1619
Increased brain entropy and its association with cognitive function following mild traumatic brain injury1Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland Baltimore, Baltimore, MD, United States, 2Center for Advanced Imaging Research, University of Maryland Baltimore, Baltimore, MD, United States
Synopsis
Keywords: Traumatic Brain Injury, Traumatic brain injury, brain entropy
Motivation: Mild traumatic brain injury (mTBI) is a prevalent neurological condition involved with physical, cognitive, and emotional impairments. Brain dynamics measured with sample entropy and its association with cognitive functions in mTBI patients remains unexplored.
Goal(s): We aim to investigate brain entropy changes in mTBI as compared to non-TBI control patients and explore their potential associations with cognitive function in mTBI patients.
Approach: Brain entropy mapping was applied based on rs-fMRI images.
Results: Results show hyper-entropy within hippocampus and para-hippocampal gyrus which has significant negative association with cognitive scores related to working memory and processing speed.
Impact: This study underscores the promise of brain entropy analysis as a valuable addition to mTBI research, with implications for improved diagnostic and treatment strategies.
Introduction
Mild traumatic brain injury (mTBI) is a prevalent neurological condition leading to short- or long-term cognitive impairments [1]. Since these consequences are often not accompanied by structural damages, studying brain activity is critical to understanding their underlying mechanisms. Entropy is a physically meaningful property. Functional brain entropy (BEN) indicates the information processing capacity and the irregularity of brain activity which may be affected by TBI. This study aims to fill a knowledge gap of BEN in mTBI and its association with cognitive impairment using resting state fMRI (rs-fMRI).Methods
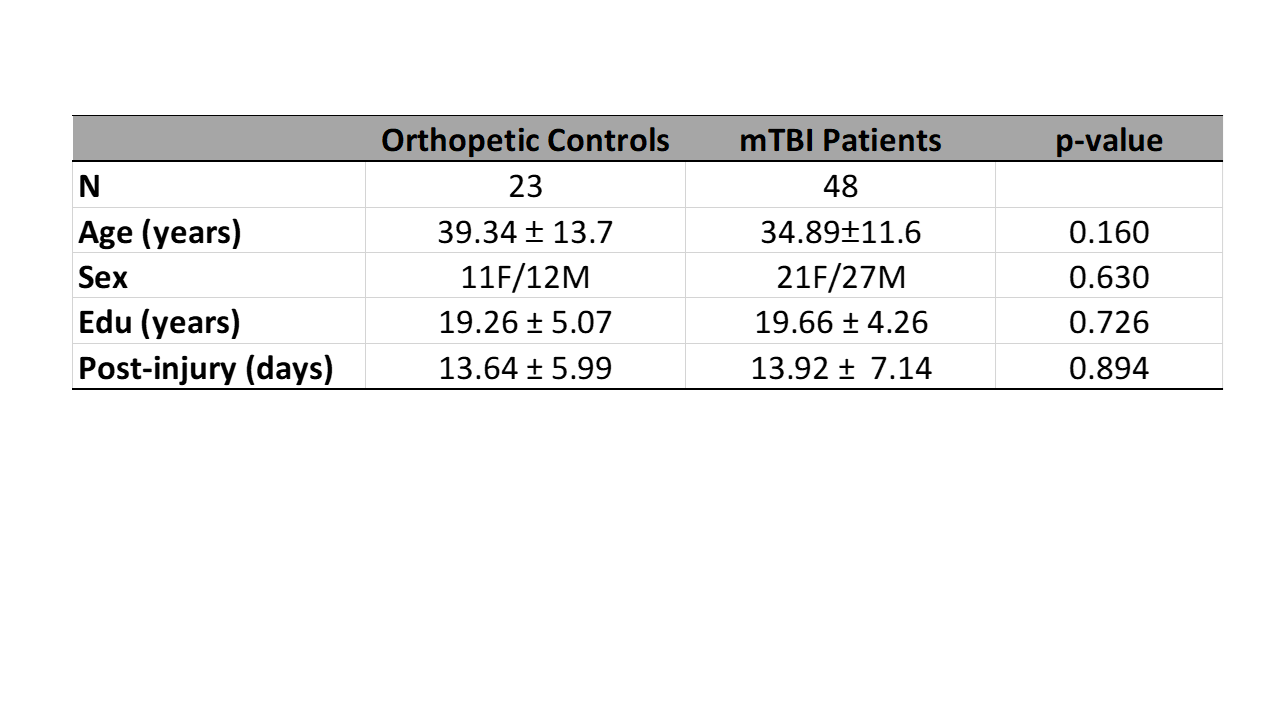
Subjects and Cognitive Tests: 50 mTBI patients and 23 age- and sex-matched non-TBI control patients were recruited from the Dr. R Adams Cowley Shock Trauma Center. All participants provided informed written consent and underwent MRI scans within 1 month of their injuries. Two participants were excluded due to severe motion artifacts in rs-fMRI data. Of the remaining participants, 64 successfully completed cognitive tests using the NIH Toolbox Cognition Battery.MRI Data Acquisition: The rs-fMRI data were acquired on a Siemens Prisma 3T MRI scanner with a 2D multi-band EPI sequence with TR/TE = 943/30 ms, resolution = 3.0 × 3.0 × 3.0 mm3, slice-acceleration factor = 4, and 500 volumes. The 3D MPRAGE T1w images were acquired with TR/TE = 4000/3.37 ms, TI = 1400 ms, resolution = 1.0 ×1.0 × 1.0 mm3.
MRI Data Preprocessing and Denoising: The rs-fMRI images were preprocessed and denoised using CONN Toolbox 22a [2], including realignment, slice-timing correction, outlier identification, direct normalization into standard MNI152 template space with resolution of 2x2x2 mm3, and spatial smoothing with 6mm FWHM Gaussian kernel. The T1w images were segmented into GM, WM and CSF. The aCompcor was used for denoising with signal confounders derived from WM and CSF, motion parameters, and the identified outlier scans. Additionally, a band-pass filter (0.008 Hz < f <0.09 Hz) was applied. Finally, a quality-control procedure was performed.
BEN Mapping: The BEN Mapping Toolbox (BENtbx) was used to calculate BEN maps using the preprocessed rsfMRI time series [3]. The two parameters involved in BEN mapping: the embedding vector length m and the distance threshold r were set to be m = 3 and r = 0.6 based on the literature [3].
Statistical Analysis: A generalized linear model (GLM) was employed, controlling for age, sex, and education, to assess brain entropy difference between mTBI and controls. Significance was set as uncorrected voxel-wise p-value < 0.008, and a cluster-wise FDR p-value < 0.05 for multiple comparison correction. Pearson correlation was conducted between brain entropy values within the significant clusters and age-corrected cognitive test scores with significant level of p-value < 0.05.
Results
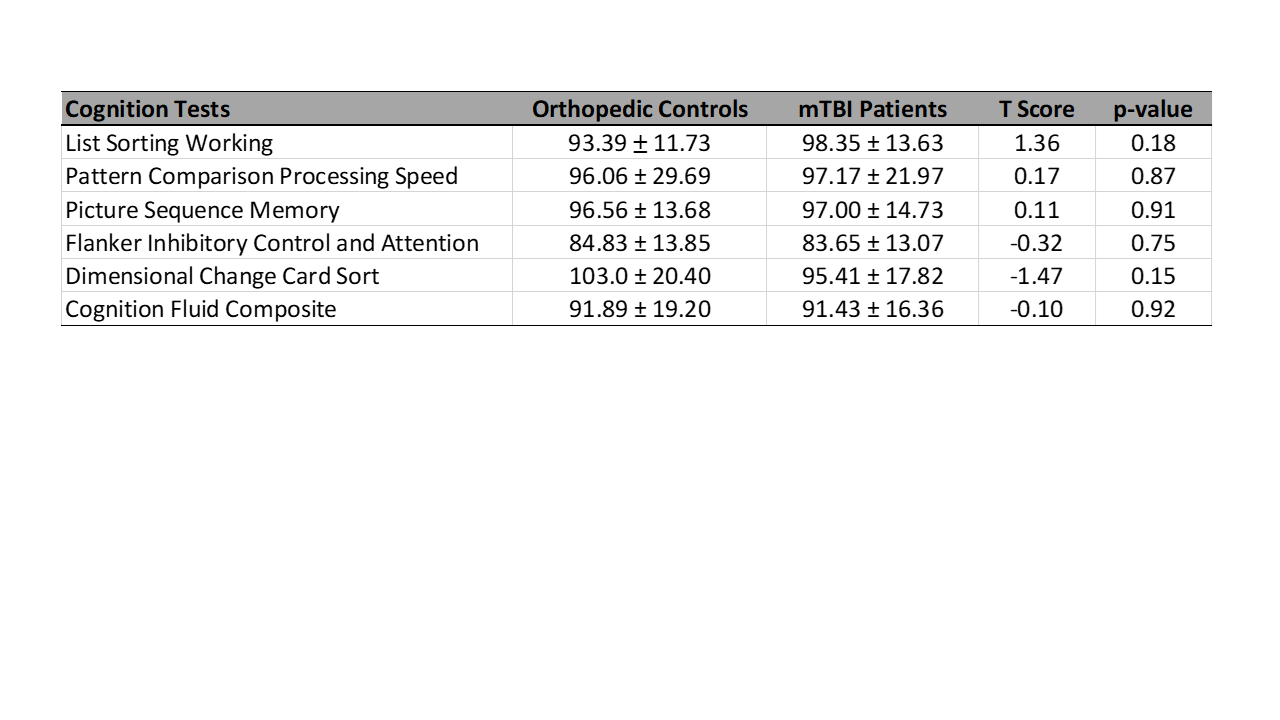
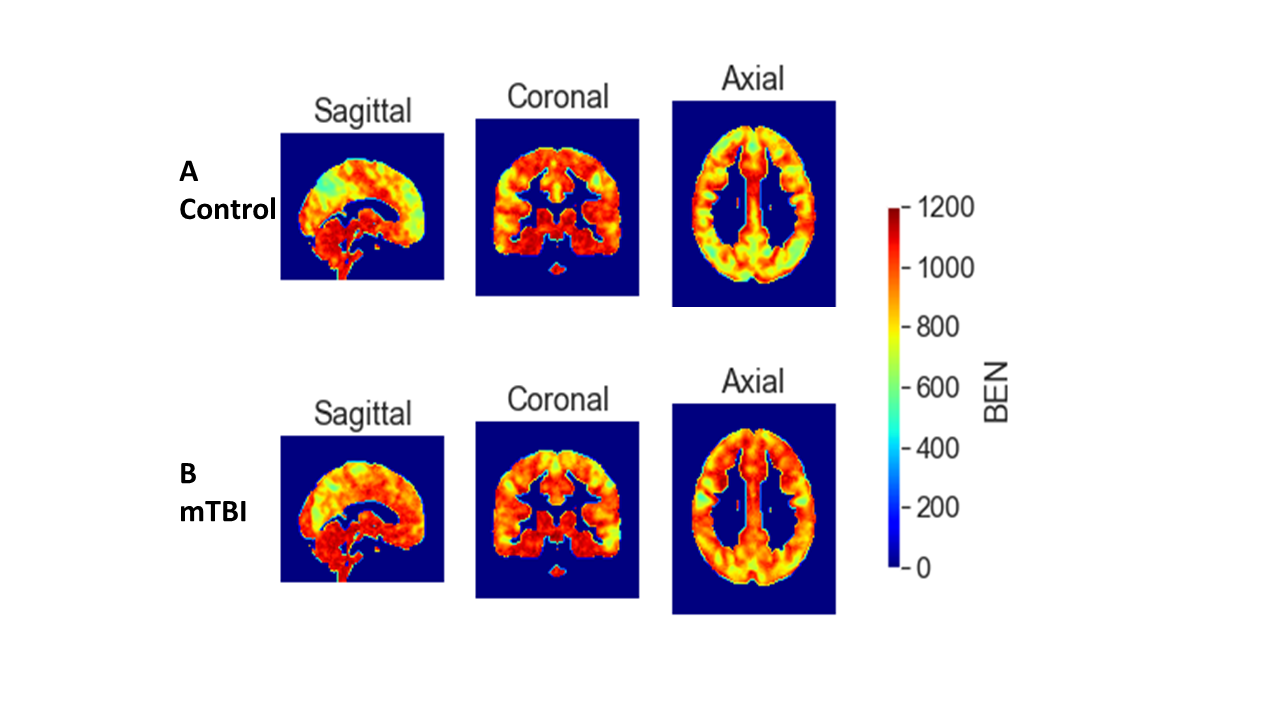
Table 1 and Table 2 indicate no significant differences in age, gender, education, or cognitive scores between mTBI and control patients.Figure 1 illustrates examples of brain entropy distribution for both control and mTBI patients, consistent with existing literature [4]. The TBI patient shows an overall higher level of brain entropy than control.
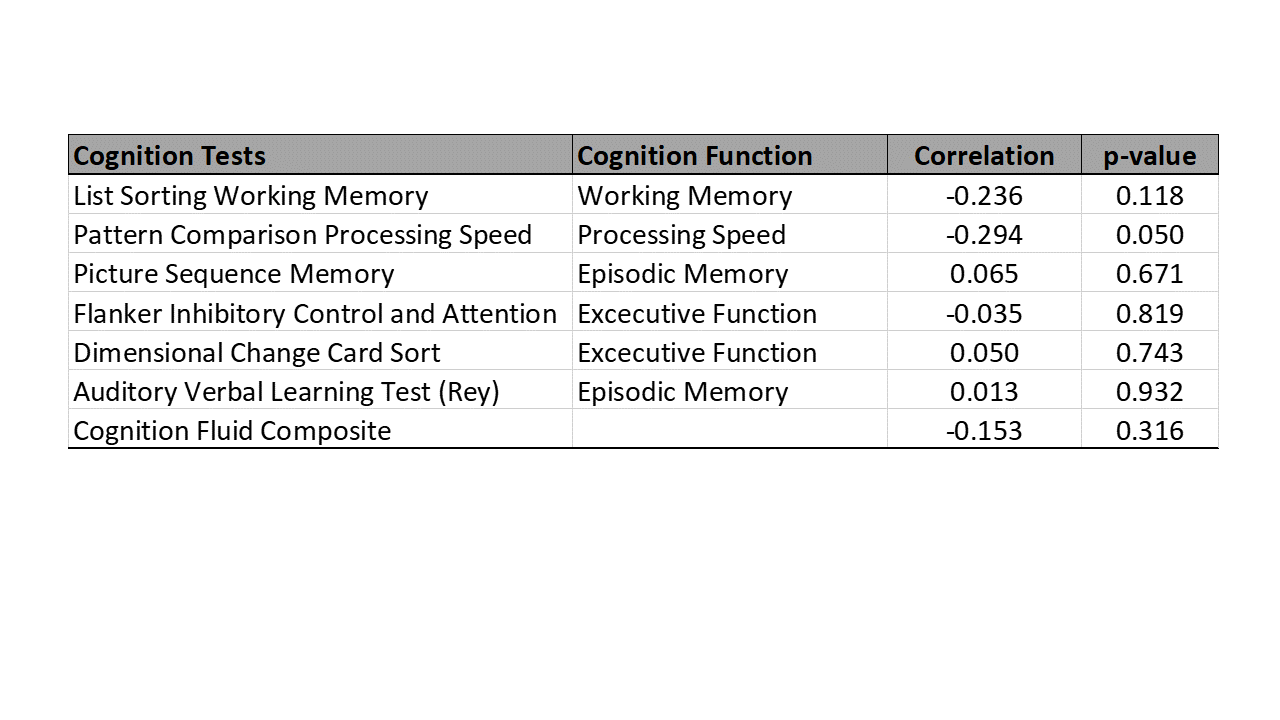
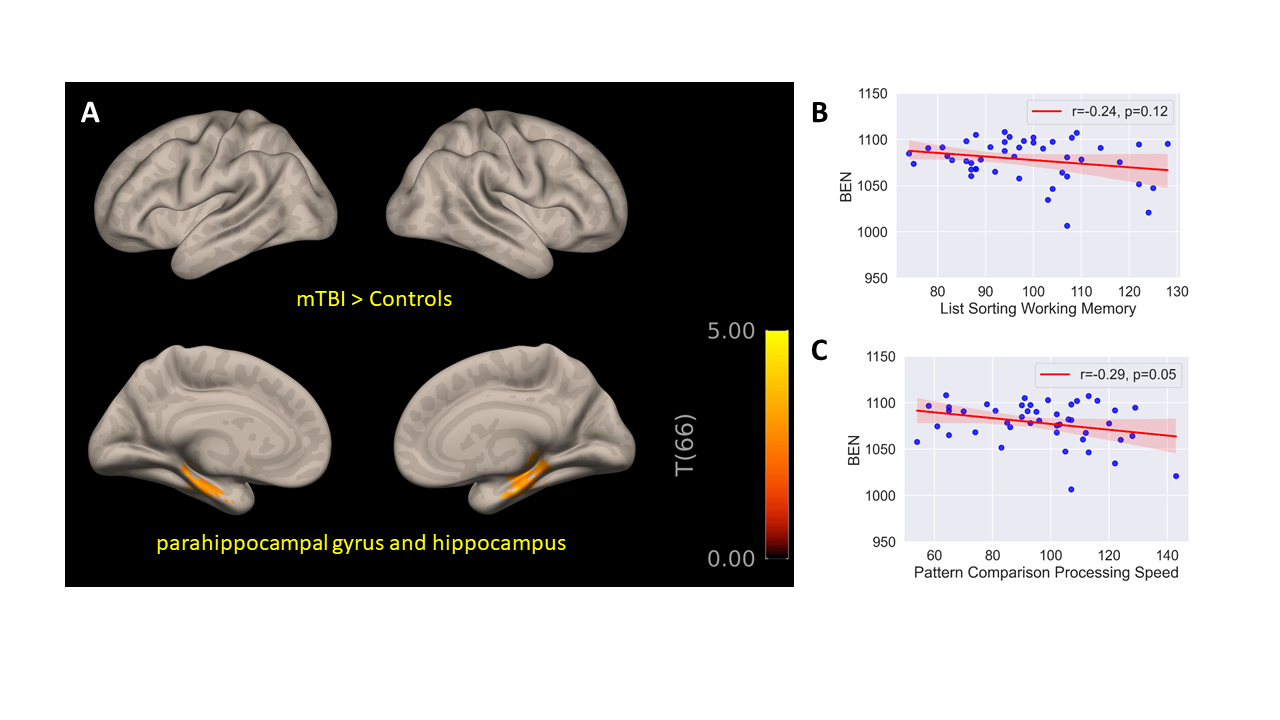
Figure 2A reveals elevated entropy levels in the para-hippocampal gyrus and hippocampus of mTBI patients compared to controls. Additionally, Figures 2B and 2C demonstrate a significant negative correlation between brain entropy in these regions and Pattern Comparison Processing Speed test scores (r = -0.294, p = 0.050). A strong negative trend, though not statistically significant, is observed with List Sorting Working Memory test scores (r = -0.236, p = 0.118). Table 3 confirms the absence of significant associations in other cognitive test scores.
Discussion
Our study explores the link between mTBI, cognitive function, and brain entropy. While cognitive tests showed no significant differences between mTBI and non-TBI control patients, brain entropy analysis revealed elevated entropy in the hippocampus and para-hippocampal gyrus, crucial for memory function. Furthermore, we observed a significant negative correlation between brain entropy and cognitive scores related to working memory and processing speed, suggesting that higher entropy is associated with poorer cognitive performance. Consistent with research on aging and diseases like Alzheimer's, higher cognitive entropy may indicate more adaptive cognitive processes [3]. In mTBI patients, increased entropy in memory-related brain regions may serve as compensation to maintain cognitive function.In conclusion, this study underscores the promise of brain entropy analysis as a valuable addition to mTBI research, with implications for improved diagnostic and treatment strategies.
Acknowledgements
The study was conducted at University of Maryland School of Medicine Center for Innovative Biomedical Resources, Translational Research in Imaging @ Maryland (CTRIM) – Baltimore, Maryland. The study is supported by NIH under grant 5R01NS105503.References
1. McInnes, K., et al., Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review. PLoS One, 2017. 12(4): p. e0174847.
2. Nieto-Castanon, A., Handbook of functional connectivity magnetic resonance imaging methods in CONN. 2020, Hilbert Press: Boston, MA. p. 3-16.
3. Wang, Z., et al., Brain entropy mapping using fMRI. PLoS One, 2014. 9(3): p. e89948.
4. Wang, Z., The neurocognitive correlates of brain entropy estimated by resting state fMRI. Neuroimage, 2021. 232: p. 117893.
Figures