1630
Predictive values of structural and functional magnetic resonance on neurological improvement in pediatric spinal cord injury1Radiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Neuro, Trauma
Motivation: Are the different prognosis of pediatric spinal cord injury (SCI) patients related to differences in brain structure and function? The research on this project has a good guiding significance for prognosis prediction and advanced intervention treatment.
Goal(s): To search for sensitive imaging indicators that can predict neurological outcomes in pediatric SCI patients.
Approach: Voxel-based morphometry (VBM) and fractional amplitude of low-frequency fluctuations (fALFF) were used to analyze the differences of brain structure and function in children with and without neurological improvement.
Results: The medial temporal gyrus may be used as neuroimaging biomarker to predict the prognosis of pediatric SCI.
Impact: MTG can be used as neuroimaging biomarker to predict the prognosis of children with SCI , providing imaging support for clinical stimulation of related brain regions to improve the probability of neurological improvement.
Introduction
Spinal cord injury without fracture or dislocation (SCIWOFD) is a kind of spinal cord injury (SCI) caused by external force, but without the imaging evidence of fracture or dislocation [1,2]. The prognosis of children with SCIWOFD varies greatly among individuals, with some children showing improvement in sensory function and others showing no improvement at all [3]. Could this difference in prognosis be related to the differences in brain structure and function of children with SCI? At present, there is no research on this issue, but this study is very instructive for the prognostic prediction and advanced interfere treatment, and also has important reference value for the selection of families with different economic conditions.Methods
57 pediatric SCIWOFD patients (age range: 6-12 years; male-to-female ratio: 6:51; ISNCSCI: 47A, 4B, 4C, 2D) were recruited in this study. We followed the patients for one year after SCIWOFD and divided them into two groups based on whether the patients had neurologic improvement (sensory scores assessed by ISNCSCI: including 27 patients without and 30 patients with neurological improvement). Images were obtained using a 3.0-T MRI system with a 12-channel phased-array head coil. High-resolution three-dimensional (3D) structural T1-weighted images were acquired for 6:59 min: repetition time (TR) / echo time (TE) / inversion time (TI) = 1800 ms / 2.13 ms / 1100 ms; flip angle (FA)=9°; number of slices=192; slice thickness=1 mm; field of view (FOV) =256× 256 mm2; matrix=256× 256; isotropic voxel size = 1×1×1 mm3. The parameters of resting-state functional magnetic resonance imaging (rs-fMRI) were acquired for 6.08 min: TR / TE = 2000 ms / 30 ms; FA=9°; number of slices=180; inter-slice gap=1 mm; slice thickness = 3 mm; FOV=220 × 220 mm2; matrix=64×64; isotropic voxel size=3.4×3.4×3.0 mm3.Post-processing of structural and rs-fMRI data were performed using Statistical Parametric Mapping (SPM) and Data Processing Assistant for Resting-State fMRI (DPARSF) implemented in MATLAB. Independent two-sample T-test was performed to assess the GMV and fALFF differences of the whole brain between pediatric SCIWOFD patients with and without neurological improvement using SPM. Then, partial correlation analyses and ETA correlation analysis were used to explore the correlations between the GMV and fALFF values and clinical indicators. Finally, receiver operating characteristic (ROC) curve was created by plotting the true positive rate against the false positive rate.
Results
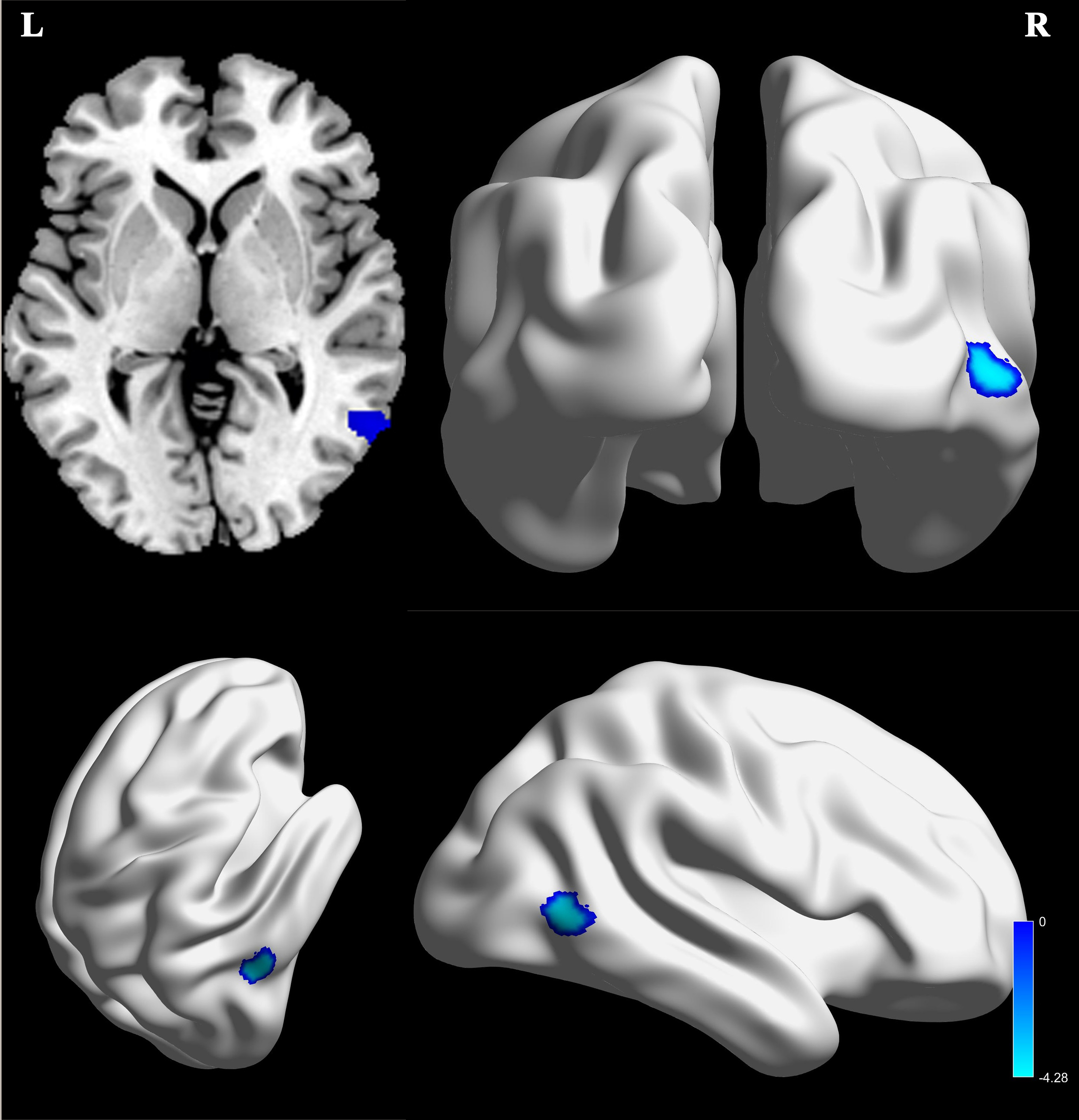
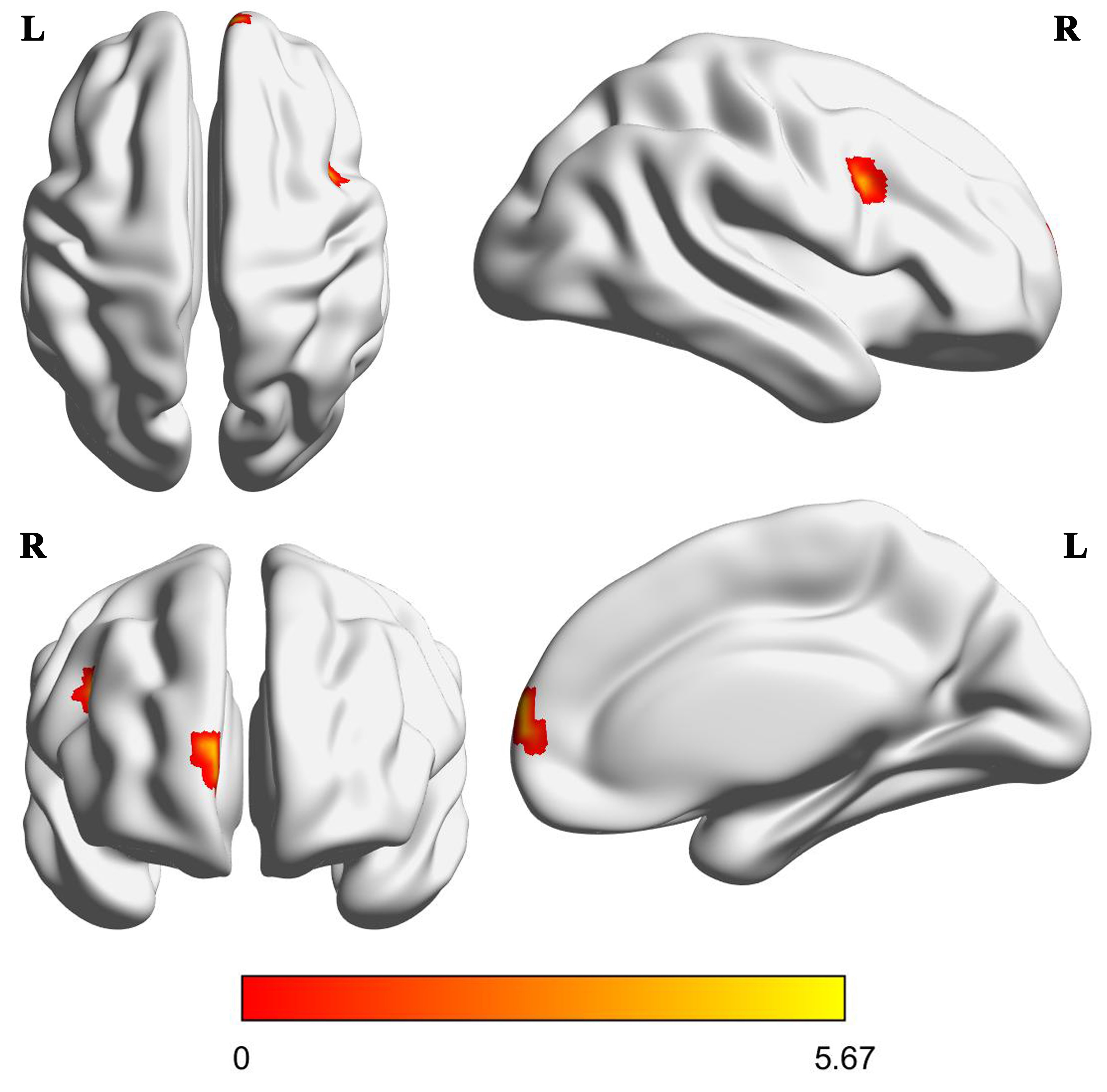
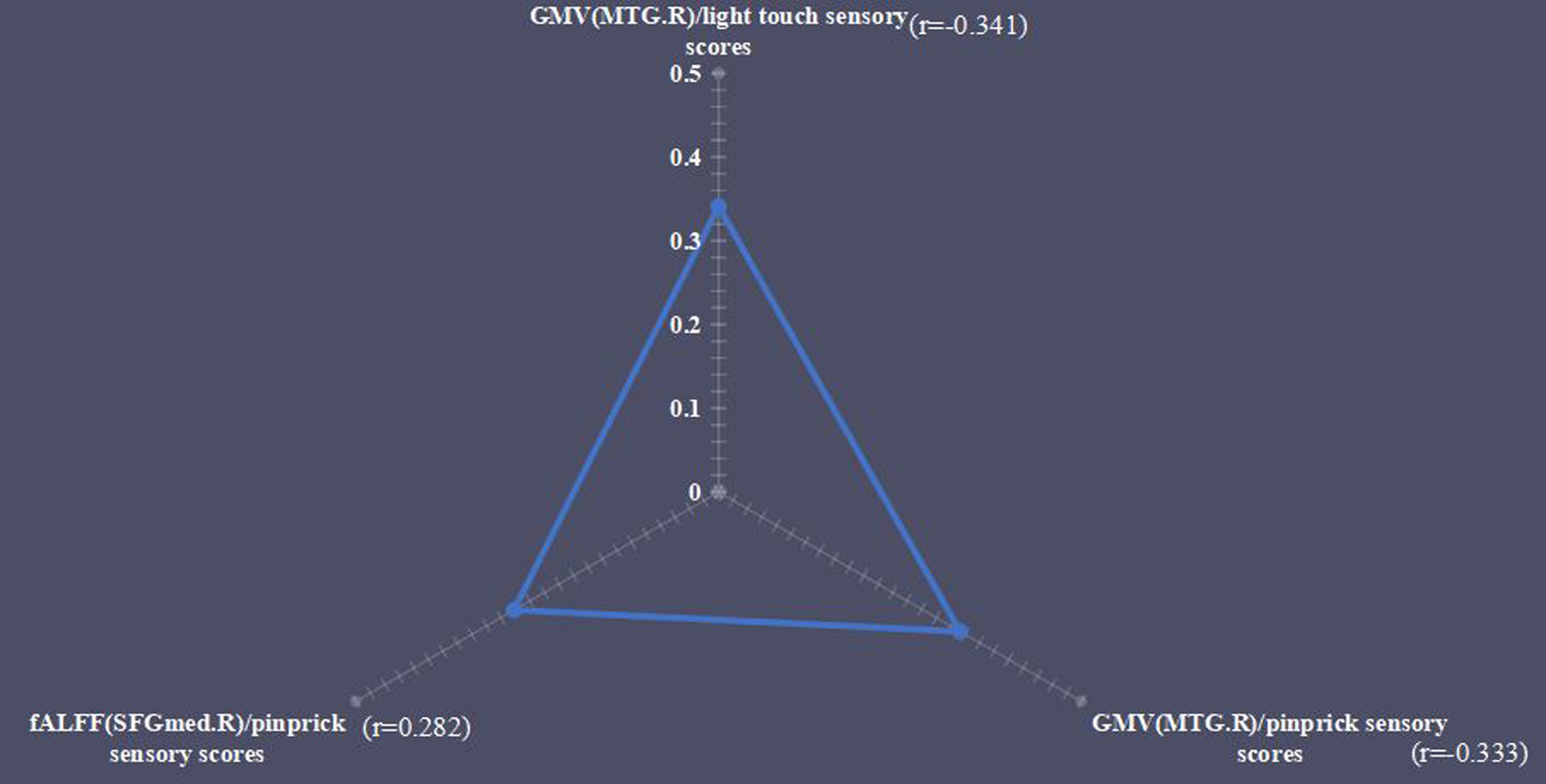
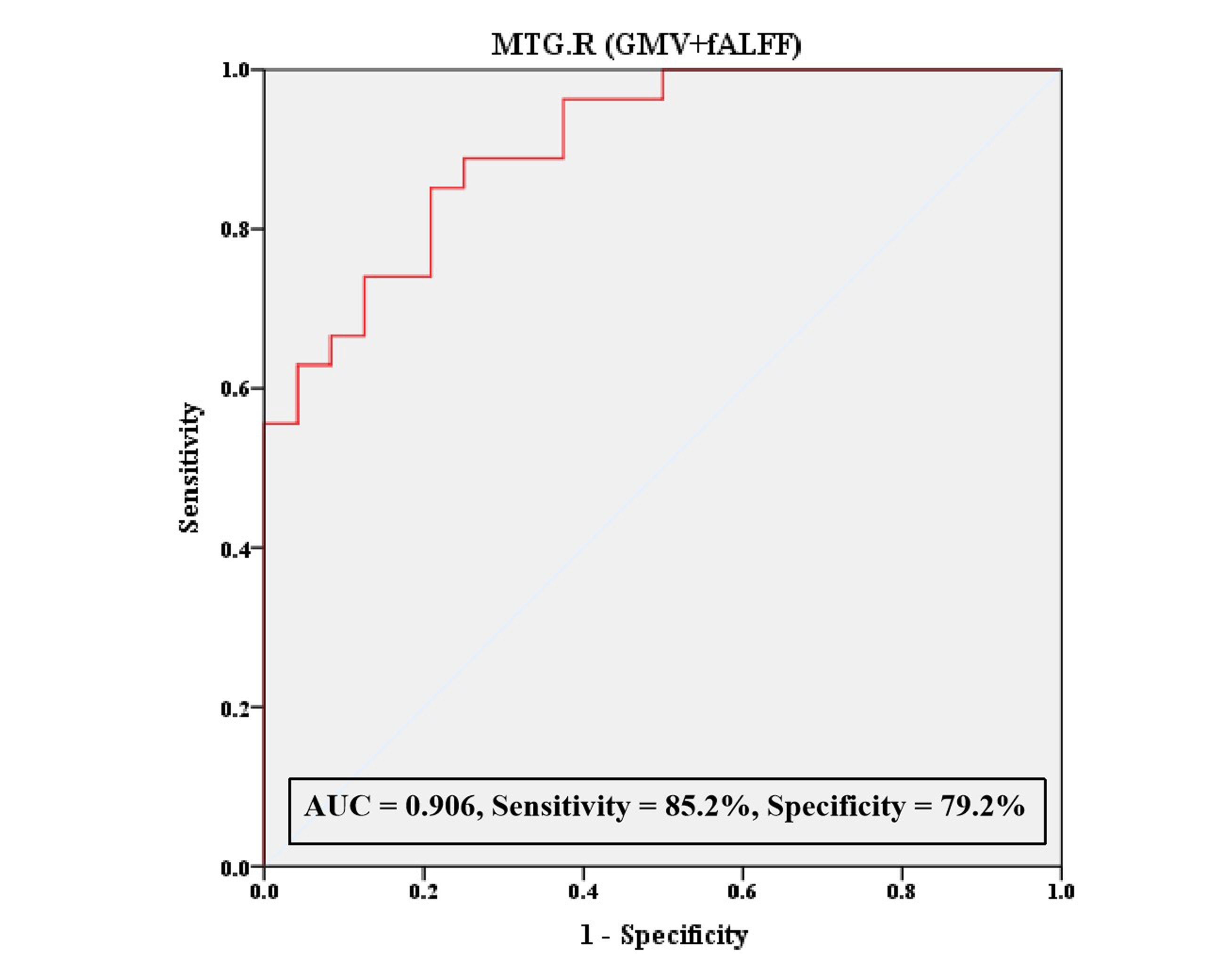
The present study characterized significant differences of GMV in right middle temporal gyrus (MTG), as well as differences of fALFF in right superior frontal gyrus, medial (SFGmed), MTG and inferior frontal gyrus, opercular part (IFGoperc) between the pediatric SCIWOFD patients with and without neurological improvement, which were partly correlated with the sensory scores and injury degree. Additionally, based on the simultaneous differences of the structure and function in right MTG, ROC analysis was performed with these two imaging measures as predictors in combination, with a relatively high sensitivity and specificity.Discussion
We hypothesized that the pediatric SCIWOFD patients with neurological improvement had smaller GMV, which is beneficial to the control of emotion and the recovery of sensory function in later stage [4-9]. The negative correlation between the GMV values of MTG and sensory scores further confirmed our hypothesis.Additionally, we speculated that the presence of high activation in these brain regions in pediatric SCIWOFD patients may be more conducive to the recovery of sensory function[10-16]. The positive correlation between the SFGmed and sensory scores further verified this conclusion.
The current study showed that the brain structure and function values in pediatric SCIWOFD patients were significantly correlated with the degree of injury, suggesting that brain structure and function indexes may be objective evaluation criteria for the degree of injury.
Based on the simultaneous changes of the structure and function in right MTG, the GMV and fALFF values of the right MTG were combined as predictors for a ROC analysis, suggesting that MTG, as an objective neuroimaging biomarker, may be used as a predictor of neurological improvement in pediatric SCIWOFD patients.
Conclusions
In summary, the present findings revealed significantly differences of GMV and fALFF between the pediatric SCIWOFD patients with and without neurological improvement, which were partly correlated with the sensory scores and injury degree. This suggested that the regions with brain structural and functional differences between the two groups, especially the right MTG (with differences of GMV and fALFF, simultaneously), may serve as neuroimaging biomarkers for the prediction of neurological improvement and provide image support for clinical stimulation of related brain areas in advance, so as to improve the probability of patients' neurological improvement.Acknowledgements
The authors thank the patients who participated in this study.References
1. Pang D, Wilberger JE Jr. Spinal cord injury without radiographic abnormalities in children. J Neurosurg 1982; 57, 114–29. 2. Walsh JW, Stevens DB, Young AB. Traumatic paraplegia in children without contiguous spinal fracture or dislocation. Neurosurgery 1983; 12, 439–45. 3. Zou Z, Teng A, Huang L, et al. Pediatric Spinal Cord Injury without Radiographic Abnormality: The Beijing Experience. Spine (Phila Pa 1976) 2021; 46(20), E1083-E1088. 4. Grabe HJ, Wittfeld K, Hegenscheid K, et al. Alexithymia and brain gray matter volumes in a general population sample. Hum Brain Mapp 2014; 35(12), 5932–5945. 5. Onitsuka T, Shenton ME, Salisbury DF, et al. Middle and inferior temporal gyrus gray matter volume abnormalities in chronic schizophrenia: an MRI study. Am J Psychiat 2004; 161(9), 1603–1611. 6. Mayer JD, Roberts RD, Barsade SG. Human abilities: emotional intelligence. Annu Rev Psychol 2008; 59, 507–536. 7. Petrides KV, Mikolajczak M, Mavroveli S, Sanchez-Ruiz MJ, Furnham A, Perez-Gonzalez JC. Developments in trait emotional intelligence research. Emot Rev 2016; 8(4), 335–341. 8. Tan YF, Zhang QL, Li WF, et al. The correlation between emotional intelligence and gray matter volume in university students. Brain Cogn 2014; 91, 100–107. 9. Wang S, Zhao Y, Wang X, et al. Emotional intelligence mediates the association between middle temporal gyrus gray matter volume and social anxiety in late adolescence. Eur Child Adolesc Psychiatry 2021; 30(12), 1857-1869. 10. Qiu C, Liao W, Ding J, et al. Regional homogeneity changes in social anxiety disorder: a resting-state fMRI study. Psychiatry Res 2011; 194, 47–53. 11. Jiang W, Li G, Liu H, et al. Reduced cortical thickness and increased surface area in antisocial personality disorder. Neuroscience 2016; 337, 143–152. 12. Park S, Ryu H, Lee JY, et al. Longitudinal changes in neural connectivity in patients with internet gaming disorder: a resting-state eeg coherence study. Front. Psychiatry 2018; 9, 252. 13. Brown CA, Schmitt FA, Smith CD, Gold BT. Distinct patterns of default mode and executive control network circuitry contribute to present and future executive function in older adults. Neuroimage 2019; 195, 320–332. 14. Bressler SL, Menon V. Large-scale brain networks in cognition: emerging methods and principles. Trends Cogn. Sci 2010; 14, 277–290. 15. Fu Z, Zhao M, He Y, et al. Divergent connectivity changes in gray matter structural covariance networks in subjective cognitive decline, amnestic mild cognitive impairment, and alzheimer’s disease. Front. Aging Neurosci 2021; 13, 686598. 16. Xue C, Qi W, Yuan Q, et al. Disrupted dynamic functional connectivity in distinguishing subjective cognitive decline and amnestic mild cognitive impairment based on the triple-network model. Front Aging Neurosci 2021; 13, 711009.Figures