1612
Detection of neuroinflammation and ischemia in traumatic brain injury in rats using amide proton transfer MRI1Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Department of Biomedical Engineering, Johns Hopkins University, Baltimore, MD, United States, 3Department of Computer Science, Johns Hopkins University, Baltimore, MD, United States, 4Department of Mechanical Engineering, Johns Hopkins University, Baltimore, MD, United States, 5Department of Electrical and Computer Engineering, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Keywords: Traumatic Brain Injury, Traumatic brain injury, neuroinflammation, ischemia
Motivation: Ischemia and neuroinflammation, two key endophenotypes post-TBI, are difficult to assess in vivo.
Goal(s): Our goal was to evaluate the feasibility of utilizing amide proton transfer-weighted (APTw) imaging as a biomarker for detecting neuroinflammation and ischemia post-TBI.
Approach: Brain APTw MRI signals of 55 rats subjected to a mild, moderate, or severe TBI were analyzed and compared to other criteria defining neuroinflammation and ischemia.
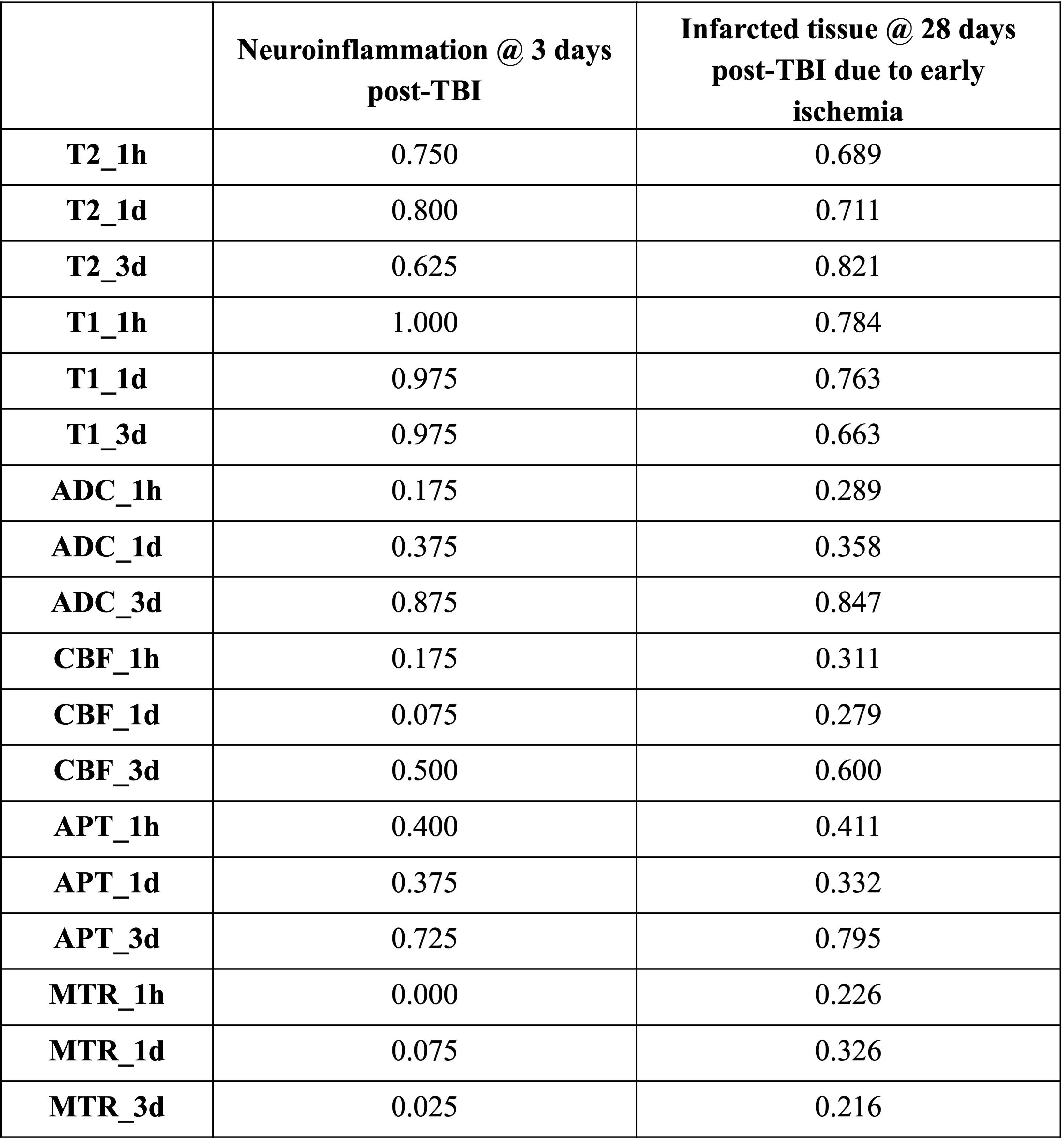
Results: The areas under curve (AUCs) of the ipsilateral cortex APTw signals at 3 days and 1 hour post-TBI were 0.725 for detecting neuroinflammation and 0.411 for detecting ischemia, respectively.
Impact: The feasibility of detecting neuroinflammation and ischemia using APTw MRI would improve the capability of MRI to objectively assess TBI and enable the accurate detection of these pathological processes at an early stage post-TBI.
Introduction
Traumatic brain injury (TBI) is a leading cause of disability and death. More than 200 thousand TBI-related hospitalizations were recorded in 2020 and more than 69 thousand TBI-related deaths in 2021.1 Neuroinflammation and ischemia are two key secondary injury events in TBI.2,3 Previous studies have shown that amide proton transfer-weighted (APTw) MRI, a molecular MRI technique generating image contrast based on the amide protons in mobile cellular proteins and peptides in tissue4, has the potential to detect neuroinflammation and ischemia.5,6 However, the extent to which APTw signal changes can correlate with neuroinflammation and ischemia post-TBI is not clear yet. In this study, we used Spearman's rank correlation coefficient and receiver operating characteristic (ROC) analysis to investigate this question. The goal is to evaluate the feasibility of utilizing amide protein transfer weighted (APTw) as an early biomarker for neuroinflammation and ischemia post-TBI.Methods
Traumatic brain injury modelControlled cortical impact (CCI) was introduced to rats (Sprague-Dawley, n=55), where the bone flap was removed and the dura was impacted with a benchmark stereotaxic impactor (IM10244; Leica Biosystems, Inc., Richmond, VA) with a diameter of 3 mm at a velocity of 5.5 m/s and a dwell time of 100 ms. Rats were categorized into four groups: sham (n=7), mild (impact depth=1mm, n=16), moderate (3mm, n=16), severe (5mm, n=16).
Magnetic resonance imaging data acquisition and analysis
MRI data including T2 mapping, T1 mapping, isotropic ADC, CBF, APTw, and MTR were acquired at 1 hour, 1 day, 3 days, 7 days, 14 days and 28 days post-TBI on a 4.7-Tesla horizontal bore animal imager (Bruker Biospin, Billerica, MA). Data were processed with Matlab (version: R2022b). Regions of interest (ROIs) included core lesion, ipsilateral cortex, contralateral cortex, ipsilateral hippocampus, and contralateral hippocampus. They were drawn manually on MTR maps, using T2w as a reference, and then transferred to the same sites on all other MRI images. The average signal intensities were extracted from each ROI.
Criteria for defining neuroinflammation and ischemia
Neuroinflammation was evaluated using histopathology assessment of glial fibrillary acidic protein (GFAP) and ionized calcium binding adaptor molecule 1 (iba1), which are indicators for astrocytes and microglia respectively, at 3 days and 28 days post-TBI. The number of rats with successful staining in each group was as follows: sham group (n = 4), mild TBI group (n = 3), moderate TBI group (n = 6), and severe TBI group (n = 6). Existence of ischemia was defined as the T2 signal intensity increase of over 50% compared to the average.
Statistical analysis
Receiver operating characteristic (ROC) analysis was used to evaluate the performance of APTw signals to identify neuroinflammation and ischemia in ipsilateral cortex. The area under the curve (AUC), sensitivity, and specificity were recorded. These analyses were performed with SPSS software (version 29.0.1.0; SPSS, Inc., Chicago, IL). P < 0.05 was considered statistically significant.
Results and discussion
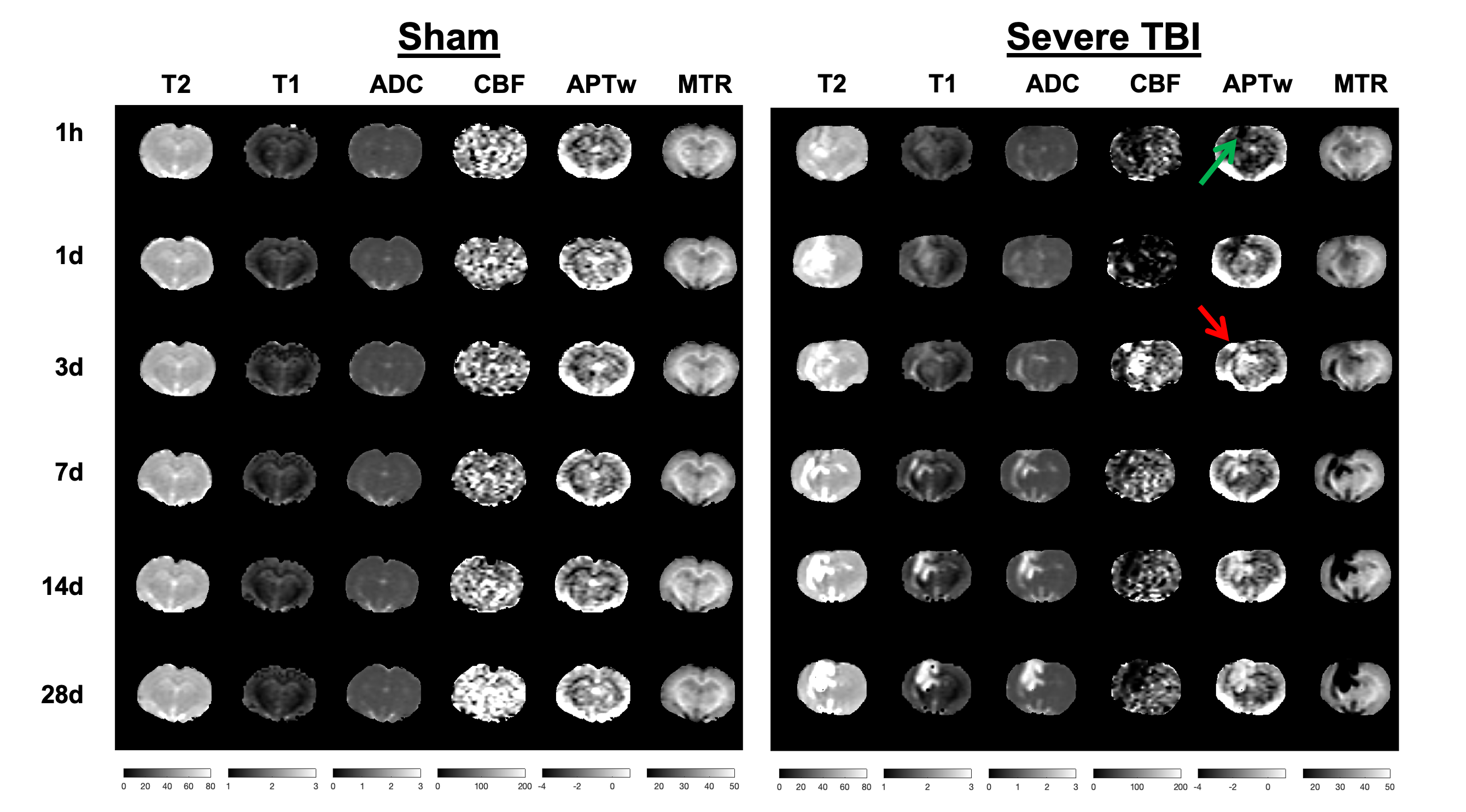
Fig. 1 compares multi-parametric MR images for one sham-group rat and one severe-group rat at multiple time points after TBI. APTw MRI signals at 1 hour post-TBI decreased around the injured area due to ischemia in the moderate and severe groups (indicated by the green arrow). Notably, APTw imaging revealed an acidosis-based ischemic penumbra around the impacted area at a few hours post-injury, which was not evident on several other MRI sequences. Hyperintense APTw MRI signal at 3 days post-TBI (indicated by the red arrow) was observed due to neuroinflammation.Based on the ROC analysis (Table 1), the AUCs of APTw signals at 3 days post-TBI was 0.725 for detecting day-3 neuroinflammation (sensitivity: 0.63, specificity: 0.80), indicating the potential of using APTw hyperintensity as a neuroinflammation biomarker at 3 days post-TBI. The signal at 1 hour post-TBI was 0.411 for detecting ischemia (sensitivity: 0.98, specificity: 0.16). Additionally, APTw signals at 3 days post-TBI may be a good indicator of infarction caused by ischemia, as shown by the relatively high AUC score of 0.795. It should be noted that the current criteria for defining ischemia can be improved and other criteria can be explored for the future analysis.
Conclusion
The findings in this preliminary study illustrate the potential of using APTw imaging as a biomarker to detect neuroinflammation and ischemia post-TBI. Such a biomarker will likely be used in future research to evaluate treatment efficacy, given its enhanced sensitivity to pathophysiological alterations in the brain.Acknowledgements
No acknowledgement found.References
- Centers for Disease Control and Prevention. National Center for Health Statistics: Mortality Data on CDC WONDER. Accessed April 2023, https://wonder.cdc.gov/mcd.html.
- Kumar, A., & Loane, D. J. (2012). Neuroinflammation after traumatic brain injury: opportunities for therapeutic intervention. Brain, behavior, and immunity, 26(8), 1191-1201.
- Greve, M. W., & Zink, B. J. (2009). Pathophysiology of traumatic brain injury. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine: A Journal of Translational and Personalized Medicine, 76(2), 97-104.
- Zhou, J., Heo, H. Y., Knutsson, L., van Zijl, P. C., & Jiang, S. (2019). APT‐weighted MRI: techniques, current neuro applications, and challenging issues. Journal of Magnetic Resonance Imaging, 50(2), 347-364.
- Sun, P.Z., Zhou, J., Sun, W., Huang, J. & van Zijl, P.C.M. (2007). Detection of the ischemic penumbra using pH-weighted MRI. J Cereb Blood Flow Metab. 27, 1129-36.
- Zhang, H., Wang, W., Jiang, S., Zhang, Y., Heo, H. Y., Wang, X., Peng, Y., Wang, J. & Zhou, J. (2017). Amide proton transfer-weighted MRI detection of traumatic brain injury in rats. Journal of Cerebral Blood Flow & Metabolism, 37(10), 3422-3432.
Figures