1628
Evaluation of the utility of the portable MRI for the diagnosis of TFCC injury in wheelchair basketball players1Graduate School of Science and Technology, University of Tsukuba, Tsukuba, Japan, 2Department of Diagnostic and Interventional Radiology, Faculty of Medicine,, University of Tsukuba, Tsukuba, Japan, 3Department of Rehabilitation Medicine, University of Tsukuba, Tsukuba, Japan
Synopsis
Keywords: New Devices, New Devices
Motivation: Wheelchair basketball players have a high risk of TFCC injury, necessitating the development of a portable MRI for wheelchair users.
Goal(s): To demonstrate that the portable MRI is clinically feasible for the diagnosis of TFCC injuries in wheelchair basketball players.
Approach: We modified an existing portable MRI system for wheelchair use and imaged both wrists of seven players who had been selected for the Japanese women's wheelchair basketball team. We measured the signal-to-noise ratio of the wrist images and performed a clinical evaluation by two radiologists.
Results: Our portable MRI provided images of clinically detectable quality for TFCC injury.
Impact: The portable MRI system for wheelchair users improved in this study enables wheelchair users to assume the examination posture themselves and diagnose TFCC injuries. This is expected to expand the opportunities for MRI examinations of the wrists of wheelchair users.
Introduction
Wheelchair basketball is the most popular para-sport in the world. Wheelchair basketball players expose their upper extremities to double abuse in daily life and competition. As a result, they are more likely to injure the triangular fibrocartilage complex (TFCC)1. MRI is useful in the examination of the TFCC2-5. Studies using 1.5T clinical MRI have reported that wheelchair basketball players have a higher frequency of severe TFCC injuries than the average wheelchair user6. However, there are many problems with the use of clinical MRI, such as the difficulty for physically disabled people to assume the examination posture by themselves. Therefore, we considered using a portable MRI system mounted in a small car. This is expected to expand examination opportunities for wheelchair users by eliminating the need to travel to the hospital. We have recently developed a portable MRI system for healthy people, in which a permanent magnet and an MRI console were installed in a small car7,8. In this study, we modified this portable MRI system for wheelchair users and evaluated its applicability to the examination of TFCC.Materials and Methods
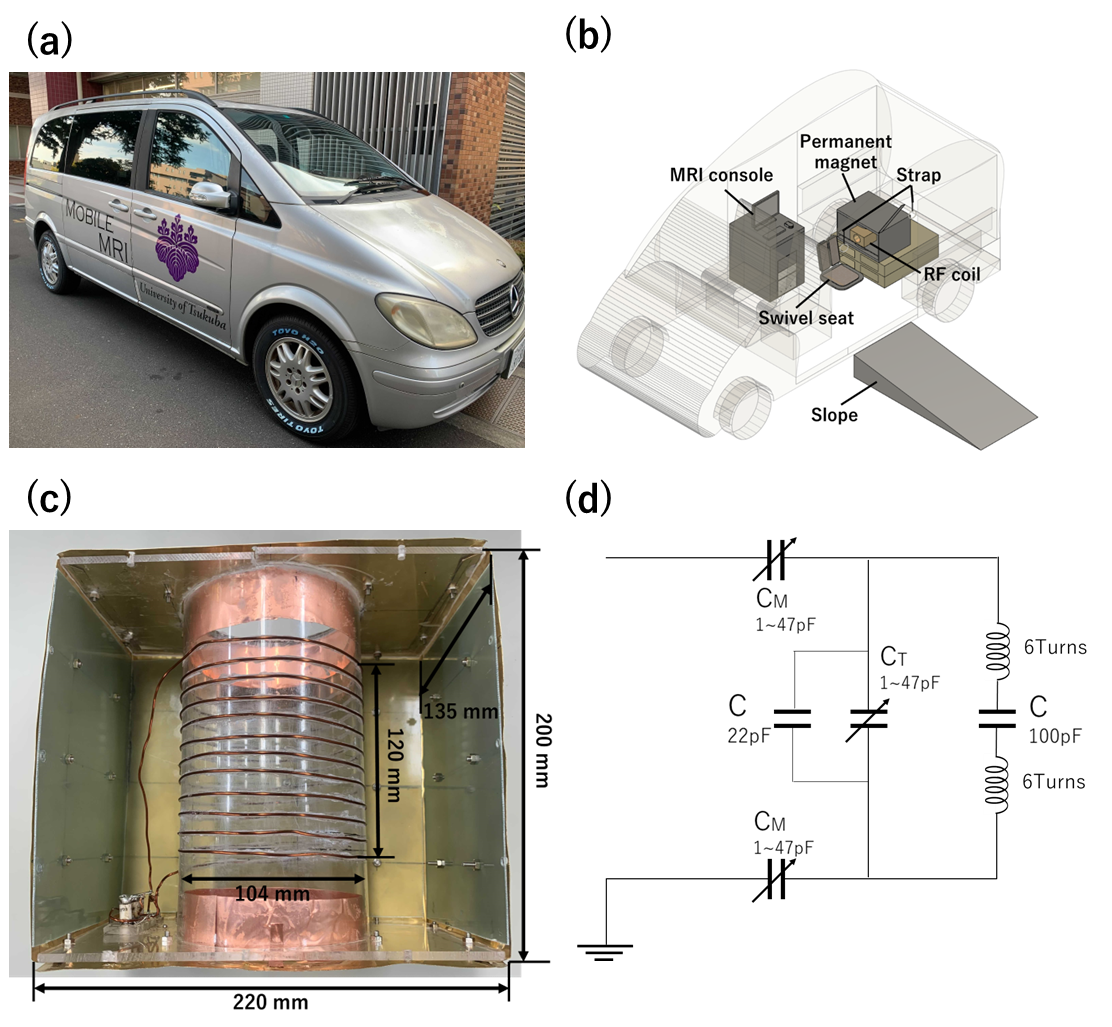
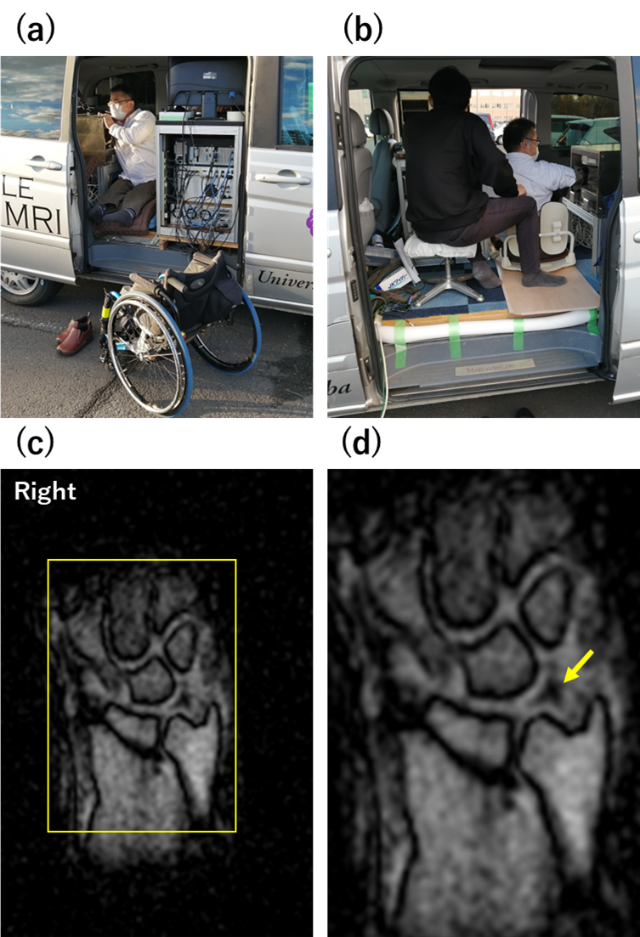
The portable MRI (Fig. 1(a,b)) consisted of a 0.2T permanent magnet (manufactured by NEOMAX Engineering Japan, 200 kg, gap 16 cm, 44 cm x 50 cm x 36 cm), a shielded RF probe, and a console (56 cm x 77 cm x 60 cm). To allow a wheelchair user to assume the examination posture without the assistance of others, posture-holding devices such as a ramp outside the vehicle, a suspension strap inside the vehicle, and a swivel chair for the physically challenged were installed; the RF probe (Fig. 1(c,d)) was newly designed and fabricated to be applicable to a wheelchair user. We imaged the right wrist of a regular wheelchair user (Fig. 2 (a, b)). In addition, we imaged both wrists of seven players who had been selected for the Japanese national women's wheelchair basketball team. The classification of the subjects' disability level followed the classification rules set by the International wheelchair basketball federation (IWBF)9. The imaging sequence was a 2D multislice T2*-weighted gradient echo. The imaging plane was the coronal plane. The parameters were TE/TR = 16ms/500ms, matrix size = 256 x 192, field of view (FOV) = 180mm x 180mm, slice thickness = 3mm, number of slices = 9, and measurement time = 1 minute 38 seconds/image. We measured the signal-to-noise ratio (SNR) of TFCC and Ulna in the acquired images. For clinical evaluation, two radiologists evaluated wrist images of a wheelchair basketball player. The evaluation was made on a 2-point scale: "n.p." for no findings and "injury" for injury.Results
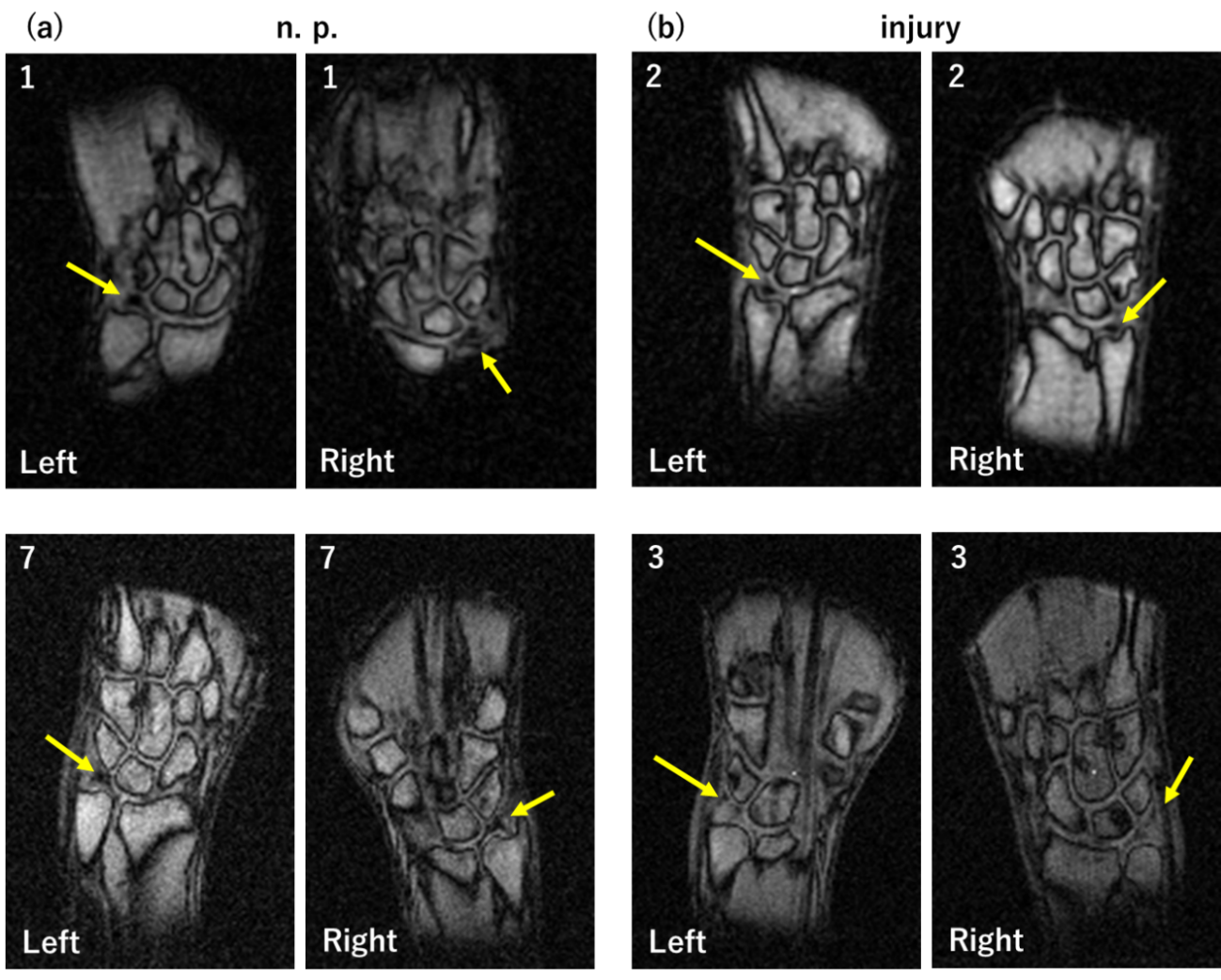
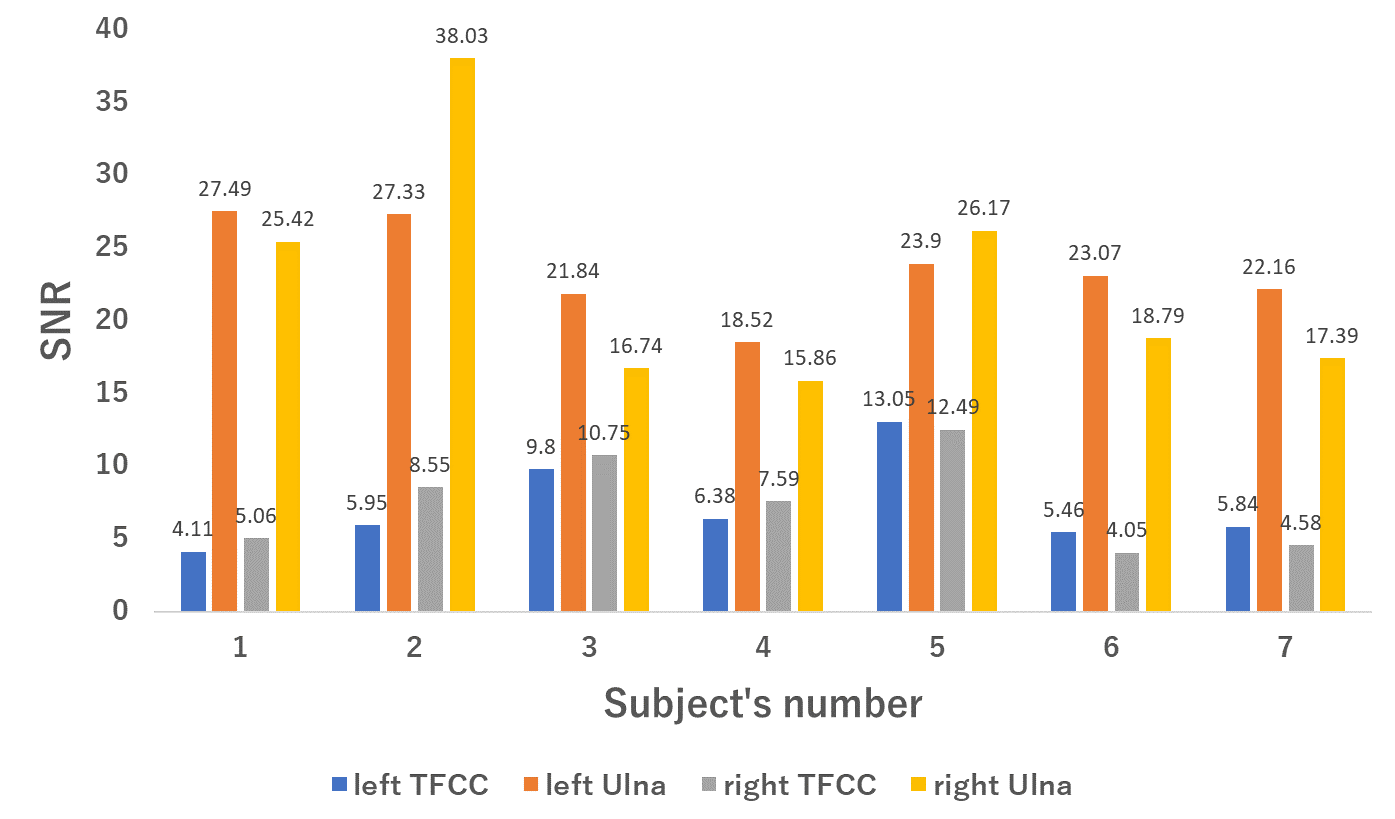
Figure 2 (c,d) shows the right wrist images of an ordinary wheelchair user. The SNRs of TFCC and Ulna were 13.6 and 28.2, respectively. Figure 3 shows a table of the results of the clinical evaluation of the wrist images of the 7 subjects in each disability class by the 2 radiologists. Of the 14 results of the clinical evaluation of wrist images from each of the 7 subjects, 6 were diagnosed as having no findings by 2 radiologists, 5 were diagnosed as having findings, and 3 were diagnosed as having findings by one of the radiologists. Figure 4 shows wrist images of a subject who had been selected for the Japanese national women's wheelchair basketball team. All images were of high enough quality to allow clinical evaluation. Figure 5 shows the graphs of SNR measurements of TFCC and Ulna of both wrists of the 7 subjects. In MRI, the SNR of TFCC was lower than that of Ulna because of its low signal.Discussion
We were able to obtain images of many subjects because we had set up an environment in which the wheelchair users themselves could assume the examination posture. All images obtained were of high quality. The system was shown to be usable for subjects with different disability classes. There were two cases in which the radiologist determined that both wrists had TFCC injuries. These subjects had much milder disability grades of 4 or 4.5. On the other hand, there were two cases in which there were no findings in either wrist, but the subjects had severe disabilities with disability classifications of 1 or 2. This suggests that subjects with less severe disabilities have greater potential wrist strain. These results demonstrate the clinical feasibility of TFCC testing in wheelchair users.Acknowledgements
No acknowledgement found.References
1. Palmer AK, Triangular fibrocartilage complex lesions: A classification. The Journal of Hand Surgery 1989; 14:594–606.
2. Tanaka T, et al., Comparison Between High-Resolution MRI With a Microscopy Coil and Arthroscopy in Triangular Fibrocartilage Complex Injury. The Journal of Hand Surgery 2006; 31:1308–1314.
3. Magge T, et al., Comparison of 3-T MRI and Arthroscopy of Intrinsic Wrist Ligament and TFCC Tears. American Journal of Roentgenology 2009; 192:80–85.
4. Anderson ML, et al., Diagnostic Comparison of 1.5 Tesla and 3.0 Tesla Preoperative MRI of the Wrist in Patients With Ulnar-Sided Wrist Pain. The Journal of Hand Surgery 2008; 33:1153–1159.
5. Iordache SD, et al., Prevalence of Triangular Fibrocartilage Complex Abnormalities on MRI Scans of Asymptomatic Wrists. The Journal of Hand Surgery 2012; 37:98–103.
6. Sakai M, et al., Characteristic MRI findings of the shoulder, elbow, and wrist joints in elite wheelchair basketball players. BMC Sports Sci Med Rehabil 2022; 14:141.
7. Miyasaka T, et al., Development of a Car-mounted Mobile MR Imaging System for Diagnosis of Sports-related Wrist Injury. MRMS 2023; 22:379–387.
8. Nakagomi M, et al. Development of a small car-mounted magnetic resonance imaging system for human elbows using a 0.2 T permanent magnet. Journal of Magnetic Resonance 2019; 304:1–6.
9. 2021-IWBF-Classification-Rules-Version-2022-12-12-vers-2-small. https://iwbf.org/wp-content/uploads/2022/12/2021-IWBF-Classification-Rules-Version-2022-12-12-vers-2-small.pdf
Figures