with hairy chests or obesity, as well as in high-field environments, with a high level of precision down to 11ms.
INTRODUCTION
ECG is a widely used technique for cardiac motion gating in cardiac MR Imaging. However, the ECG signal is often impaired by the magnetohydrodynamic effect, particularly in high-field ($$$\geq$$$3T) scanners, for patients with hairy chests, and obese patients. As an alternative, self-gating provides a wireless method to obtain the cardiac dynamic state in 2D cine with about 8ms uncertainty under breath-hold1. Nevertheless, compared to the standard ECG signal, the uncertainty of current 3D cardiac self-gating is approximately 20ms-30ms2-4. This means that if a 50ms duration is set for a cardiac phase, the cardiac phase has an uncertainty of about half the cardiac phase duration.METHODS
ROCK Sequence and in Vivo Experiments:
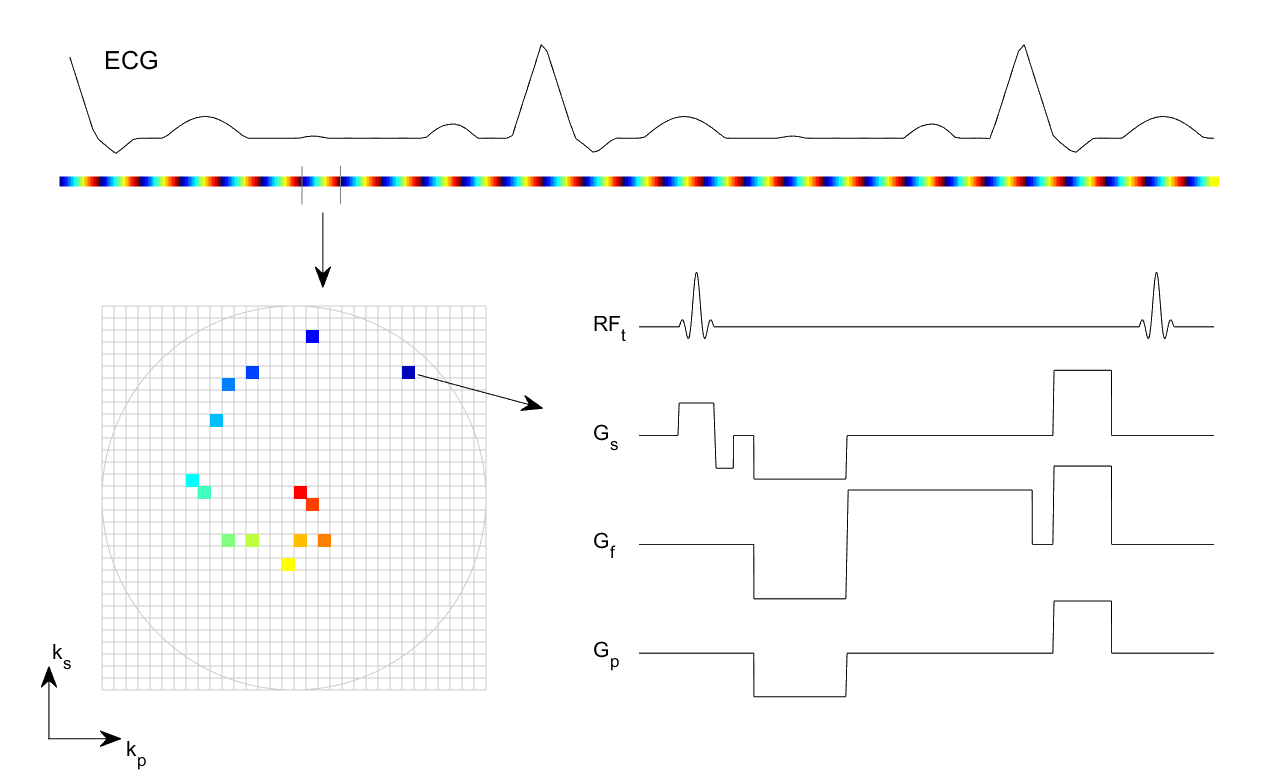
The 3D ungated spoiled gradient echo pulse sequence with a Rotating Cartesian K-Space (ROCK5) pattern is used in our study as shown in Fig. 1.
Experiments were conducted on 1 human (35-year-male) without contrast agent and 13 pigs (4-month-old) with gadolinium.
The sequence parameters for the human were TR/TE = 4.26/1.82 ms, RF = 5°, 400 Hz/px receiver bandwidth, matrix size of 256×256×80 mm3, 424 samples per readout, and spatial resolution of 1.25×1.25×1.5 mm3. The scan time was 8 minutes and 57 seconds.
The sequence parameters for the pigs receiving gadolinium were TR/TE = 3.52/1.4 ms, RF = 20°and 650 Hz/px receiver bandwidth, matrix size of 225×234×80 mm3, 370 samples per readout, and spatial resolution of 1.2×1.2×1.2 mm3. The scan time was 4 minutes and 26 seconds. Millimeter Wave Radar (mmWR6) is a non-contact respiratory triggering device and was recorded simultaneously with ECG signals.
All scans were performed on a 3T scanner (uMR890; United Imaging Healthcare, Shanghai, China) using a 12-channel chest coil array and a 16/48-channel spine coil array for signal reception.
Selective PCA self-gating method:
The 3D self-gating is usually implemented by interleaved k-readout lines through the k-space center along superior-inferior (SI) direction. The spatial variations in coil sensitivities and the heart’s motion make the SI projections obtained from different coils and locations have different weightings of cardiac and respiratory signals. To estimate the weightings of these two physiological signals, we introduced a parameter, Respiration to Cardiac Ratio (RCR) in the following equation
$$\mathrm{RCR}(n_c,n_x) = \frac{\int_{R_l}^{R_u}s(n_c,n_x,f)s_r(f)\mathrm{d}f}{\int_{C_l}^{C_u}s(n_c,n_x,f)s_c(f)\mathrm{d}f}.$$
Here, $$$s(n_c,n_x,f)$$$ represents the SI projection signal from $$$n_c$$$ channel and $$$n_x$$$ point at the frequency $$$f$$$; $$$R_l$$$ and $$$R_u$$$ denote the upper and lower cut-off frequencies for respiration and were set to 0.01Hz and 0.5Hz; $$$C_l$$$ and $$$C_u$$$ for cardiac signal were set to 0.5Hz and 2Hz for human and 0.5H and 3Hz for pigs. $$$s_r(f)$$$ and $$$s_c(f)$$$ are the estimated respiratory and cardiac spectrum.
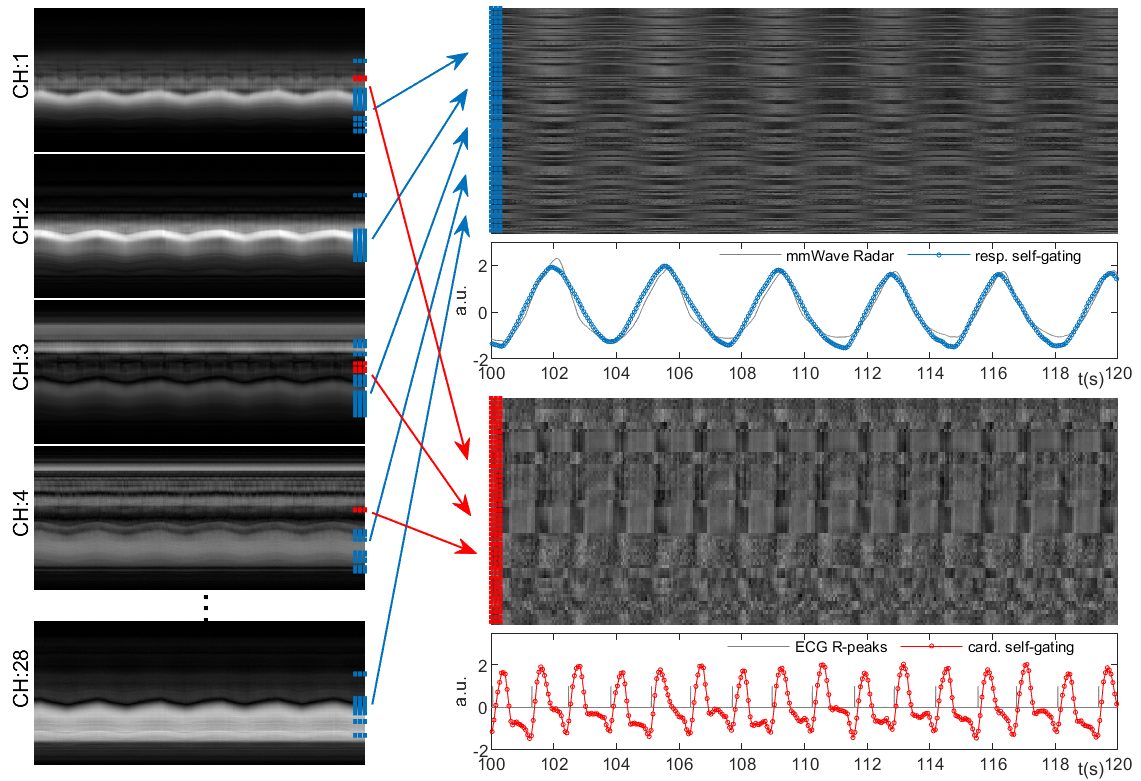
Points ranking in the bottom 0.5% based on RCR were selected and normalized to generate the cardiac signal using PCA, depicted in Fig. 2 (red). Similarly, points ranking in the top 10% based on RCR underwent the same process to generate the respiratory signal, as shown in Fig. 2 (blue). RCR was calculated twice using updating $$$s_r(f)$$$ and $$$s_c(f)$$$. In the first calculation, $$$s_r(f)$$$ and $$$s_c(f)$$$ were generated from the mass center of SI projection, while in the second calculation, they were obtained from the PCA of selected SI points based on first calculated RCR.
RESULTS
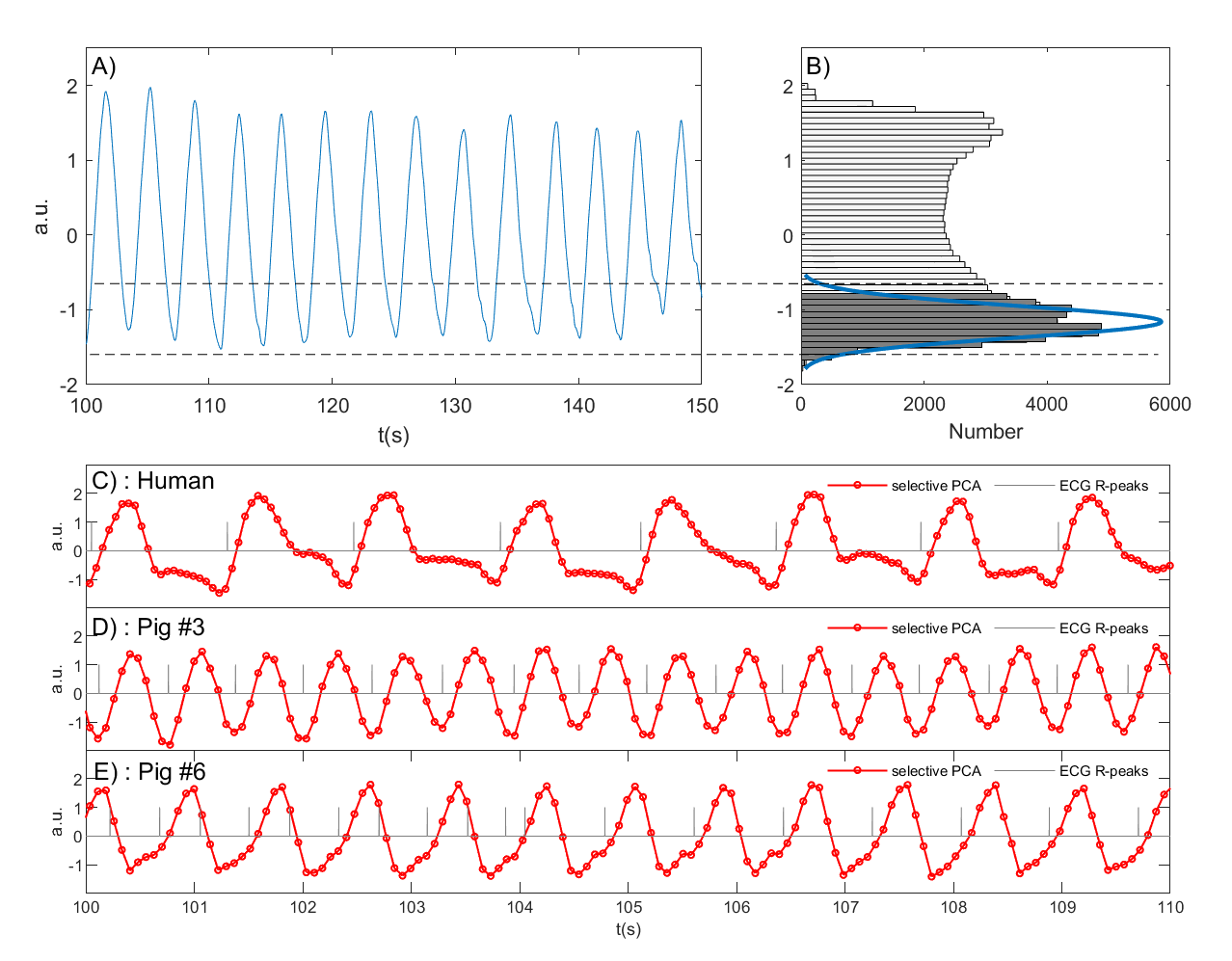
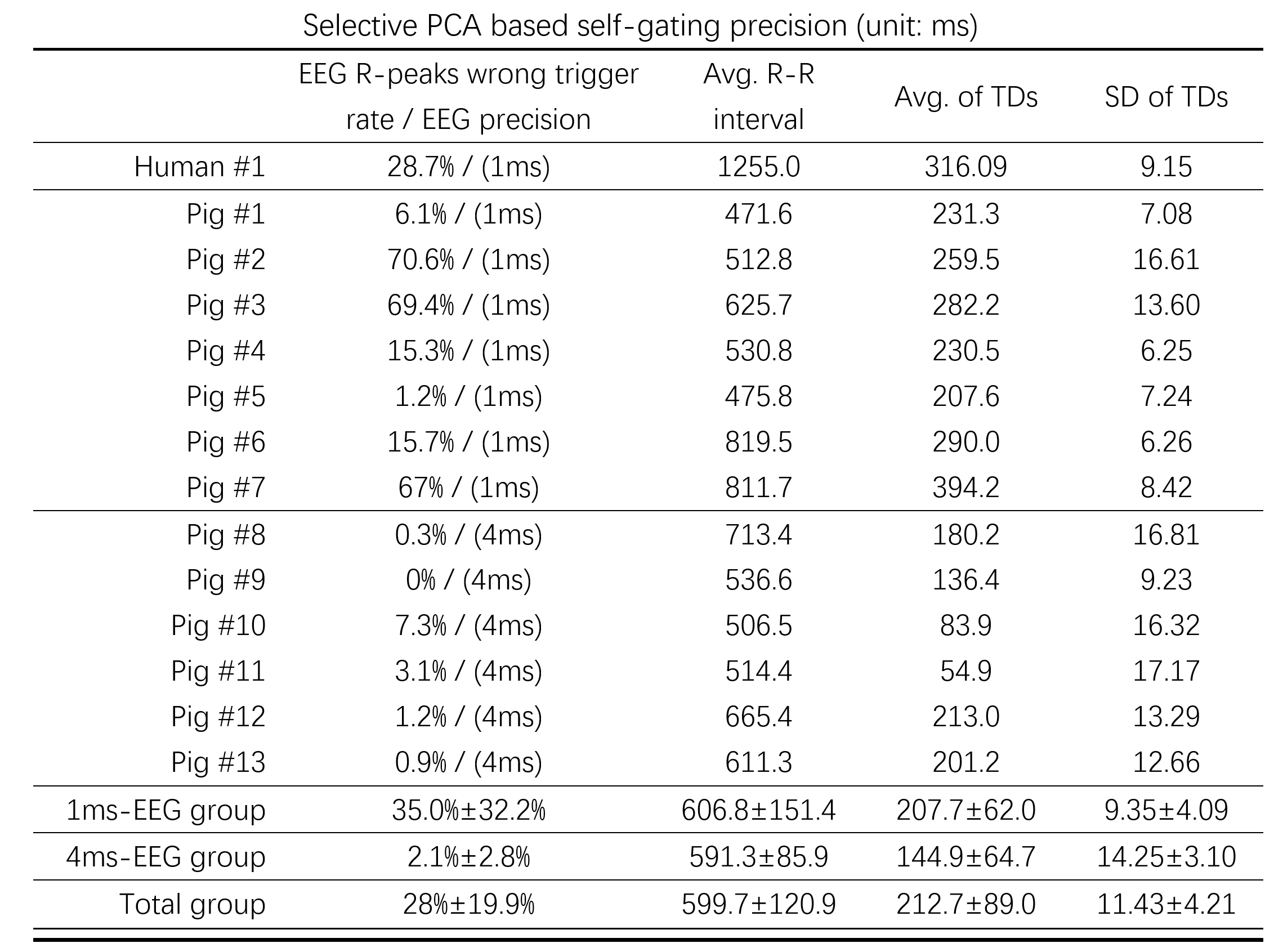
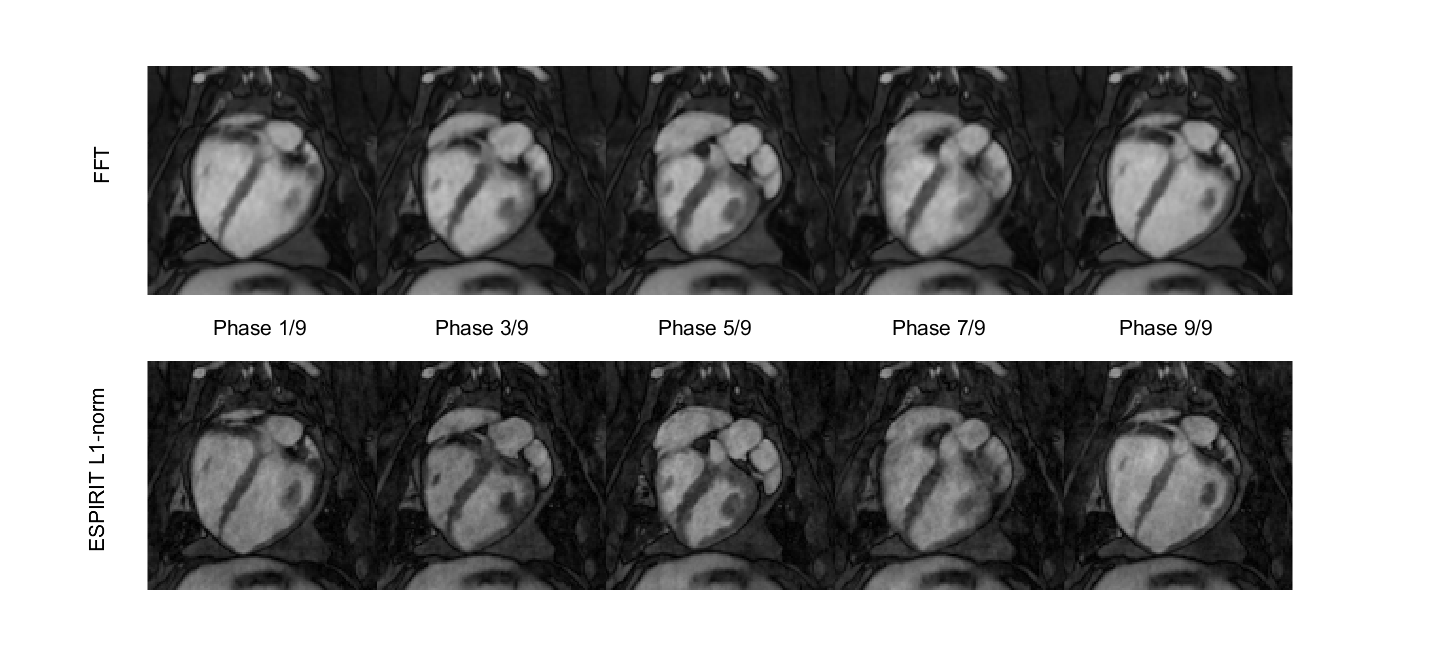
The respiratory and cardiac self-gating from 1 human and 3 pigs is shown in Fig. 3. The averaged time delays (TDs) between ECG R-peaks and self-gating peaks were calculated and listed in Fig. 4. The selective PCA temporal precision achieved 11.43ms in total. The MR cine images of #pig 3 are shown in Fig. 5. Blood pool and cardiac muscle can be clearly seen in the cardiac phases.DISCUSSION
The proposed RCR successfully selects respiration and heartbeat-related signals from mixed physiological signals in SI projections, accounting for coil sensitivity and heart location differences. This selection process enhances the cardiac signal while attenuating the respiratory signal, and vice versa for the respiratory signal. Compared with normal PCA self-gating methods, our method does not require a step to differentiate cardiac from respiratory gating signals. Since only 10% or 5% of the SI projection data are used for PCA, the calculation burden is highly reduced. During the experiment, the ECG had an R-peak detection failure rate of 35%, which strengthens the necessity for self-gating techniques.CONCLUSION
Selective PCA offers reliable self-gating for 3D cardiac MR Imaging, accurate to 11ms, and applicable in challenging ECG-gating situations, such as hairy chests and obesity, as well as high-fields ($$$\geq$$$3T). The method not only pinpoints the gating moment but preserves the entire cardiac dynamics, paving the way for enhanced arrhythmia CMR Imaging.Acknowledgements
No acknowledgement found.References
1. Larson AC, White RD, Laub G, McVeigh ER, Li D, Simonetti OP. Self‐gated cardiac cine MRI. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2004 Jan;51(1):93-102.
2. Liu J, Wieben O, Jung Y, Samsonov AA, Reeder SB, Block WF. Single breathhold cardiac CINE imaging with multi‐echo three‐dimensional hybrid radial SSFP acquisition. Journal of Magnetic Resonance Imaging. 2010 Aug;32(2):434-40.
3. Pang J, Sharif B, Fan Z, Bi X, Arsanjani R, Berman DS, Li D. ECG and navigator‐free four‐dimensional whole‐heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magnetic resonance in medicine. 2014 Nov;72(5):1208-17.
4. Di Sopra L, Piccini D, Coppo S, Stuber M, Yerly J. An automated approach to fully self‐gated free‐running cardiac and respiratory motion‐resolved 5D whole‐heart MRI. Magnetic resonance in medicine. 2019 Dec;82(6):2118-32.
5. Han F, Zhou Z, Han E, Gao Y, Nguyen KL, Finn JP, Hu P. Self‐gated 4D multiphase, steady‐state imaging with contrast enhancement (MUSIC) using rotating cartesian K‐space (ROCK): validation in children with congenital heart disease. Magnetic resonance in medicine. 2017 Aug;78(2):472-83.
6. Wang H, Li Y, Xia X, Hu L, Zhao J, Chen Q. Non-contact respiratory triggering for clinical MRI using frequency modulated continuous wave radar. InMedical Imaging 2021: Physics of Medical Imaging 2021 Feb 15 (Vol. 11595, pp. 268-275). SPIE.
Figures