1554
Development of a whole spinal MRI-based tumor burden score method in participants with multiple myeloma: a pilot study of prognostic significance1Second Hospital of Shanxi Medical University, Taiyuan, China, 2Fifth hospital of Shanxi Medical University, Taiyuan, China, 3Shanxi Medical University, Taiyuan, China, 4GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Skeletal, MR Value
Motivation: Quantifying the extent of bone marrow infiltration or bone destruction plays a key role in assessing tumor burden and evaluating prognosis.
Goal(s): Previous semi-quantitative tumor burden scoring methods had limitations.
Approach: We developed a new whole spinal MRI-based tumor burden scoring method in participants with newly diagnosed multiple myeloma and to explore its prognostic significance by evaluating its role in predicting the early treatment response and its association with the R-ISS.
Results: The tumor burden score was an independent predictor of poor response and the AUC was 0.842. The tumor burden score was higher in R-ISS-III than in R-ISS-I and R-ISS-II.
Impact: This study quantified the extent of bone marrow infiltration or bone destruction in multiple myeloma and showed that high tumor burden scores were associated with poor early treatment response and high R-ISS stage.
Introduction
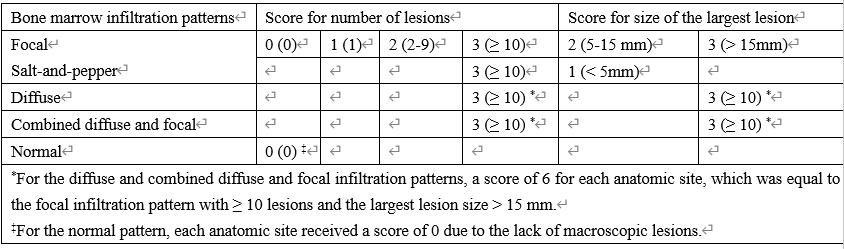
Multiple myeloma (MM) is a monoclonal plasma cell proliferative disorder and causes bone marrow infiltration or bone destruction, which is the most prominent feature of MM, occurring in approximately two-thirds of patients at diagnosis and in nearly all patients during their disease [1,2]. Quantifying the extent of bone marrow infiltration or bone destruction plays a key role in assessing tumor burden, guiding treatment, and evaluating prognosis [3]. Conventional radiography and computed tomography (CT) can visualize the number and size of bone destruction, but its sensitivity is limited because it cannot show bone marrow infiltration [4]. The limitation is now often complemented by fluorodeoxyglucose (FDG) positron emission tomography (PET)/ CT, which contains both tumor morphology and metabolism information. However, FDG PET/CT is expensive, radiative, insensitive to bone marrow infiltration and bone destruction located in the skull or ribs and has a high false-positive rate and false-negative rate [5-7]. Magnetic resonance imaging (MRI) is highly sensitive for detecting bone marrow infiltration because of the excellent soft-tissue contrast [8]. Moreover, whole-body (WB) MRI has been proved to have greater sensitivity and specificity in detecting bone marrow infiltration or bone destruction than FDG PET/CT [9]. There are five MRI patterns of bone marrow infiltration in MM: normal, focal, diffuse, combined focal and diffuse, and salt-and-pepper [10]. Previous studies have shown that the tumor burden and prognosis differ among five MRI patterns [11-14]. Subsequently, semi-quantitative tumor burden scoring methods based on MRI pattern began to emerge in MM. However, previous scoring methods had some controversies: (I) they did not cover all five MRI patterns (such as normal and salt-and-pepper patterns) [15], (II) the studies had variational scoring weight for the number and size of focal lesions [15,16], (III) scoring weight for diffuse and combined diffuse and focal patterns were not proper and did not correspond to their tumor burden [1,15]. WB MRI has the disadvantages of long scanning time, high requirements for technology and equipment, and difficult observation of humeral lesions due to limited field of view (FOV). MM lesions are mainly located in the axial skeleton, and the whole spine is the most affected area [17]. The whole spine scan is quick and convenient and is widely used in clinical practice as an alternative to the WB MRI. In our study, we try to develop a new, easy-to-implement scoring method for all five MRI patterns on whole spine scanning. We explored the prognostic significance of the new tumor burden score by evaluating its role in predicting the early treatment response and its association with the revised International Staging System (R-ISS) stage.Methods
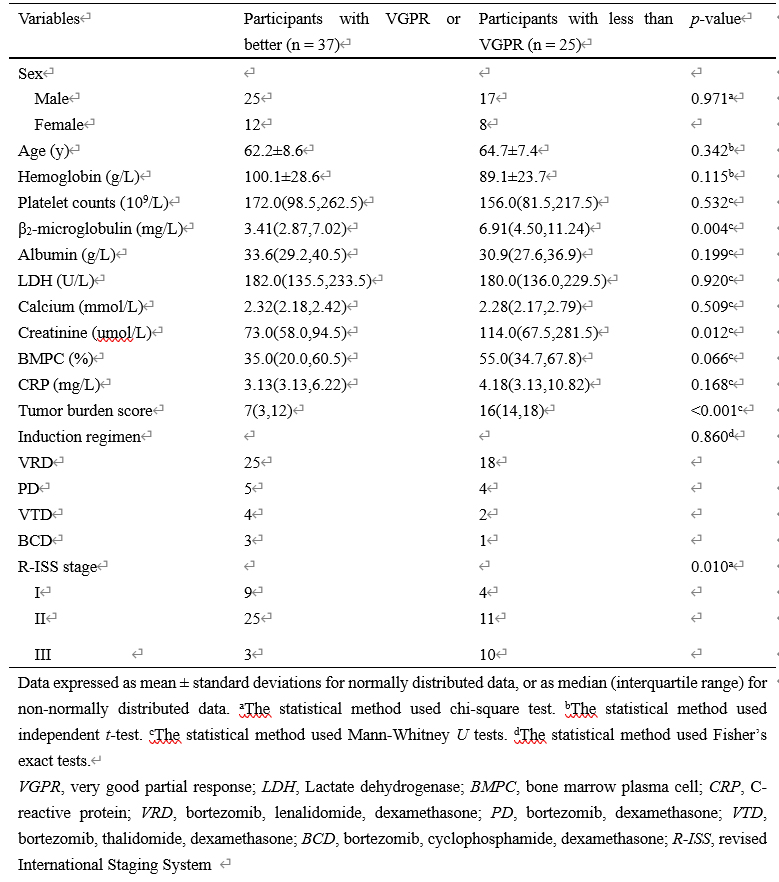
We prospectively recruited participants with newly diagnosed MM who were determined by the International Myeloma Working Group criteria (IMWG) from August 2020 to October 2022, collected their clinical data, and performed whole spinal MRI on them. We developed a new tumor burden scoring method according to the extent of bone marrow infiltration in five MRI patterns and calculated the tumor burden scores. Before treatment, all participants were divided into three groups based on the R-ISS stage, and then all participants were treated with one of the following first-line induction regimens: bortezomib, lenalidomide, dexamethasone (n = 43); bortezomib, dexamethasone (n = 9); bortezomib, thalidomide, dexamethasone (n = 6); bortezomib, cyclophosphamide, dexamethasone (n = 4). All participants were divided into good response [≥ very good partial response (VGPR)] and poor response (< VGPR) groups after four treatment cycles. Univariate (independent t test or Mann-Whitney U test and Chi-square test or Fisher’s exact test) and multivariate (logistic regression) analyses were used to identify independent predictors and then receiver operating characteristic (ROC) curve analyses were performed. The Kruskal-Wallis H test was used to compare the differences of tumor burden score between R-ISS stages.Results
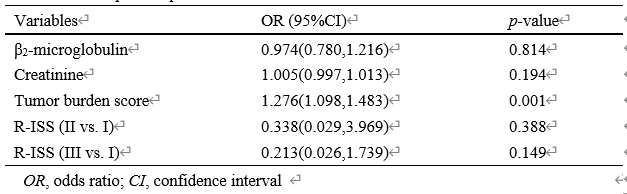
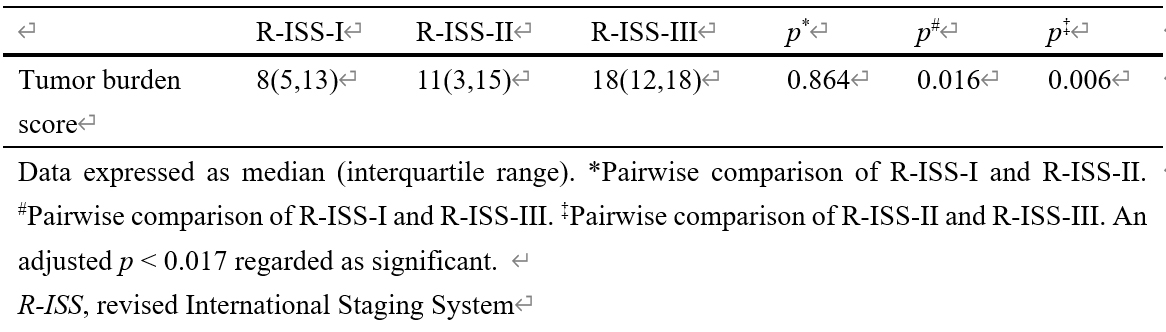
The new tumor burden scoring method was used in 62 participants to assess their tumor burden (median score, 12; range, 0-18). The β2-microglobulin, creatinine, tumor burden score and R-ISS stage were significant different between two treatment response groups (all p < 0.05). The tumor burden score (odds ratio 1.276, p = 0.001) was an independent predictor of poor response and the area under the curve (AUC) was 0.842. The tumor burden score was higher in R-ISS-III stage than in R-ISS-I and R-ISS-II stages (p = 0.016, p = 0.006 respectively).Conclusions
We developed a new tumor burden scoring method applicable to five patterns of bone marrow infiltration and calculated the tumor burden score. The tumor burden score was an excellent predictor of early treatment response and may serve as a supplemental marker for the R-ISS.Acknowledgements
No acknowledgement found.References
1. Ormond Filho AG, Carneiro BC, Pastore D et al (2019) Whole-Body Imaging of Multiple Myeloma: Diagnostic Criteria. Radiographics 39(4):1077–1097. https://doi.org/10.1148/rg.2019180096 2. Terpos E, Berenson J, Raje N, Roodman GD (2014) Management of bone disease in multiple myeloma. Expert Rev Hematol 7(1):113–125. https://doi.org/10.1586/17474086.2013.874943 3. Dall'Olio FG, Marabelle A, Caramella C et al (2022) Tumour burden and efficacy of immune-checkpoint inhibitors. Nat Rev Clin Oncol 19(2):75–90. https://doi.org/10.1038/s41571-021-00564-3 4. Giles SL, deSouza NM, Collins DJ et al (2015) Assessing myeloma bone disease with whole-body diffusion-weighted imaging: comparison with x-ray skeletal survey by region and relationship with laboratory estimates of disease burden. Clin Radiol 70(6):614–621. https://doi.org/10.1016/j.crad.2015.02.013 5. Shortt CP, Gleeson TG, Breen KA et al (2009) Whole-Body MRI versus PET in assessment of multiple myeloma disease activity. AJR Am J Roentgenol 192(4):980–986. https://doi.org/10.2214/AJR.08.1633 6. Regelink JC, Minnema MC, Terpos E et al (2013) Comparison of modern and conventional imaging techniques in establishing multiple myeloma-related bone disease: a systematic review. Br J Haematol 162(1):50–61. https://doi.org/10.1111/bjh.12346 7. Cavo M, Terpos E, Nanni C et al (2017) Role of 18F-FDG PET/CT in the diagnosis and management of multiple myeloma and other plasma cell disorders: a consensus statement by the International Myeloma Working Group. Lancet Oncol 18(4):e206–e217. https://doi.org/10.1016/S1470-2045(17)30189-4 8. Hillengass J, Landgren O (2013) Challenges and opportunities of novel imaging techniques in monoclonal plasma cell disorders: imaging "early myeloma". Leuk Lymphoma 54(7):1355–1363. https://doi.org/10.3109/10428194.2012.740559 9. Lecouvet FE, Boyadzhiev D, Collette L et al (2020) MRI versus 18F-FDG-PET/CT for detecting bone marrow involvement in multiple myeloma: diagnostic performance and clinical relevance. Eur Radiol 30(4):1927–1937. https://doi.org/10.1007/s00330-019-06469-1 10. Baur-Melnyk A, Buhmann S, Dürr HR, Reiser M (2005) Role of MRI for the diagnosis and prognosis of multiple myeloma. Eur J Radiol 55(1):56–63. https://doi.org/10.1016/j.ejrad.2005.01.017 11. Moulopoulos LA, Gika D, Anagnostopoulos A et al (2005) Prognostic significance of magnetic resonance imaging of bone marrow in previously untreated patients with multiple myeloma. Ann Oncol 16(11):1824–1828. https://doi.org/10.1093/annonc/mdi362 12. Dimopoulos MA, Hillengass J, Usmani S et al (2015) Role of magnetic resonance imaging in the management of patients with multiple myeloma: a consensus statement. J Clin Oncol 33(6):657–664. https://doi.org/10.1200/JCO.2014.57.9961 13. Dutoit JC, Verstraete KL (2016) MRI in multiple myeloma: a pictorial review of diagnostic and post-treatment findings. Insights Imaging 7(4):553–569. https://doi.org/10.1007/s13244-016-0492-7 14. Mai EK, Hielscher T, Kloth JK et al (2015) A magnetic resonance imaging-based prognostic scoring system to predict outcome in transplant-eligible patients with multiple myeloma. Haematologica 100(6):818-825. https://doi.org/10.3324/haematol.2015.124115 15. Dong H, Huang W, Ji X et al (2022) Prediction of Early Treatment Response in Multiple Myeloma Using MY-RADS Total Burden Score, ADC, and Fat Fraction From Whole-Body MRI: Impact of Anemia on Predictive Performance. AJR Am J Roentgenol 218(2):310-319. https://doi.org/10.3324/haematol.2015.124115 16. Lai AYT, Riddell A, Barwick T et al (2020) Interobserver agreement of whole-body magnetic resonance imaging is superior to whole-body computed tomography for assessing disease burden in patients with multiple myeloma. Eur Radiol 30(1):320-327. https://doi.org/10.1007/s00330-019-06281-x 17. Silbermann R, Roodman GD (2013) Myeloma bone disease: pathophysiology and management. J Bone Oncol 2(2):59–69. https://doi.org/10.1016/j.jbo.2013.04.001Figures