1627
Quantitative Evaluation of Postoperative Status after Meniscal Repair Using Synthetic Magnetic Resonance Imaging1The First Affiliated Hospital of Jinan University, Guangzhou, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Synthetic MR, Quantitative Imaging, MSK
Motivation: Post-surgical imaging evaluation of the meniscus is essential for clinicians to formulate personalized rehabilitation programs.
Goal(s): SyMRI can simultaneously quantify the T1, T2 relaxation time and PD of tissues, providing an objective method to reflect meniscus change.
Approach: The conventional MRI and SyMRI were performed before surgery, at 6 months, and 1 year after a surgery of meniscus repair, along with the Lysholm scores, to evaluate the postoperative recovery status.
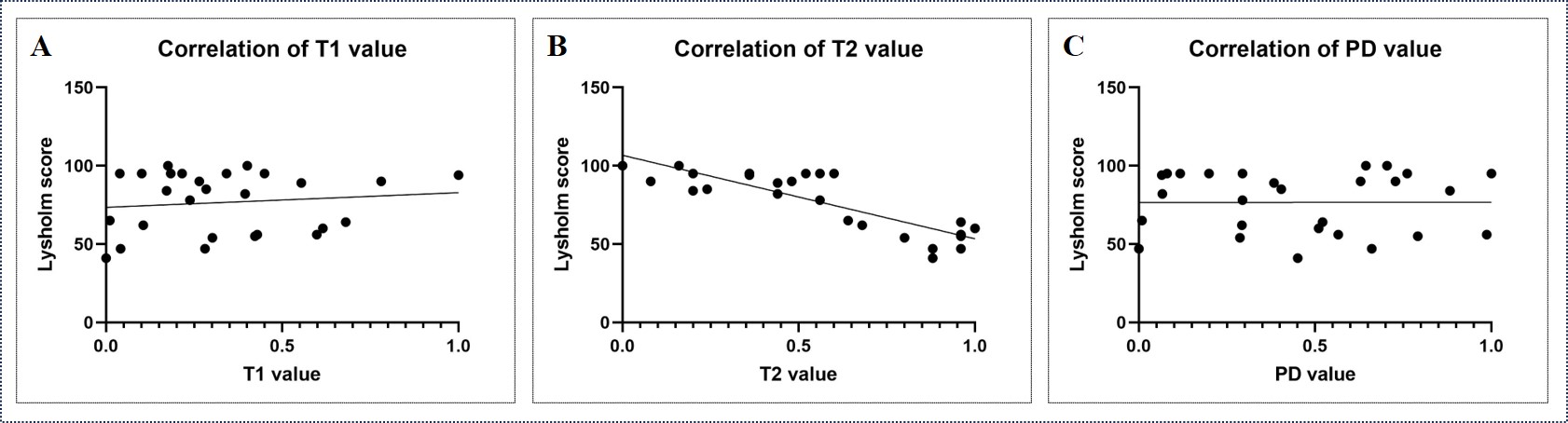
Results: Compared with the conventional MRI, T2 values presented a significant correlation with Lysholm scores and enabled to reflect follow-up postoperative function status of the meniscus.
Impact: The post-surgery abnormal meniscus signals fail to accurately distinguish the recurrent meniscus tears from postoperative changes during recovery period using conventional MRI. SyMRI can simultaneously provide contrast weighted MRI and quantification, giving an objective assessment of meniscus changes.
Introduction and Purpose
Evaluation of postoperative condition after meniscus repair surgery is essential for the further clinical treatment. Assessment of meniscal healing based on contrast MR arthrography and arthroscopy is relatively subjective and not easy to follow-ups [1]. Although arthroscopic assessment is considered the gold standard for meniscus injury, the invasive operation makes it not suitable for the follow-up menisci healing after surgery. Currently, the conventional MRI is widely used for tracking patient conditions after surgery, but the long-term abnormal high signal of the meniscus after surgery leads to the inability for accurately evaluating the postoperative changes of the meniscus. SyMRI can simultaneously quantify the T1, T2 relaxation time and PD of tissues in one scan to objectively reflect meniscus change and provide contrast weighted images for subjective evaluation. In this study, synthetic MRI (SyMRI) and conventional MRI was used in patients undergoing meniscus repair before surgery, 6 months and 1 year after surgery. Taking the Lysholm scores as the reference to evaluate the postoperative recovery status, our study aimed to explore whether the SyMRI including qualitative and quantitative maps could be used to accurately evaluate the postoperative condition of patients.Materials and Methods
Forty-nine patients who required an arthroscopic surgery were recruited from July 2022 to November 2022 and underwent both conventional MRI with the resolution of 2.1 ´ 2.1 ´ 2.4 in axial, sagittal and coronal views and sagittal SyMRI using 3.0T magnetic resonance scanner (Signa Premier, GE Healthcare, Waukesha, WI) before surgery as well as at 6 months and 1 year after surgery. Each patient completed the Lysholm form before MRI examination and twenty-seven patients completed all MR imaging. T1, T2 and PD values were measured on the MRI scanner console. One-way analysis of variance was used to analyze all three parameters of the same region of interests on the meniscus injury site; Pearson correlation analysis was used to assess the correlation between meaningful measurements and Lysholm scores.Results
T2 but not T1 and PD values showed significant difference between each two of time points (the pre-surgical, post-surgical 6-month and post-surgical 12-month time point, P < 0.001) (Fig. 1). The was no significant correlation between T1 or PD values and Lysholm scores, but there was a significant correlation between T2 values of meniscus and Lysholm scores (r= -0.854, P < 0.001) (Fig. 2).Discussion and Conclusion
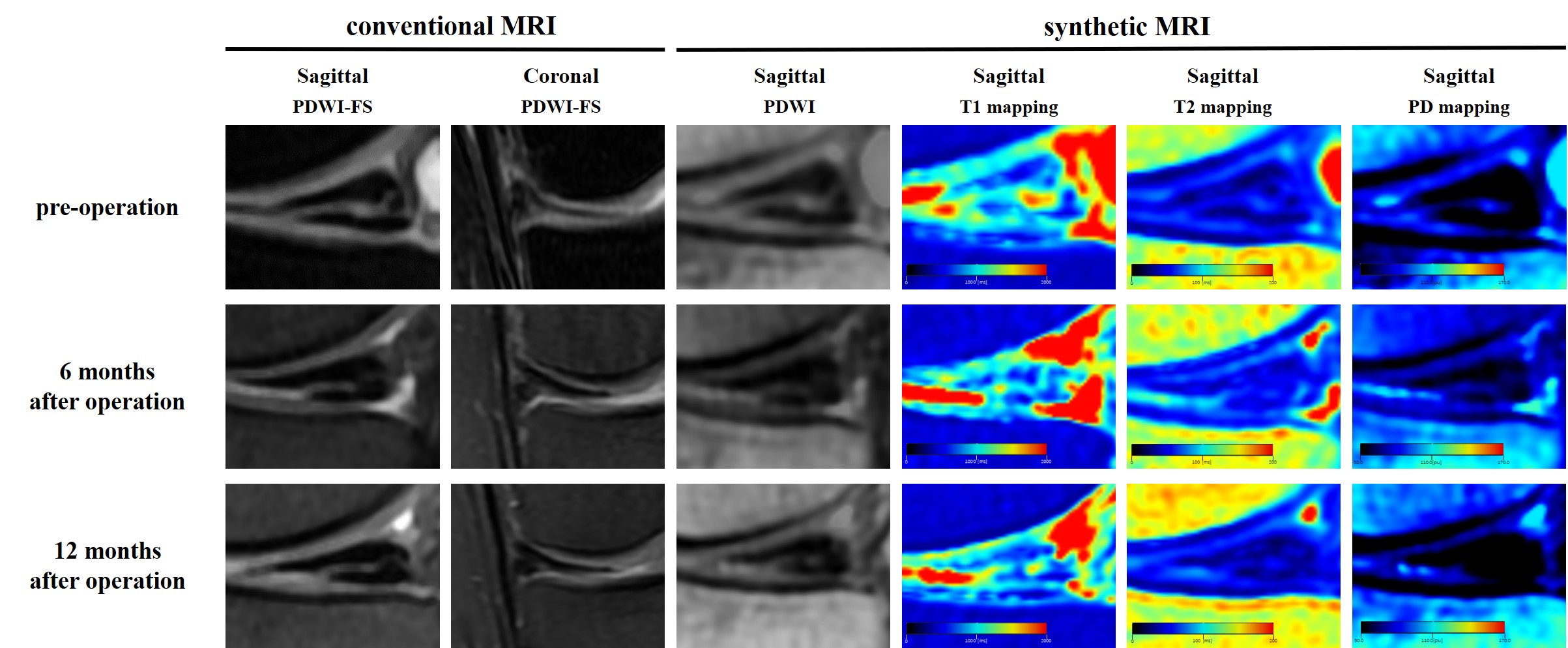
In this study, SyMRI-acquired T2 relaxation time showed a significant correlation with Lysholm scores, indicating recovery status of the collagen fibers in the extracellular matrix after meniscus surgery. Shorter T2 values of meniscus after surgery suggested a decreased water content as well as increased concentration of proteoglycans, recovery of collagen content and network integrity, thereby hinting inflammation is gradually diminished [2]. The meniscus appeared abnormal signals on conventional MRI especially in a short time after meniscus repair surgery. With the healing time of the meniscus, the abnormal signals in the meniscus gradually returns to the normal state, including the reduction of the depth, length, and area [3], but some patients possibly have recurrent meniscal tears during recovery. The abnormally high signal intensity in the meniscus remains for 1 year after surgery on conventional T2-weighted images, and thus recurrent meniscus tears may not be distinguished during meniscus recovery period [4]. The injury area with abnormal signal is normally wider due to swelling of the surgical site on both conventional MRI and synthetic contrast MRI. The high signal intensity on PD-weighted image was no significant change at the surgical site for 1 year after operation. Besides, the morphology, size and signal intensity of abnormal meniscus signals on fat-saturated PD-weighted images and synthetic PD-weighted images were similar. In contrast, the T2 values of SyMRI at the same surgical site gradually decreased after meniscus repair surgery, suggesting the meniscus is still recovering (Fig. 3). Moreover, T2 values were negatively correlated with the Lysholm scores. To sum up, SyMRI generated compatible contrast images to conventional MRI and computed T2 map to assist evaluation of the postoperative meniscus recovery, suggesting SyMRI could be a clinical tool to assist discrimination of operation-induced edema from recurrent meniscal tears.Acknowledgements
Funding: This project was supported by the Science and Technology Projects in Guangzhou, China (2023A03J0609), Guangdong Basic and Applied Basic Research Foundation (2022A1515110630).References
[1] Miao Y, Yu JK, Ao YF, Zheng ZZ, Gong X, Leung KK. Diagnostic values of 3 methods for evaluating meniscal healing status after meniscal repair: comparison among second-look arthroscopy, clinical assessment, and magnetic resonance imaging. Am J Sports Med. 2011;39(4):735-742.
[2] Koff MF, Amrami KK, Kaufman KR. Clinical evaluation of T2 values of patellar cartilage in patients with osteoarthritis. Osteoarthritis Cartilage. 2007;15(2):198-204.
[3] Zhao M, Zhou Y, Chang J, et al. The accuracy of MRI in the diagnosis of anterior cruciate ligament injury. Ann Transl Med. 2020;8(24):1657
[4] Heuck A, Woertler K. Posttreatment Imaging of the Knee: Cruciate Ligaments and Menisci. Semin Musculoskelet Radiol. 2022;26(3):230-241.
Figures
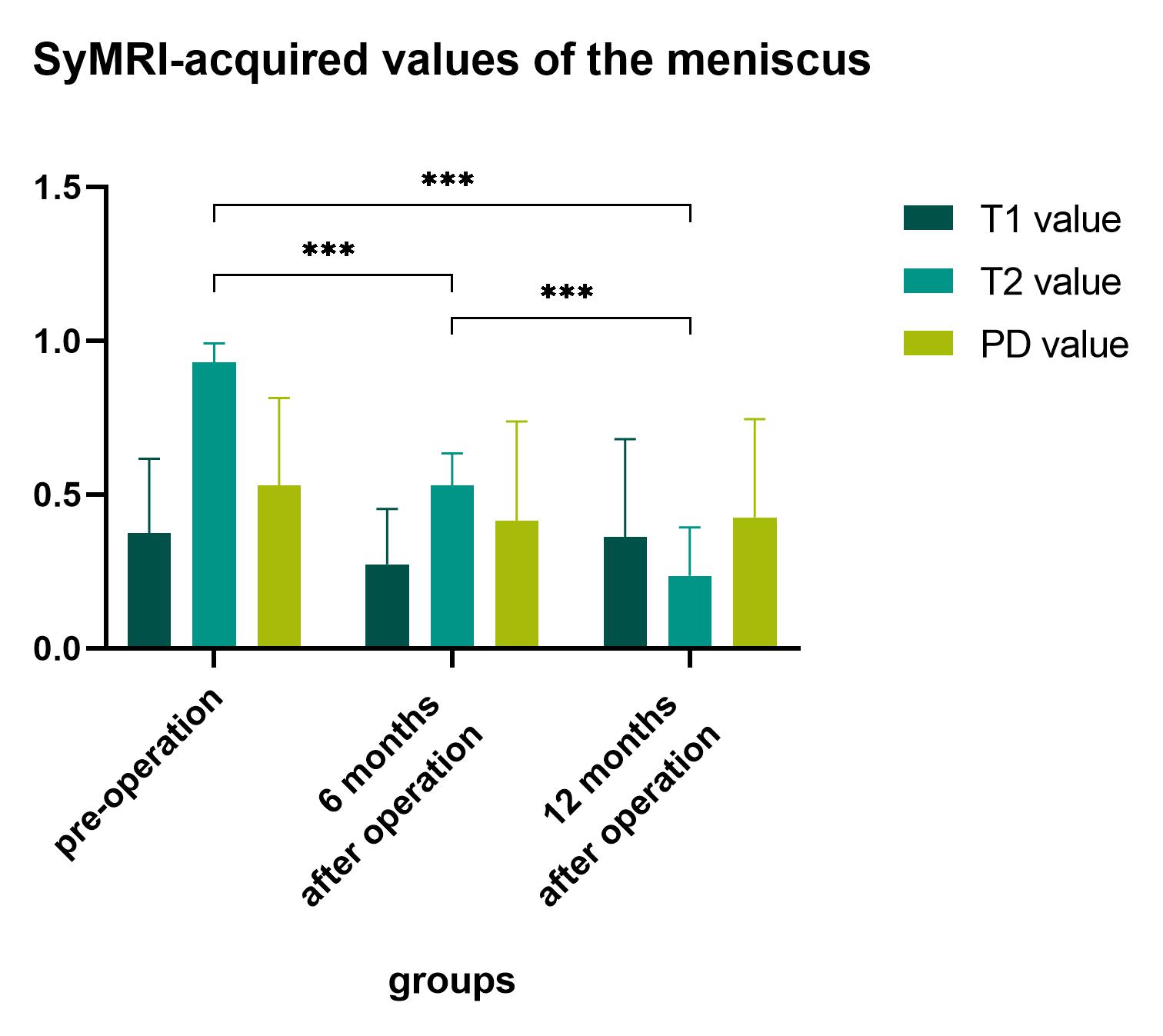
Figure 1: Normalized T1, T2 and PD values at the pre-surgical, post-surgical 6-month and post-surgical 12-month time points. T2 but not T1 and PD values showed significant difference between each two of time points. (***: P < 0.001)