1614
Fiber-specific white matter properties related to clinical features in military service members after a remote mild traumatic brain injury1National Intrepid Center of Excellence, Bethesda, MD, United States
Synopsis
Keywords: Traumatic Brain Injury, Traumatic brain injury, repetitive brain injury, fixel-based analysis, post-concussion syndrome, post-traumatic stress disorder
Motivation: Identifying brain changes that are associated with repetitive insult and persistent post-concussive symptoms can be potentially useful in differentiating mild traumatic brain injury from purely psychological disorders.
Goal(s): Apply fixel-based analysis (FBA) method to assess the relationships between clinical symptoms and tissue features using advanced dMRI techniques, and to identify WM changes that are associated with repetitive insult in service members (SMs).
Approach: Employ FBA, tractography and TSA on NODDI in SMs with mTBI.
Results: Unique anatomical locations where structural properties related to clinical symptoms. The white matter changes over the brainstem fibers are associated with the number of total lifetime TBI.
Impact: Advanced diffusion MRI techniques using higher model should be considered as a choice of option in assessing subtle white matter alterations in mild traumatic brain injury presenting due to the great heterogeneity of underlying pathological features.
Introduction
Mild traumatic brain injury (mTBI) presents with a wide array of clinical features due to the great heterogeneity of underlying pathological features. Injuries to service members (SMs) with mTBI are further complicated by post-traumatic stress disorder (PTSD) and other psychological disorders, e.g. depression. It is widely held that successive brain injuries lead to a cumulative effect greater than would be expected due to entirely independent injuries. Studies have demonstrated this effect in terms of both post-concussive syndrome and cognitive outcomes.1,2 Therefore, identifying brain changes that are associated with repetitive insult and persistent post-concussive symptoms can be potentially useful in differentiating mTBI from purely psychological disorders.The goal of this study is to apply fixel-based analysis (FBA)3 method and tract-specific analysis (TSA) to assess the relationships between clinical symptoms and tissue features using advanced diffusion magnetic resonance imaging (dMRI) techniques, and to identify WM changes that are associated with repetitive insult in service members (SMs).Methods
Two hundred and eleven (211) male SMs (age: 40.18 ± 5.88 years old), who had finished self-report Neurobehavioral Symptom Inventory (NSI) and the PTSD Checklist-Civilian version (PCLC), were selected from a larger sample of TBI cohort at the National Intrepid Center of Excellence, WRNMMC. Injuries were characterized via a structured interview addressing potential concussive events during military deployments and across the entire lifetime using a modification of the Ohio State University TBI Identification instrument.4 Simultaneous multi-slice (SMS, factor=3) multi-shell dMRI was acquired using a 3T scanner equipped with a 32-channel head coil with three shells (b=1000, 2000, 3000, 1.7 mm3). dMRI was preprocessed using the TORTOISE package. The NODDI-Watson model5 was fit to reconstruct maps of neurite density index (NDI), the intracellular volume fraction which primarily represents axonal density within WM; the volume fraction of the isotropic diffusion compartment (FISO) representing the free water content within the tissue; and orientation dispersion index (ODI) of neurites. To perform FBA, fiber orientation distributions (FOD) were estimated using the multi-shell multi-tissue constrained spherical deconvolution, and a study specific, unbiased FOD template was generated from a subset of participants using linear and non-linear registration of the FOD images followed by registering all FOD images to this template. Validity-10 scale was applied to assess symptom validity at ≥ 19 for possible symptom exaggeration6. We employed generalized additive modeling (GAM)7 to more flexibly model age-related variance given the wide age range of participants8 by modeling age as a covariate while evaluating the association between clinical features and neuroimaging metric. Significance was tested with 0.05 false discovery rate for correcting multiple comparisons. Finally, the WM features of the reconstructed tracts on the paths of those fixels were further evaluated by correlating the WM changes and the number of lifetime TBIs and concussive events using partial correlation after taking age into account.Results
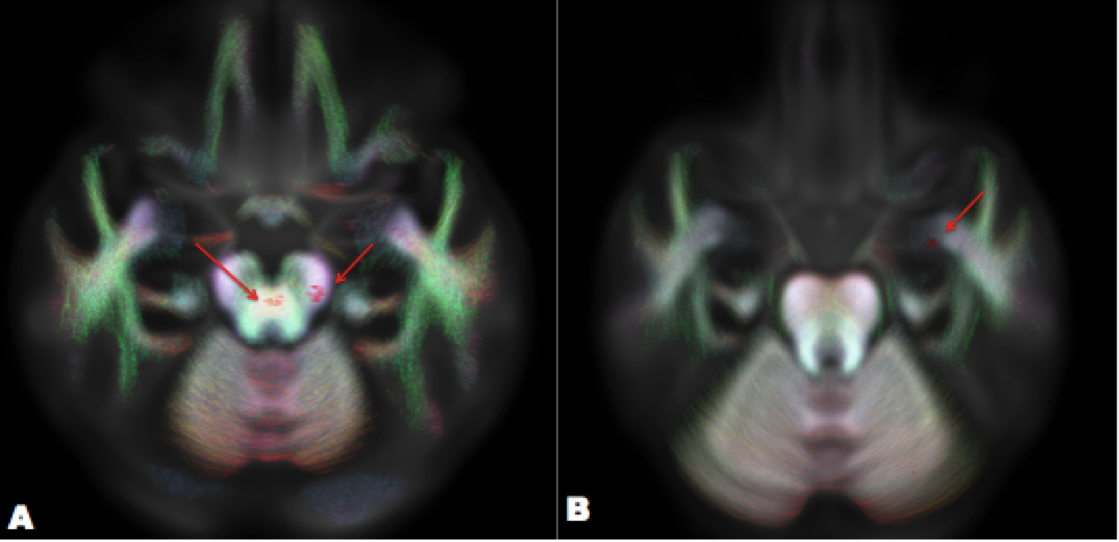
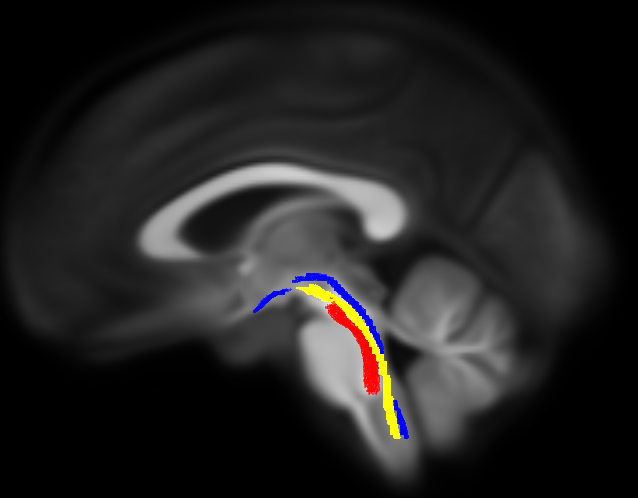
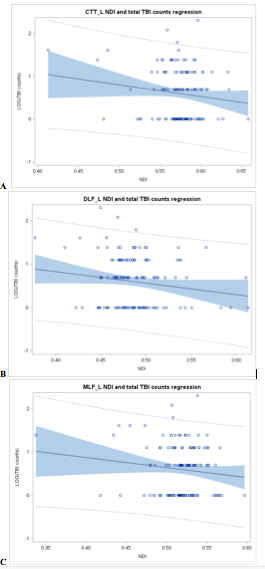
NSI score was associated with NODDI metrics, e.g. NDI and ODI, over the brainstem and the cerebral peduncles (Fig. 1A); and the PCLC score was correlated with NODDI metrics over the amygdala (Fig. 1B) and the fronto-parietal WM. Moreover, the mapped dMRI metrics of the fixels over the brainstem were found to be associated with the NSI score but not with the PCLC store (Fig. 1). The candidate fibers on the paths of the brainstem fixels were reconstructed using probabilistic tractography and identified as the medial longitudinal fasciculus, the dorsal longitudinal fasciculus and the central tegmental tracts (Fig. 2). After removing mTBI subjects who may exaggerate symptoms and had no concussion event, correlational analysis showed that logarithm of the lifetime TBI count was inversely correlated with NDI of the left central tegmental tract, the left dorsal longitudinal fasciculus and the left medial longitudinal fasciculus (r=-0.42, p=0.007; r = -0.41, p=0.009;r=-0.40, p=0.01 respectively) (Fig. 3).Discussion / Conclusions
Our results suggest combining FBA, tractography and TSA is helpful in identifying WM changes that is associated with clinical features after a remote brain injury in SMs. The findings of correlation between lifetime TBI event and microstructural changes of brainstem fibers suggest high shear force develop at the brainstem after repetitive insult, which is supported by literature9. In addition, the association of PTSD-like symptom and WM changes over the amygdala is compatible with the hypothesis of disrupted fronto-limbic circuitry.The anatomical locations between the clinical presentations and the fiber specific structural changes are unique and specific. Most importantly, the findings of this study can be used neuroimaging markers to differentiate pure psychological disorders, e.g. PTSD from mTBI, and have the potential clinical application for monitoring the recovery of mTBI in SMs.Acknowledgements
Disclaimer: The views expressed in this abstract are those of the authors and do not necessarily reflect the official policy of the Department of Defense or the U.S. Government.References
1. Teasdale TW. Cognitive dysfunction in young men following head injury in childhood and adolescence: a population study. J Neurol Neurosurg Psychiatry. 2003;74(7):933-936. doi:10.1136/jnnp.74.7.933
2. PONSFORD J, WILLMOTT C, ROTHWELL A, et al. Factors influencing outcome following mild traumatic brain injury in adults. J Int Neuropsychol Soc. 2000;6(5):568-579. doi:10.1017/S1355617700655066
3. Dhollander T, Clemente A, Singh M, et al. Fixel-based Analysis of Diffusion MRI: Methods, Applications, Challenges and Opportunities. Neuroimage. 2021;241:118417. doi:10.1016/j.neuroimage.2021.118417
4. Walker WC, Carne W, Franke LM, et al. The Chronic Effects of Neurotrauma Consortium (CENC) multi-centre observational study: Description of study and characteristics of early participants. Brain Inj. 2016;30(12):1469-1480. doi:10.1080/02699052.2016.1219061
5. Zhang H, Schneider T, Wheeler-Kingshott CA, Alexander DC. NODDI: Practical in vivo neurite orientation dispersion and density imaging of the human brain. Neuroimage. Published online 2012. doi:10.1016/j.neuroimage.2012.03.072
6. Lange RT, Brickell TA, Lippa SM, French LM. Clinical utility of the Neurobehavioral Symptom Inventory validity scales to screen for symptom exaggeration following traumatic brain injury. J Clin Exp Neuropsychol. 2015;37(8):853-862. doi:10.1080/13803395.2015.1064864
7. Hastie T, Tibshirani R. Generalized Additive Models. Stat Sci. 1986;1(3):297-310.
8. Zhao C, Tapera TM, Bagautdinova J, et al. ModelArray: An R package for statistical analysis of fixel-wise data. Neuroimage. 2023;271:120037. doi:10.1016/j.neuroimage.2023.120037
9. Mac Donald CL, Johnson AM, Cooper D, et al. Detection of blast-related traumatic brain injury in U.S. military personnel. N Engl J Med. 2011;364(22):2091-2100. doi:10.1056/NEJMoa1008069
Figures