1610
Multicenter Harmonization of Longitudinal DTI and NODDI of White Matter Microstructure after Acute TBI: A TRACK-TBI* Study1Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 2Department of Neurosurgery, University of California San Francisco, San Francisco, CA, United States, 3University of Washington, Seattle, WA, United States, 4Spaulding Rehabilitation Hospital, Harvard Medical School, Boston, MA, United States, 5Medical College of Wisconsin, Milwaukee, WI, United States, 6Baylor College of Medicine, Houston, TX, United States, 7University of California San Diego, San Diego, CA, United States, 8University of Pennsylvania, Philadelphia, PA, United States, 9University of Pittsburgh Medical Center, Pittsburgh, PA, United States
Synopsis
Keywords: Traumatic Brain Injury, Neurodegeneration, TBI, White matter, DTI, NODDI
Motivation: Diffusion MRI-derived NODDI demonstrated promise as biomarkers of post-TBI long-term symptoms and clinical outcomes in single-center studies, but hasn't been validated in large-scale multi-center trials.
Goal(s): This study aimed to detect post-TBI white matter degeneration and its significance to outcomes using analysis methods incorporating RISH-based harmonization, followed by DTI and NODDI fitting.
Approach: Harmonized DTI and NODDI are analyzed for a longitudinal comparison between 2 weeks and 6 months post-TBI, and for associations with GOSE, RPQ, and WAIS-PSI outcomes.
Results: Widespread white matter degeneration was evident in longitudinal changes of DTI and NODDI. The 2-week metrics were predictive of 3 and 6-month outcomes.
Impact: This study applies RISH-based harmonization to a multi-shell, multi-center dMRI study that involved 7 scanners of different manufacturers and models with different software versions and pulse-sequence parameters. These efforts brought new insights into post-traumatic white matter injury and patient outcomes.
Background
Traumatic brain injury (TBI) triggers prolonged and intermingled recovery and degeneration that is variable across individuals1-3. Diffusion MRI (dMRI) tensor imaging (DTI) and biophysical compartment models (e.g., neurite orientation dispersion and density imaging: NODDI) of white matter (WM) microstructure are promising biomarkers of patient outcomes in single-center TBI studies4,5, but advanced multishell dMRI techniques such as NODDI have yet to be validated in large-scale multicenter trials. A major challenge is that NODDI metrics of neurite density index (NDI), orientation dispersion index (ODI) and free water fraction (FISO) are known to have low reproducibility across different scanners5-7. In this work, we demonstrate DTI and NODDI harmonization in a multicenter longitudinal acute TBI study using a unified dMRI acquisition protocol and standardized processing pipeline incorporating a state-of-the-art multishell dMRI harmonization algorithm8-11 to detect white matter microstructural injury and its significance to long-term patient outcomes.Methods
Acute TBI patients ages 18-70 years were enrolled at 7 of the 18 TRACK-TBI Level-1 trauma centers participating in the Phase 2 MRI study, 95% with Glasgow Coma Scale 13-15 signifying mild TBI. 3T dMRI was acquired 2 weeks (n=333) and 6 months (n=258) post-injury with b=1000 and 3000 s·mm-2 using 64 directions per shell and 2.4-mm voxels. The study enrolled 49 demographically matched controls across the 7 centers. Images were preprocessed with FSL eddy12 for topup distortion correction, slice-to-volume motion correction, and outlier rejection. MP-PCA denoising13 was performed. Inter-scanner harmonization employed rotation-invariant spherical harmonics (RISH)8-11 trained on the control subjects to generate the inter-scanner transformations used for the TBI patients. DTIfit of b1000 data yielded fractional anisotropy (FA), axial diffusivity (AD), mean diffusivity (MD), and radial diffusivity (RD). Accelerated microstructure imaging via convex optimization (AMICO) analysis from b1000 and b3000 shells generated NDI, ODI, and FISO14. FA maps were registered to the FMRIB58 template in MNI152 space and anchored group registration and skeletonization for all parameters using TBSS15. Skeletonised DTI and NODDI maps were analyzed voxelwise with randomise and tractwise with the Johns Hopkins University (JHU) WM Atlas, using voxelwise threshold-free cluster enhancement and tractwise false discovery rate (FDR) correction for multiple comparisons correction. Two-week DTI and NODDI metrics were investigated as predictors of 3-month and 6-month Glasgow Outcome Scale Extended (GOSE) disability, Rivermead Postconcussion Questionnaire (RPQ) symptoms and Wechsler Adult Intelligence Scale Processing Speed Index (WAIS-PSI) in multivariable models adjusting for age, sex, race/ethnicity, years of education, psychiatric history, and prior TBI.Results
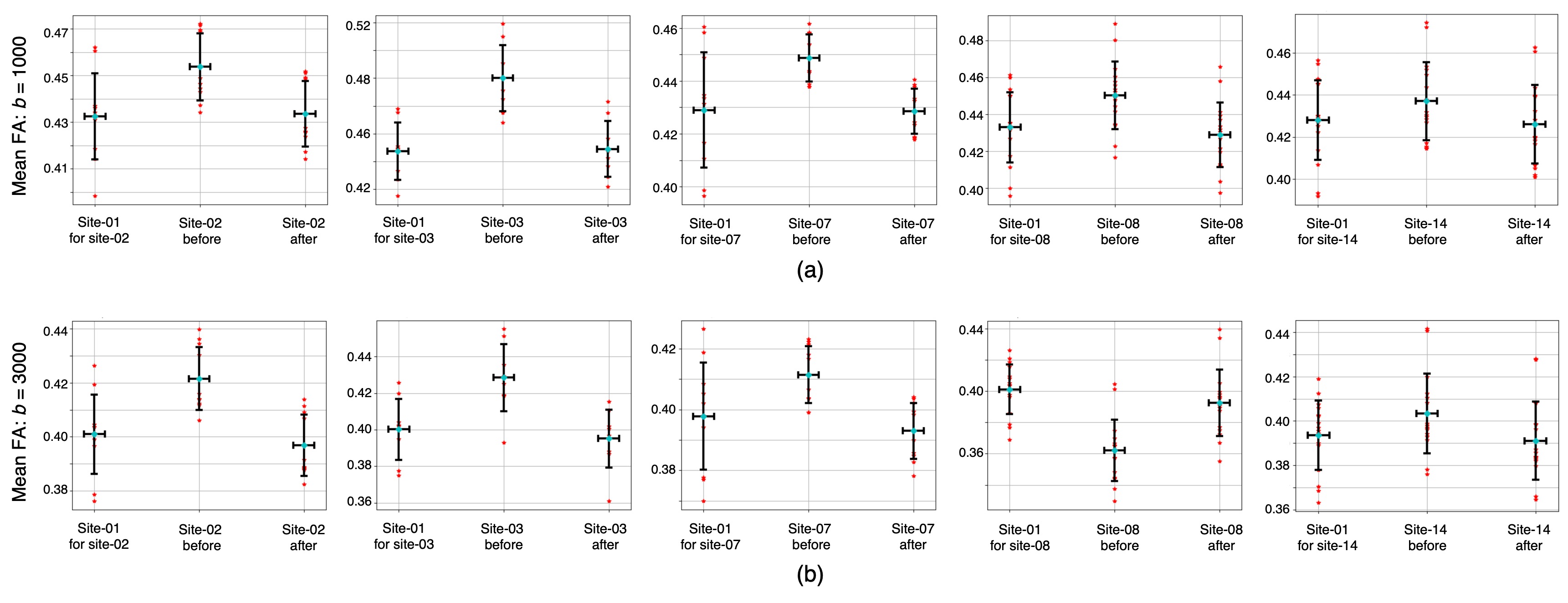
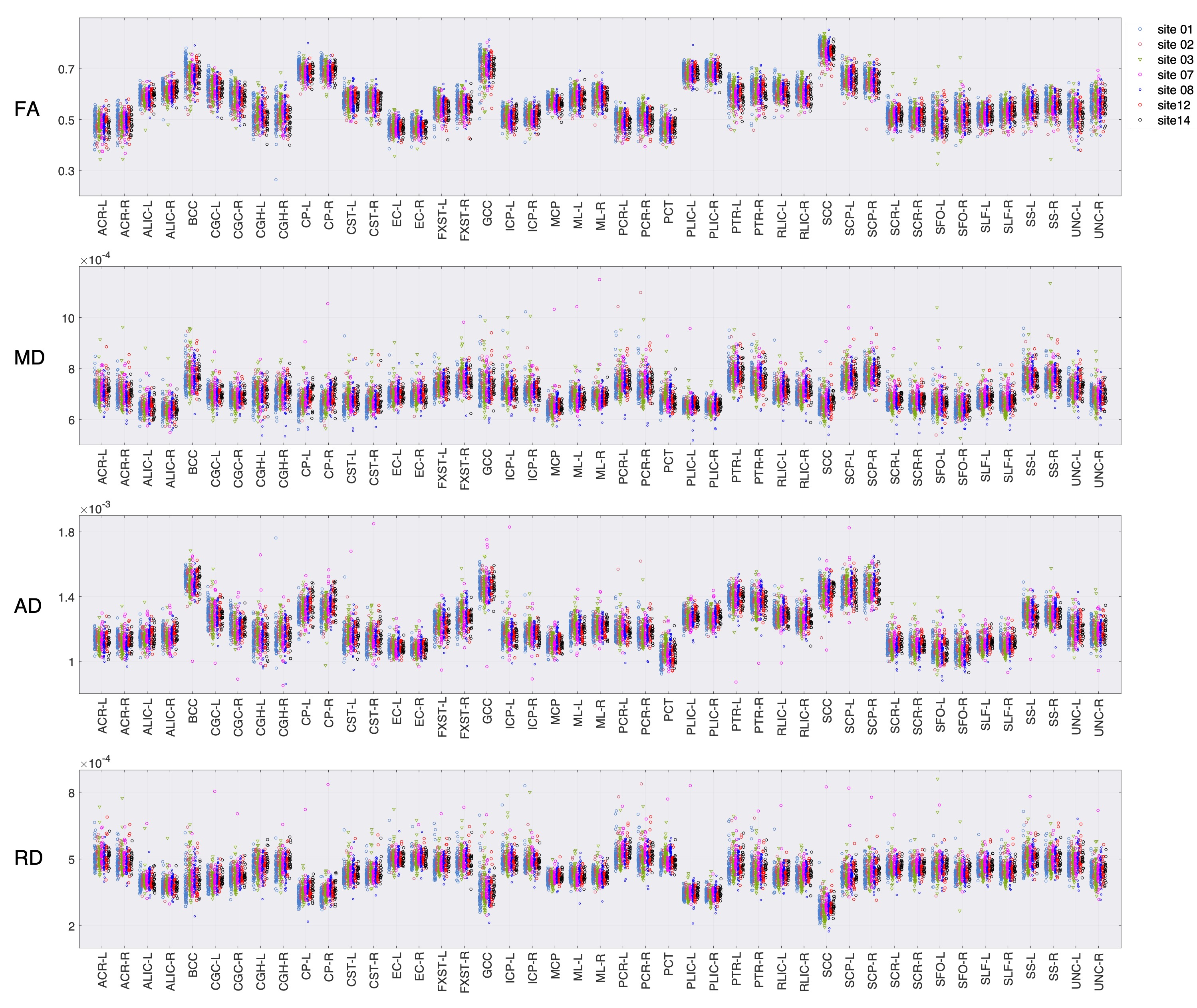
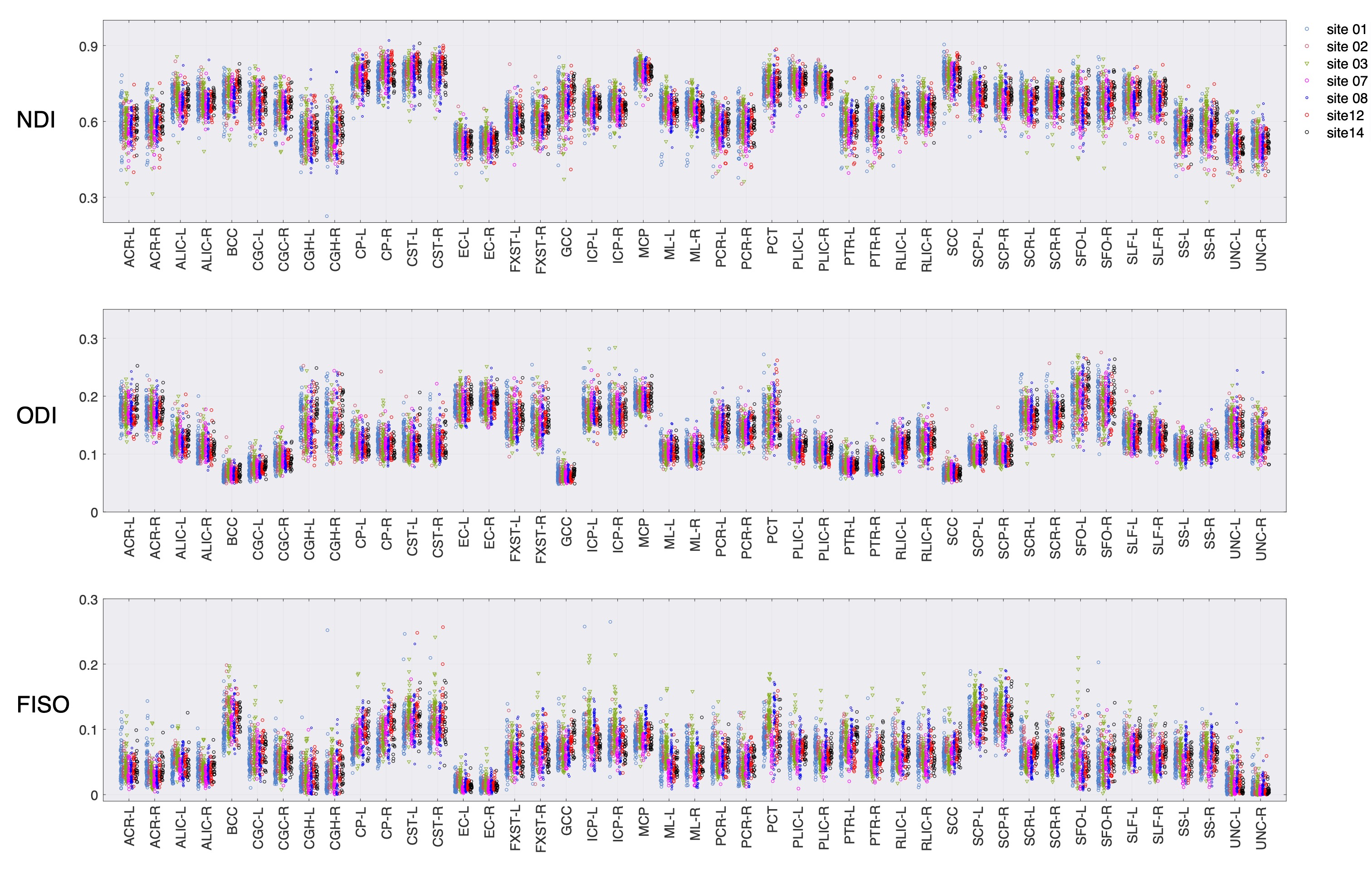
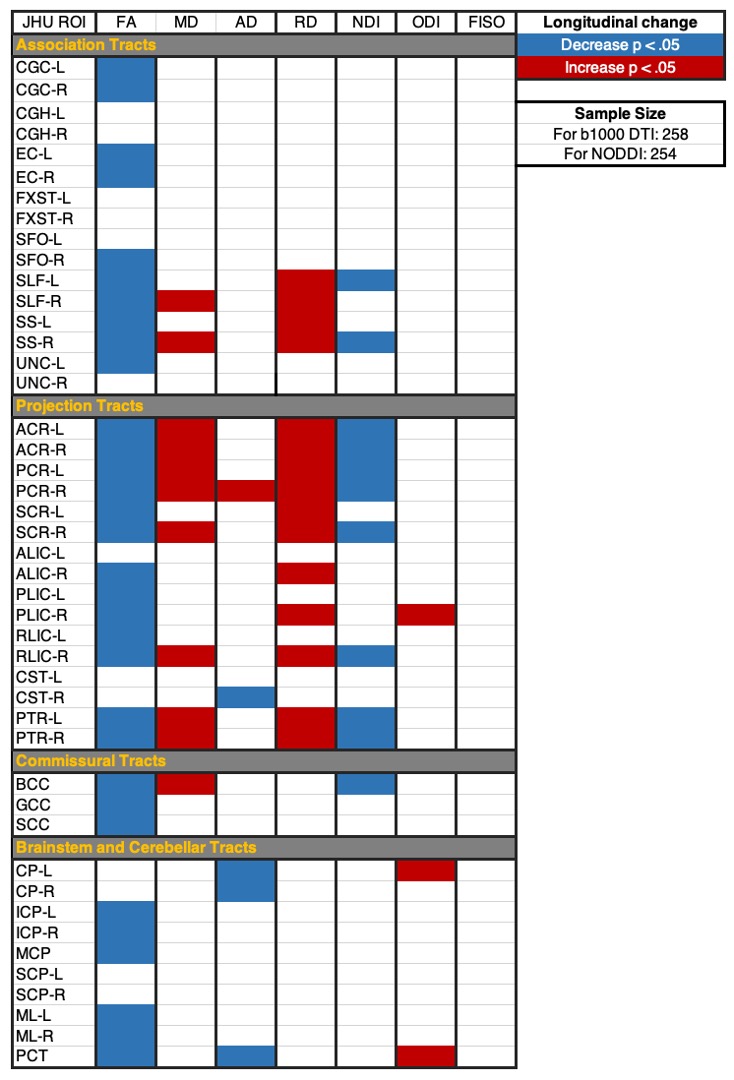
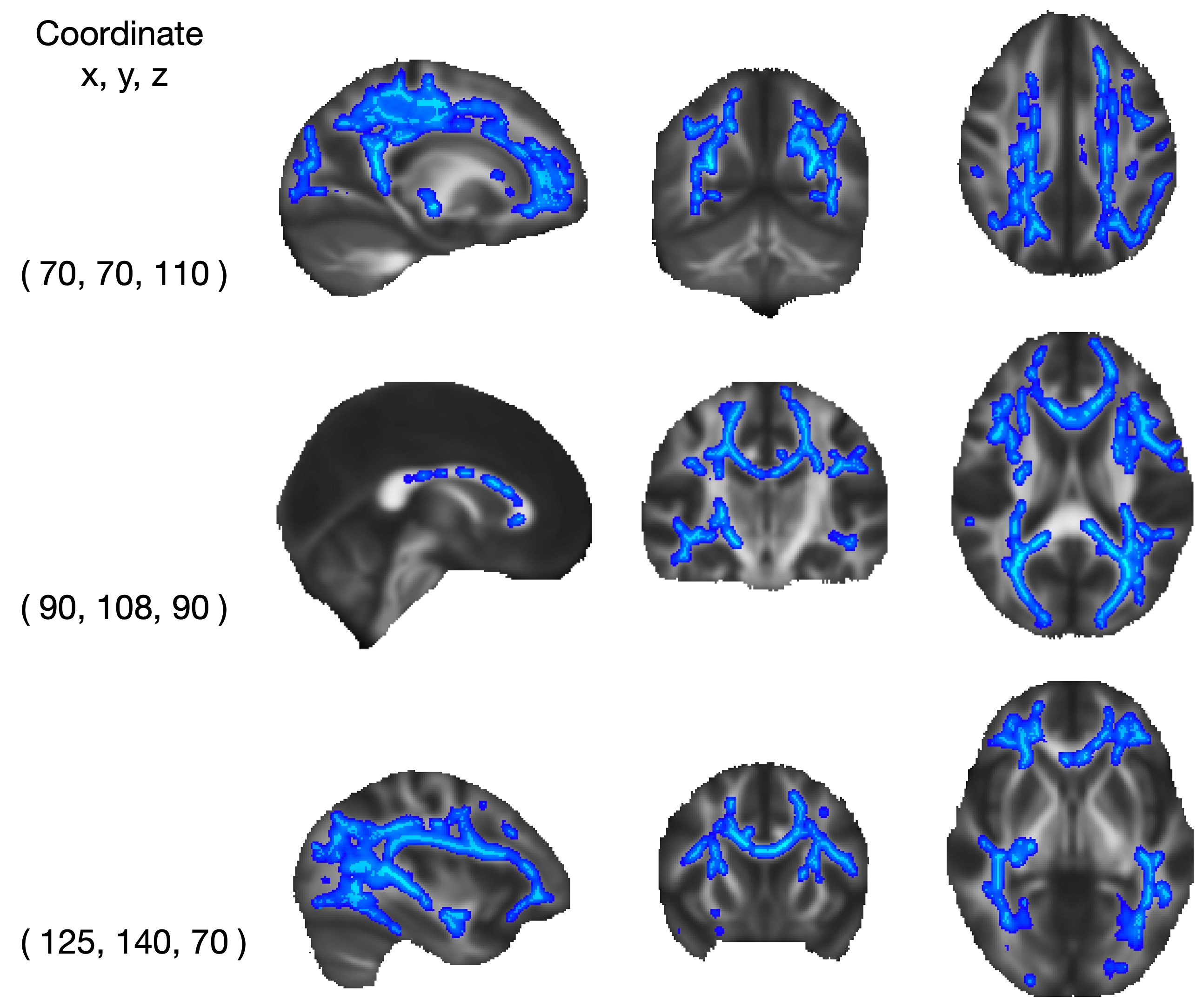
RISH harmonization mitigated inter-site variability of DTI and NODDI in controls and patients (Figs. 1-3). DTI and NODDI both revealed extensive WM changes from 2 weeks to 6 months post-injury (Figs. 4-5). Applying JHU tract abbreviations, corona radiata and PTR showed decreasing FA and NDI with increasing MD and RD. The internal capsules showed decreasing FA and increasing RD. FA was decreasing in most association tracts and the entire corpus callosum, some with decreasing NDI and increasing MD and RD. Most brainstem/cerebellar tracts showed decreasing FA, a few with decreasing AD and increasing ODI. Widespread changes in NDI, but not ODI or FISO, were also found in TBSS voxelwise analysis (Fig. 5).Adjusting for clinical/demographic covariates, 2-week DTI and NODDI of corpus callosum, brainstem and cerebellum were predictive of 3-month and, to a lesser extent, 6-month GOSE, with the strongest association at 6-months for SCP NDI with odds ratio (OR) of 1.48 (1.07-2.08, p=0.02). Two-week WM AD and FISO were predictive of 3-month and 6-month RPQ, especially in corpus callosum and brainstem/cerebellar tracts, with the strongest association at 6-months for the SCP with AD fold change (FC) of 1.19 (1.01-1.40, p=0.03) and FISO FC of 1.19 (1.06-1.35, p=0.004). Two-week global WM ODI was predictive of 6-month WAIS-PSI at b=-2.77 (-0.41 to -5.11, p=0.02), with the strongest tract associations in SCP at b=-2.45 (-0.31 to -4.46, p=0.04) and ICP at b=-2.20 (-0.10 to -4.30, p=0.04). Two-week AD was also predictive of 6-month WAIS-PSI in BCC at b=2.42 (0.40 to 4.45, p=0.02).
Conclusions
After RISH harmonization of multicenter longitudinal multishell dMRI data, widespread DTI and NODDI changes of white matter microstructure were observed over time in these largely mild TBI patients across cerebral association, projection, and commissural tracts as well as in brainstem and cerebellum. Two-week DTI and NODDI WM metrics were predictive of long-term disability, symptomatic and cognitive outcomes, especially in corpus callosum and brainstem/cerebellum, independent of clinical and demographic factors. This paves the way towards larger-scale multicenter longitudinal trials of advanced multishell dMRI for TBI diagnosis, prognosis, and treatment monitoring as well as for other neurological and psychiatric disorders.Acknowledgements
The TRACK-TBI study is sponsored by the U.S. National Institutes of Health, National Institute of Neurologic Disorders and Stroke (Grant U01 NS086090), and the US Department of Defense (W81XWH-14-2-0176, W81XWH-18-2-0042).
* TRACK-TBI: Transforming Research and Clinical Knowledge in Traumatic Brain Injury
The TRACK-TBI Investigators: Shankar Gopinath, MD, Baylor College of Medicine; Ramesh Grandhi, MD MS, University of Utah; C. Dirk Keene, MD PhD, University of Washington; Randall Merchant, PhD, Virginia Commonwealth University; Laura B. Ngwenya, MD, PhD, University of Cincinnati; Ava Puccio, PhD, University of Pittsburgh; David Schnyer, PhD, UT Austin; Sabrina R. Taylor, PhD, University of California, San Francisco; John K. Yue, MD, University of California, San Francisco; Ross Zafonte, DO, Harvard Medical School
References
1. Kuceyeski, A. F., Jamison, K. W., Owen, J. P., Raj, A., & Mukherjee, P. (2019). Longitudinal increases in structural connectome segregation and functional connectome integration are associated with better recovery after mild TBI. Human brain mapping, 40(15), 4441-4456.
2. Maas, A. I., Menon, D. K., Manley, G. T., Abrams, M., Åkerlund, C., Andelic, N., ... & Zemek, R. (2022). Traumatic brain injury: progress and challenges in prevention, clinical care, and research. The Lancet Neurology, 21(11), 1004-1060.
3. Nelson, L. D., Temkin, N. R., Dikmen, S., Barber, J., Giacino, J. T., Yuh, E., ... & TRACK-TBI Investigators. (2019). Recovery after mild traumatic brain injury in patients presenting to US level I trauma centers: a transforming research and clinical knowledge in traumatic brain injury (TRACK-TBI) study. JAMA neurology, 76(9), 1049-1059.
4. Yuh, E. L., Cooper, S. R., Mukherjee, P., Yue, J. K., Lingsma, H. F., Gordon, W. A., ... & Sinha, T. K. (2014). Diffusion tensor imaging for outcome prediction in mild traumatic brain injury: a TRACK-TBI study. Journal of neurotrauma, 31(17), 1457-1477.
5. Palacios, E. M., Owen, J. P., Yuh, E. L., Wang, M. B., Vassar, M. J., Ferguson, A. R., ... & TRACK-TBI Investigators. (2020). The evolution of white matter microstructural changes after mild traumatic brain injury: a longitudinal DTI and NODDI study. Science Advances, 6(32), eaaz6892.
6. Andica, C., Kamagata, K., Hayashi, T., Hagiwara, A., Uchida, W., Saito, Y., … & Aoki, S. (2020). Scan–rescan and inter-vendor reproducibility of neurite orientation dispersion and density imaging metrics. Neuroradiology, 62(4), 483-494.
7. Kamiya, K., Hori, M., & Aoki, S. (2020). NODDI in clinical research. Journal of Neuroscience Methods, 345, 108908.
8. Mirzaalian, H., Ning, L., Savadjiev, P., Pasternak, O., Bouix, S., Michailovich, O., … & Rathi, Y. (2018). Multi-site harmonization of diffusion MRI data in a registration framework. Brain Imaging and Behavior, 12(1), 284-295.
9. Cetin Karayumak, S., Bouix, S., Ning, L., James, A., Crow, T., Shenton, M., Kubicki, M., & Rathi, Y. (2019). Retrospective harmonization of multi-site diffusion MRI data acquired with different acquisition parameters. Neuroimage, 184, 180-200.
10. Billah T, Cetin Karayumak S, Bouix S, Rathi Y. (2019). Multi-site Diffusion MRI Harmonization. https://github.com/pnlbwh/dMRIharmoniziation, doi: 10.5281/zenodo.2584275.
11. Ning, L., Bonet-Carne, E., Grussu, F., Sepehrband, F., Kaden, E., Veraart, J., … & Tax, C. (2021). Cross-scanner and cross-protocol multi-shell diffusion MRI data harmonization: Evaluation of algorithms. Neuroimage, 221, 117128.
12. Andersson, J.L., & Sotiropoulos, S.N. (2016). An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage, 125(1), 1063–1078.
13. Veraart, J., Novikov, D.S., Christiaens, D., Ades-aron, B., Sijbers, J., & Fieremans, E. (2016). Denoising of diffusion MRI using random matrix theory. Neuroimage, 142(11), 394.
14. Daducci, A., Canales-Rodríguez, E. J., Zhang, H., Dyrby, T. B., Alexander, D. C., & Thiran, J. P. (2015). Accelerated microstructure imaging via convex optimization (AMICO) from diffusion MRI data. Neuroimage, 105, 32-44.
15. Smith, S.M., Jenkinson, M., Johansen-Berg, H., Rueckert, D., Nichols, T.E., Mackay, C.E., Watkins, K.E., Ciccarelli, O., Cader, M.Z., Matthews, P.M., & Behrens, T.E. (2006). Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage, 31(4), 1487–1505.
Figures