1555
Evaluating the Effectiveness of the FRACTURE Sequence in Assessing Ossification of the Posterior Longitudinal Ligament in the Cervical Spine1The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Clinical & Technical Support, Philips Healthcare, Beijing, 100102, China, Beijing, China
Synopsis
Keywords: Skeletal, Skeletal, CT like image
Motivation: There is no consensus on the use of anterior or posterior surgery for ossification of the posterior longitudinal ligament (OPLL).
Goal(s): The purpose of this study was to evaluate the usefulness of the FRACTURE MRI sequence in comparison to CT in the detection of OPLL of the cervical spine.
Approach: Seven radiological parameters were analyzed though the inter-observer and inter-modality agreement.
Results: MRI with FRACTURE may be sufficient for the assessment of cervical spine OPLL, with good performance compared to CT in type of OPLL, distribution of OPLL, ossification thickness, canal-occupying ratio, K-line, and dural calcification.
Impact: In the evaluation of ossification of the posterior longitudinal ligament of the cervical spine, FRACTURE sequence might be a useful alternative to conventional CT scan.
Introduction
Posterior longitudinal ligament ossification (OPLL) of the cervical spine is a degenerative disease of the cervical spine [1]. OPLL is a common cause of cervical cord compression in Asian populations with a prevalence of 1.9%-4.3% in people aged more than 30 years in Japan and about 1.6-1.8% in China [2]. There is no recognized guideline for the treatment of cervical OPLL, especially for the choice of surgical methods, which is variable and generally depends on a variety of radiological parameters. Now CT is considered the "gold standard" for OPLL because of the high sensitivity for lesions of bony structures, but it does not show soft tissue lesions well. Recently, a potential clinical application of MRI for the evaluation of bony structure using a 3D fast field echo sequence resembling a CT using restricted echo-spacing (FRACTURE) sequence was reported [3,4]. The objective of this study was to evaluate the usefulness of the FRACTURE sequence in comparison the radiological parameters to CT in the detection of OPLL of the cervical spine.Methods
A total of 30 patients (20 men, 10 women; mean age, 53.8±5.5 years; range, 46–75 years) who performed CT and MRI of the cervical spine were included in this study. All MRI examinations were performed using a 3.0-T scanner (Ingenia Elition X; Philips Medical Systems, Best, The Netherlands) using a 20-channel head and neck coil. The 3D FRACTURE sequence was acquired with six in-phase echoes (Starting TE: 2.3 ms, TR: 28 ms, echo-spacing: 4.6 ms) , flip angle 15°, isotropic voxels (voxel size: 0.7 ×0.7×0.7 mm3) and a field of view of 180×169×70 mm3. The CT scan followed the clinical routine with a 0.625 mm slice thickness. The MR images and CT images were read with at least 4 weeks in between readings by two radiologists with 10 and 12 years of experience blinded to clinical information, respectively. According to these images, the following features were evaluated:OPLL classification, distribution of OPLL, K-line (+) or (-), dural calcification, whether there is a vacuum phenomenon in the intervertebral disc (categorical data); and ossification thickness and canal-occupying ratio (metrological data). For inter-modality comparison, the metrological data is recorded as the average of the two measurements. Meanwhile, if the judgment of the categorical data is inconsistent, a consensus will be made after discussion. The inter-observer agreement of FRUCTURE sequence and inter-modality agreement were analyzed. The Bland-Altman analysis with 95% limits of agreement (LOA) were used to assess the consistency of the metrological data. The Cohen kappa test of agreement was used to determine the agreement for the categorical data. A Cohen kappa value of 0.2 was defined as slight agreement, 0.21–0.40 as fair agreement, 0.41–0.60 as moderate agreement, 0.61–0.80 as strong agreement, and 0.81–1.00 as almost perfect agreement. All statistical analyses were performed using SPSS software (v. 26, Chicago, IL) and MedCalc software (v. 15.6.1, Ostend, Belgium) with P < 0.05 considered statistically significant.Results
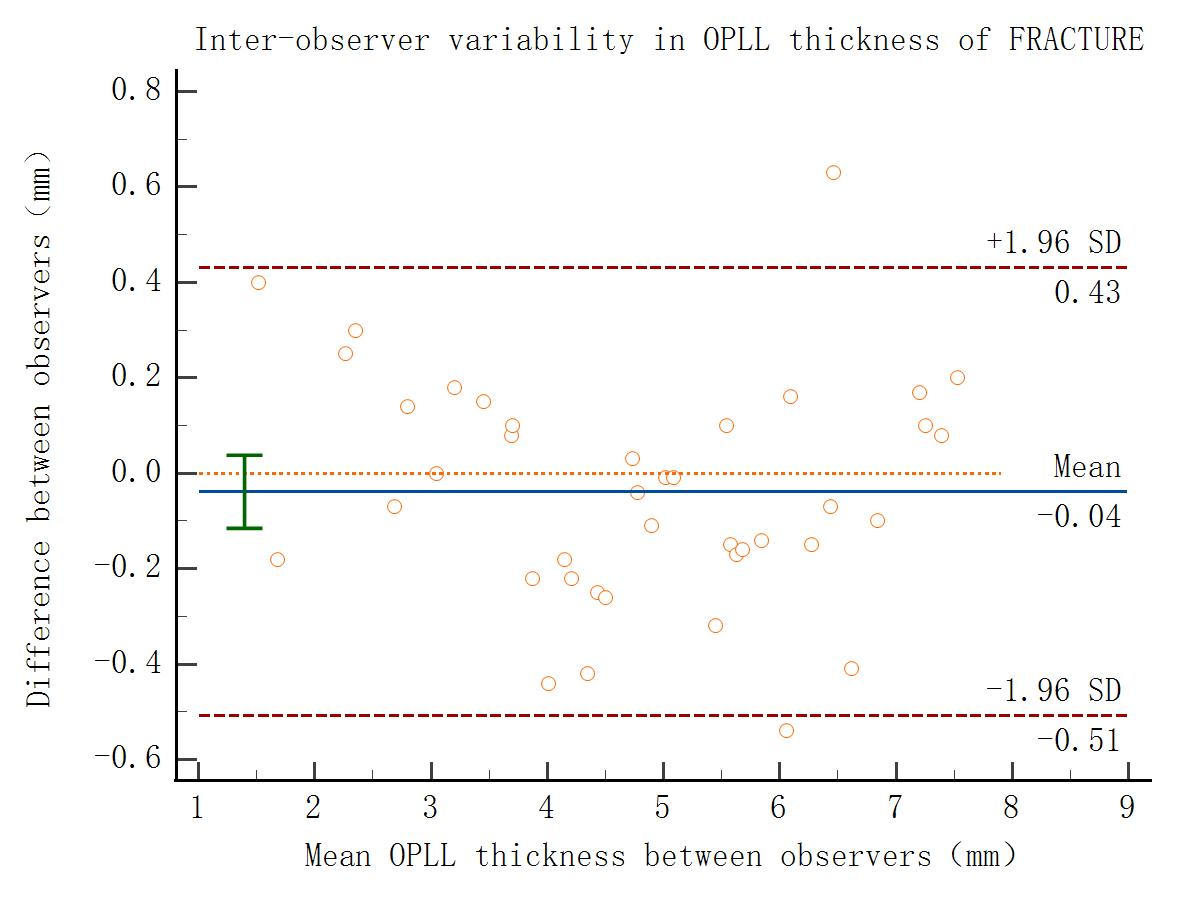
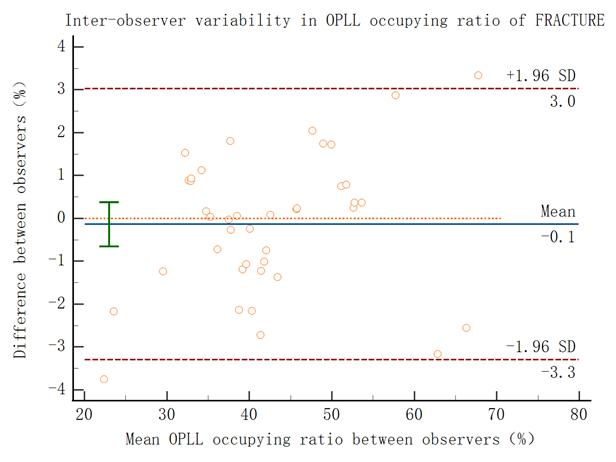
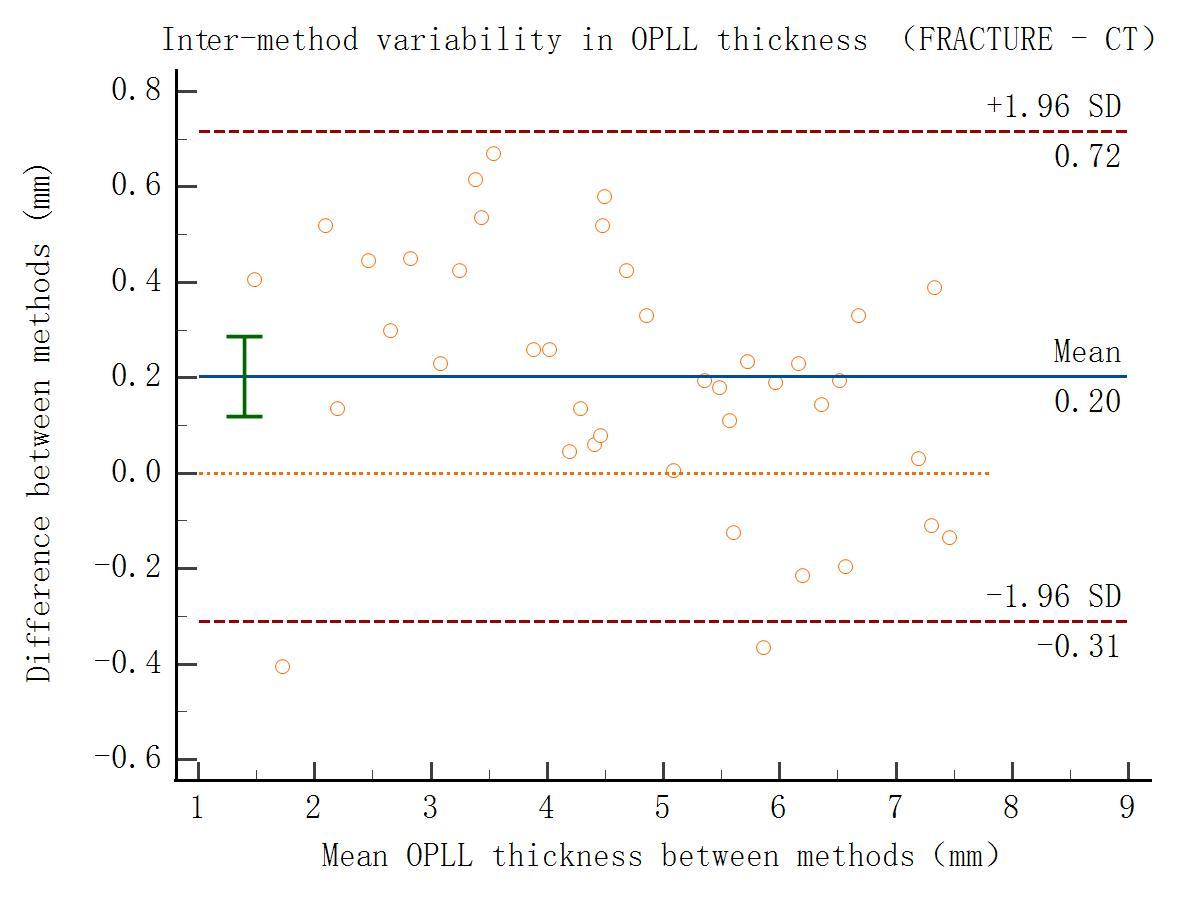
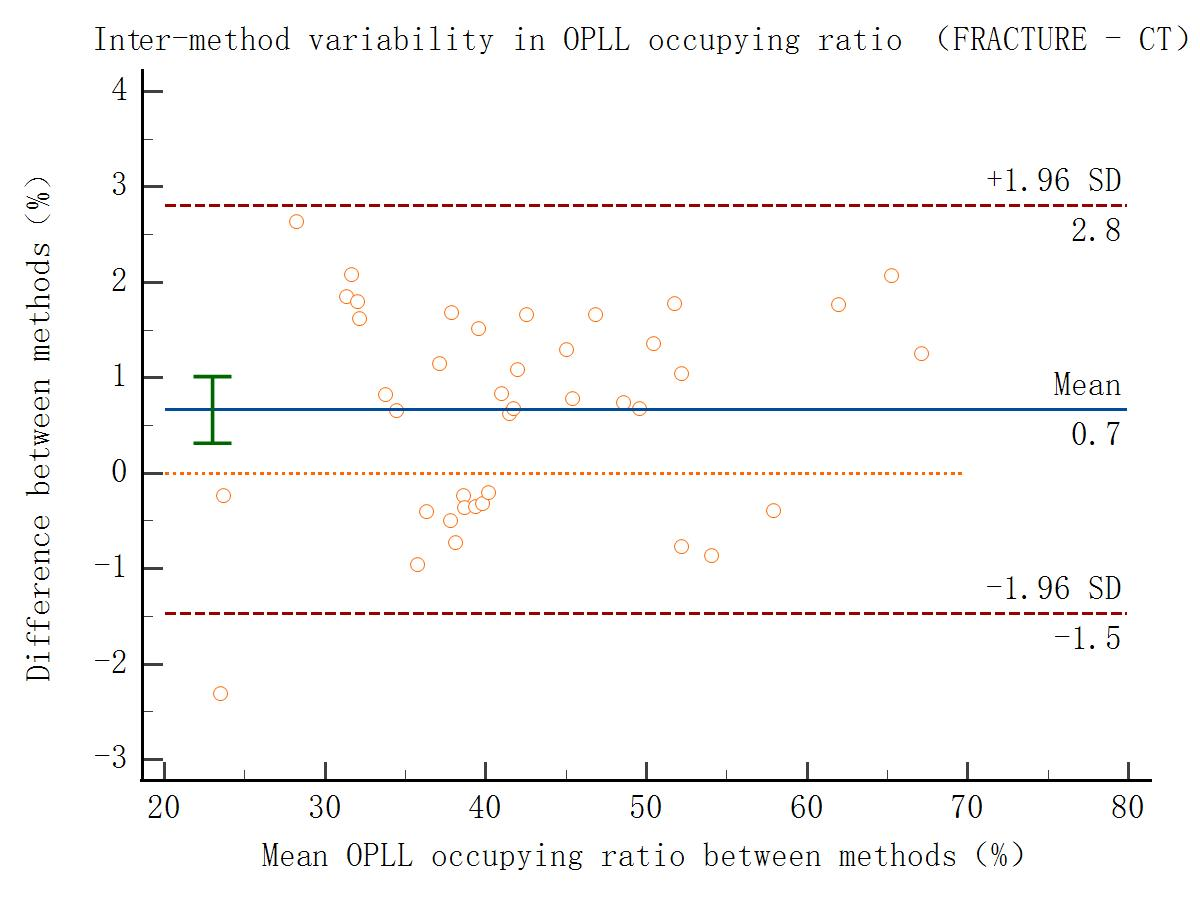
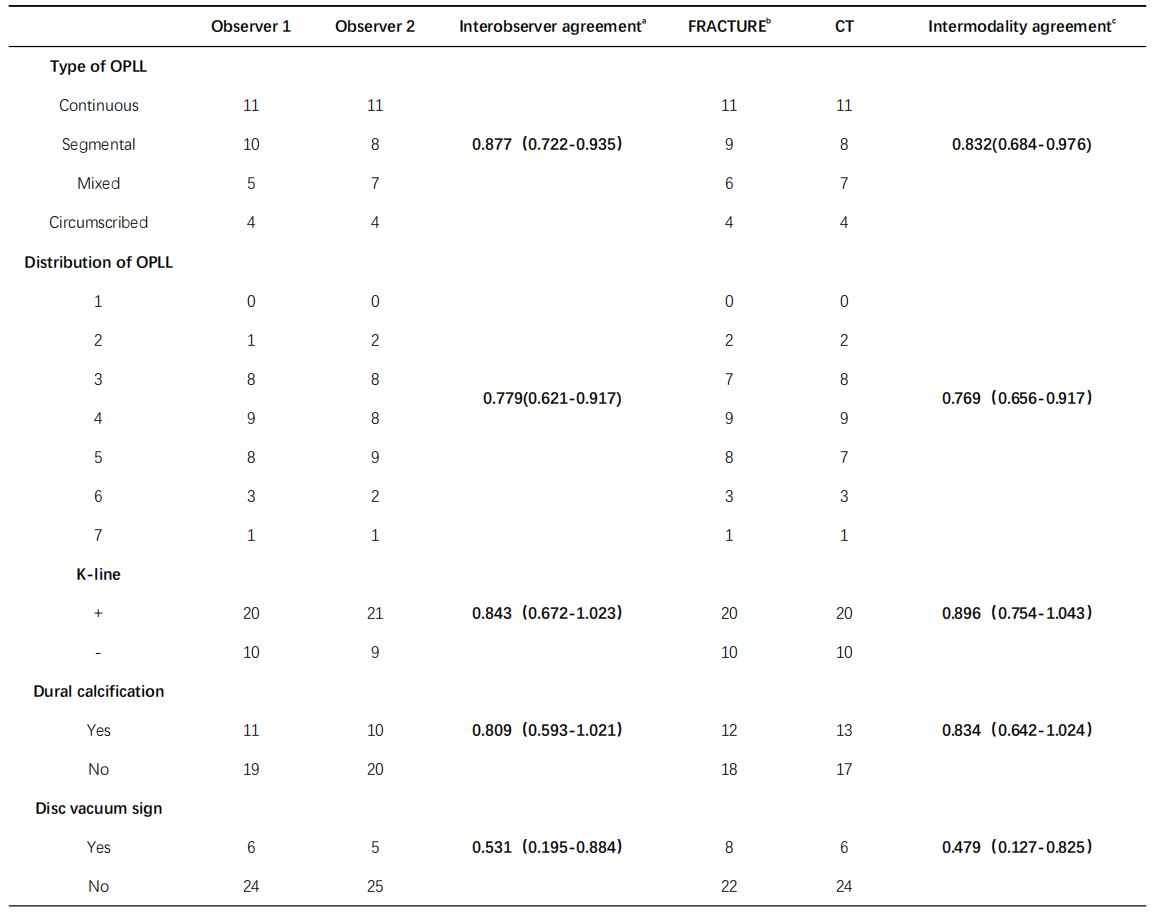
The inter-observer agreement of FRACTURE images and inter-modality agreement between FRACTURE images and CT images were calculated. Measurements of ossification thickness and canal-occupying ratio exhibited strong consistency among both the observers of the FRACTURE sequence (Fig.1 and Fig. 2) and the two types of examinations (Fig.3 and Fig. 4). As shown in Table 1, the inter-observer / inter-modality agreement was strong to perfect for the type of OPLL 0.877 (0.722-0.935) and 0.832 (0.684-0.976), distribution of OPLL 0.779 (0.621-0.917) and 0.769 (0.656-0.917), K-line, 0.843 (0.672-1.023) and 0.896 (0.754-1.043), dural calcification 0.809 (0.593-1.021) and 0.834 (0.642-1.024). However, consistency in detecting the intervertebral vacuum phenomenon was relatively poor, with values of 0.531 (0.195-0.884) and 0.479 (0.127-0.825).Discussion
In this study, excluding the assessment of intervertebral vacuum phenomenon, the imaging parameters measured using the FRACTURE sequence demonstrated strong interobserver consistency and exhibited a high degree of agreement when compared to data obtained from CT scans. However, we observed that the low proton density of air results in a conspicuous high signal in the FRACTURE sequence. This phenomenon may lead to the misinterpretation of intradiscal air accumulation, a consequence of intervertebral disc degeneration (commonly recognized as the " intervertebral vacuum phenomenon " in CT images), as calcification. These results suggest the importance of exercising caution when utilizing the FRACTURE sequence for identifying bony structures containing gas.Conclusion
In summary, the FRACTURE sequence offers a reliable radiological evaluation of cervical OPLL, demonstrating strong concordance with CT scans.Acknowledgements
No acknowledgement found.References
[1] Kim B-S, Moon M-S, Yoon MG, et al (2018) Prevalence of Diffuse Idiopathic Skeletal Hyperostosis Diagnosed by Whole Spine Computed Tomography: A Preliminary Study. Clin Orthop Surg 10:41–46.
[2] Sun X, Wang Y, Sun J, et al (2020) Consensus statement on diagnosis and treatment of cervical ossification of posterior longitudinal ligament from Asia Pacific Spine Society (APSS) 2020. J Orthop Surg 28:2309499020975213.
[3] Gascho D, Zoelch N, Tappero C, et al (2020) FRACTURE MRI: Optimized 3D multi-echo in-phase sequence for bone damage assessment in craniocerebral gunshot injuries. Diagn Interv Imaging 101:611–615.
[4] Johnson B, Alizai H, Dempsey M (2021) Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. Skeletal Radiol 50:1705–1713.
Figures