1558
Localization of Back Pain by Assessment of Sigma-1 Receptor Expression using PET/MR imaging1Radiology, University of Wisconsin-Madison, Madison, WI, United States, 2Neurosurgery, Stanford University School of Medicine, Stanford, CA, United States, 3Neurosurgery Artificial Intelligence Lab, Stanford University School of Medicine, Stanford, CA, United States
Synopsis
Keywords: Other Musculoskeletal, PET/MR, back pain, molecular imaging
Motivation: Diagnosis of chronic low back pain remains a challenge with conventional diagnostic methods leading to unsatisfactory treatment in a vast majority of patients.
Goal(s): To investigate the use of sigma-1 receptor (S1R) radioligand, [18F] FTC-146 in conjunction with positron emission tomography/magnetic resonance imaging (PET/MRI) for identifying the pain generator in chronic low back pain.
Approach: Correlation of [18F] FTC-146 PET-MRI imaging in patients with unresolved chronic low back pain to clinical findings.
Results: S1R PET/MRI imaging matched the clinical diagnosis in all cases. Additionally, it offered benefit over traditional MRI by identifying additional “functional” findings both within and outside the spine.
Impact: Future clinical implementation of S1R-PET/MR can potentially help reveal previously unidentified pain generator in patients with chronic low back pain that have exhausted standard clinical care leading to better-targeted treatment.
Introduction
Back pain is a highly prevalent source of morbidity and a significant medical and economic burden.1-4 Utilization of opioid-based analgesics for back pain has resulted in an unintentional and tragic contribution to the opioid epidemic.5-8 The main issue is our inability to correctly identify the pain generator with current imaging methods in a vast majority of patients leading to inadequate treatment.9,10 Local increases in the expression of sigma-1 receptors (S1R) have been observed at the site of pain generation, and, accordingly, S1R has been implicated as an imaging biomarker for nociceptive activity.11,12 Leveraging a novel radioligand molecule ([18F]FTC-146) that binds to S1R13,14 with extremely high specificity and positron emission tomography (PET) MR imaging, we aimed to develop a method for precise anatomic visualization and localization of pain-generating activity in patients with back pain.Methods
This prospective, single-center, observational study was approved by the IRB and all subjects signed a written informed consent. Specific patient selection for full body ([18F]FTC-146) PET/MRI scan was performed after clinical and radiological review. Patients with either axial back pain or radicular pain were included by the neurosurgeon specializing in spinal surgery and must have experienced at least 2 months of back pain and failed conventional treatments.A single 5 mCi dose of 18F-FTC-146 was injected to the subject 40 minutes before imaging in a PET/MRI scanner (GE SIGNA 3.0 Tesla MRI with a time-of flight PET scanner, GE Healthcare, Waukesha, U.S.). Depending on the subject’s height, 1 to 2 bed positions were utilized to scan the lumbar spine to the mid-thigh of the subject. 20-minute simultaneous acquisition of PET and MRI were conducted for each bed position. Multiplanar 2D FSE sequences with T1 and T2 weighting from our clinical lumbar spine MRI protocol, 3D axial LAVA-FLEX, and 3D coronal CUBE-FLEX will be employed for MRI acquisition. PET data was reconstructed using a fully 3-dimensional iterative ordered-subsets expectation maximization algorithm that corrected for attenuation, scatter, dead time and decay.
An experienced musculoskeletal radiologist with extensive expertise in reading PET images, reviewed MRI-only images and 18F-FTC-146 PET/MRI images from the patients and controls in a random order blinded to patient’ information. Imaging review for MRI was focused on finding abnormally increased signal intensity on T2 sequences while PET image review focused on increased [18F]FTC-146 uptake. SUVmax values were measured. The interval between MRI-only review and PET/MRI review for the same subject was 3 weeks to prevent memory bias. Using only the imaging findings, suspected painful lesions were identified and marked on the PET/MRI sequences. The PET/MRI identified lesion was compared with the subject’s clinical symptoms to determine whether it was an accurate localization. Both sets of images were then correlated with this reference standard.
Results
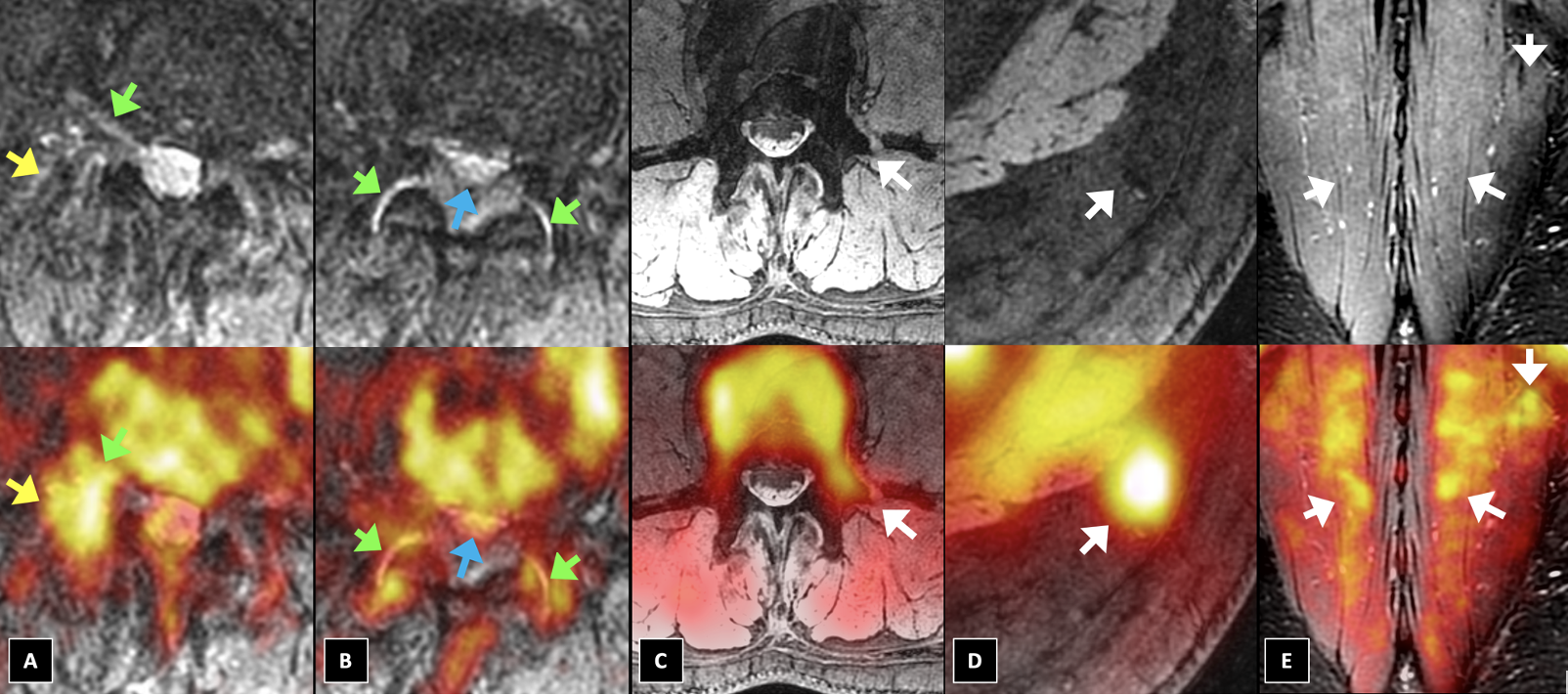
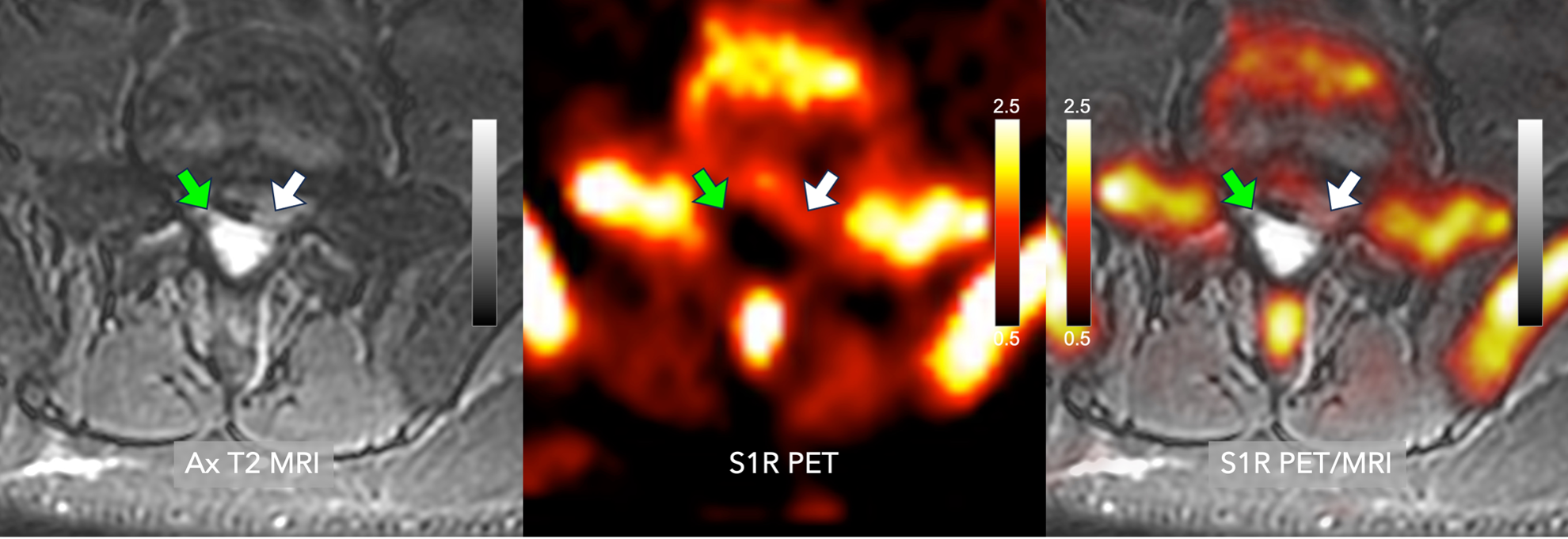
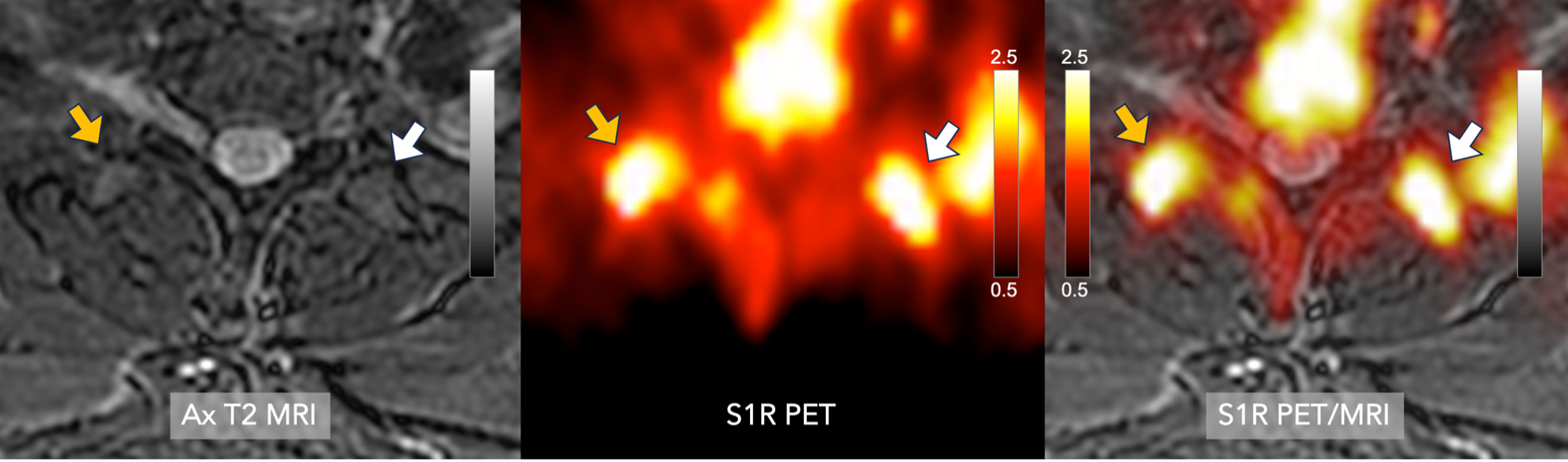
Eight patients with various etiologies of back pain were included. Abnormally elevated [18F]FTC-146 uptake was seen in several relevant spinal anatomic landmarks including spinal nerves (Figure 1A), facet joints (Figure 1A and 1B), the spinal canal (Figure 1B), transverse processes (Figure 1C), subcutaneous tissues (Figure 1D), and paraspinal muscles (Figure 1E). However, structural or signal abnormalities on MRI were observed only in some cases: nerve compression (Figure 1A), facet arthropathy (Figure 1A), stenosis (Figure 1B), and fracture (Figure 1C).S1R PET/MRI imaging matched the clinical diagnosis in all cases, including disc herniation, nerve compression, stenosis, and arthropathy (examples shown in figure 2 and 3). Additionally, it offered benefit over traditional MRI by identifying additional “functional” findings both within and outside the spine. This additional functional detail, was useful for patients with either no or multiple structural abnormalities on MRI to pinpoint the true cause of pain demonstrating the synergistic utility of this imaging modality. Such functional detail guided successful interventions including surgery, therapy, and injections in our patient cohort that successfully addressed the pain in all 8 patients.
Discussion
In this preliminary study, S1R PET/MR imaging appears to achieve enhanced diagnostic sensitivity to local nociceptive sources of LBP. More work will be needed to further validate the correlation between pain generators and imaging findings. Moreover, future prospective, longitudinal studies will help determine whether the integration of S1R PET/MR imaging will improve the outcomes of chronic low back pain sufferers.Conclusion
Early results show promise for improved confidence and sensitivity in detecting sources of pain using full body ([18F]FTC-146) PET/MRI scan which can potentially improve patient management and outcomes. S1R imaging helped guide therapy in all patients which led to outcome improvements. Our study results strongly support the likelihood of achieving enhanced diagnostic sensitivity to sources of back pain with the proposed S1R imaging approach.Acknowledgements
We would like to acknowledge Dawn Holley, Kim Halbert, Bin Shen, Jessa Castillo, Medhi Khaligi and Gunilla Jacobsen for their technical and administrative assistance and Chris McCurdy Phd for chemical support. Financial support was provided in part by GE Healthcare and a Spectrum Grant. We wish to acknowledge support from Bracco Diagnostics who provide research support to the University of Wisconsin.References
1. Andronis L, Kinghorn P, Qiao S, Whitehurst DG, Durrell S, McLeod H. Cost-Effectiveness of Non-Invasive and Non-Pharmacological Interventions for Low Back Pain: a Systematic Literature Review. Appl Health Econ Health Policy. Apr 2017;15(2):173-201. doi:10.1007/s40258-016-0268-8
2. Luo X, Pietrobon R, Sun SX, Liu GG, Hey L. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine (Phila Pa 1976). Jan 1 2004;29(1):79-86. doi:10.1097/01.Brs.0000105527.13866.0f
3. Krismer M, van Tulder M. Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. Feb 2007;21(1):77-91. doi:10.1016/j.berh.2006.08.004
4. Tagliaferri SD, Miller CT, Owen PJ, et al. Domains of Chronic Low Back Pain and Assessing Treatment Effectiveness: A Clinical Perspective. Pain Pract. Feb 2020;20(2):211-225. doi:10.1111/papr.12846
5. Deyo RA, Von Korff M, Duhrkoop D. Opioids for low back pain. Bmj. Jan 5 2015;350:g6380. doi:10.1136/bmj.g6380
6. Florence CS, Zhou C, Luo F, Xu L. The Economic Burden of Prescription Opioid Overdose, Abuse, and Dependence in the United States, 2013. Med Care. Oct 2016;54(10):901-6. doi:10.1097/mlr.0000000000000625
7. Katz JN. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Joint Surg Am. Apr 2006;88 Suppl 2:21-4. doi:10.2106/jbjs.E.01273
8. Azad TD, Zhang Y, Stienen MN, et al. Patterns of Opioid and Benzodiazepine Use in Opioid-Naïve Patients with Newly Diagnosed Low Back and Lower Extremity Pain. J Gen Intern Med. Jan 2020;35(1):291-297. doi:10.1007/s11606-019-05549-8
9. Gilbert FJ, Grant AM, Gillan MG, et al. Does early imaging influence management and improve outcome in patients with low back pain? A pragmatic randomised controlled trial. Health Technol Assess. May 2004;8(17):iii, 1-131. doi:10.3310/hta8170
10. Urits I, Burshtein A, Sharma M, et al. Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment. Current Pain and Headache Reports. 2019/03/11 2019;23(3):23. doi:10.1007/s11916-019-0757-1
11. Ruiz-Cantero MC, González-Cano R, Tejada M, et al. Sigma-1 receptor: A drug target for the modulation of neuroimmune and neuroglial interactions during chronic pain. Pharmacol Res. Jan 2021;163:105339. doi:10.1016/j.phrs.2020.105339
12. Merlos M, Romero L, Zamanillo D, Plata-Salamán C, Vela JM. Sigma-1 Receptor and Pain. Handb Exp Pharmacol. 2017;244:131-161. doi:10.1007/164_2017_9
13. Shen B, Behera D, James ML, et al. Visualizing Nerve Injury in a Neuropathic Pain Model with [(18)F]FTC-146 PET/MRI. Theranostics. 2017;7(11):2794-2805. doi:10.7150/thno.19378
14. Yoon D, Cipriano P, Carroll I, et al. Sigma-1 receptor PET/MRI for identifying nociceptive sources of radiating low back pain. Journal of Nuclear Medicine. 2020;61(supplement 1):178-178.
Figures