1552
Relationship between Modic Change and Resorption of Ruptured Lumbar Disc Herniation Based on MRI: A Longitudinal Study1Chengdu Sport University, Chengdu Sichuan, China, 2Sichuan Province Orthopedic Hospital, Chengdu Sichuan, China, 3GE HealthCare MR Research, Beijing, China
Synopsis
Keywords: Bone, Cartilage
Motivation: Ruptured lumbar disc herniation (RLDH) can lead to severe clinical symptoms, significantly impacting patients' daily lives.
. Understanding factors influencing disc resorption, particularly Modic change (MC), is crucial for making treatment decisions.
Goal(s): To investigate the relationship between MC and the occurrence of disc resorption in RLDH patients.
Approach: This longitudinal study examined the presence of MC at baseline and assessed disc resorption at follow-up to determine the potential influence of MC on RLDH resorption.
Results: The study revealed that MC is an independent influencing factor for RLDH resorption failure, highlighting its significance in the management of this condition.
Impact: First, our study validated the efficacy of nonsurgical treatment of RLDH in resorption. Second, we demonstrated that MC is an independent factor hindering resorption, which helps clinicians to forecast resorption in RLDH patients, to select appropriate treatment methods.
Introduction
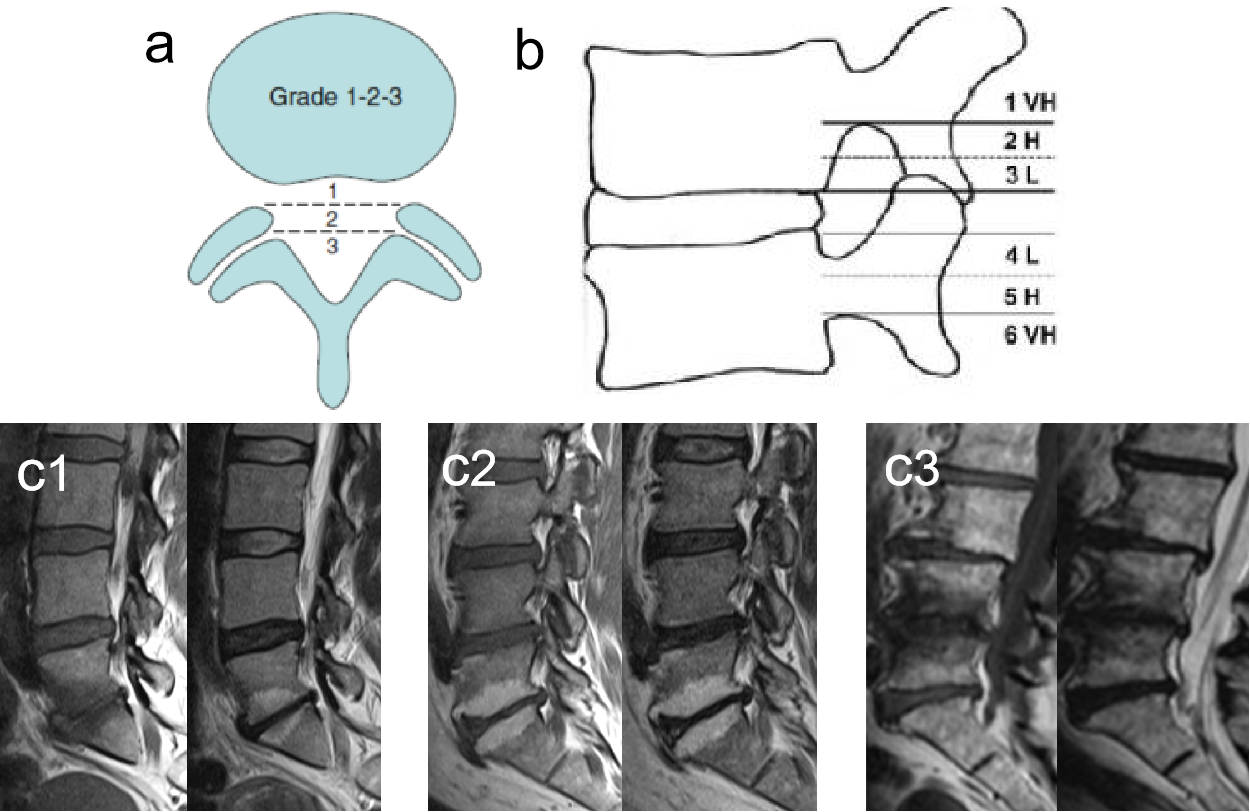
Ruptured lumbar disc herniation (RLDH) is characterized by significant protrusion and severe clinical symptoms, often necessitating surgical intervention. Previous studies have indicated that approximately 60% of LDH patients may experience spontaneous reabsorption, alleviating pressure and chemical stimulation on the nerve roots and spinal cord1. However, these studies mostly used the volume method to evaluate protrusion size, which may not accurately reflect patients' clinical symptoms2,3. Additionally, the location of the protrusion had a greater impact on clinical symptoms than its size. In this study, alternative methods that could better reflect the clinical symptoms of patients, such as MSU classification4 and the classification of disc migration5 were used to evaluate the situation of disc regression (Figure 1). The study also explored the association of baseline MC with disc resorption to help clinicians determine the prognosis of LDH patients.Methods
Patients: After IRB-approved written informed consent was obtained, 65 patients with single-segment RLDH at the L4/5 or L5/S1 level underwent 3.0T routine lumbar MRI scanning (SIGNA Architect, GE Healthcare) and were enrolled in the study. Subsequently, each patient underwent a repeat lumbar MRI scan 3 to 12 months after receiving nonsurgical resorption treatment.Imaging parameters: The MR scan included routine sagittal T2- weighted imaging, T2-weighted (2.0x2.0x2.0mm3, TR =8.0 ms, TE=3.6 ms, number of TEs=6, number of shots =2).
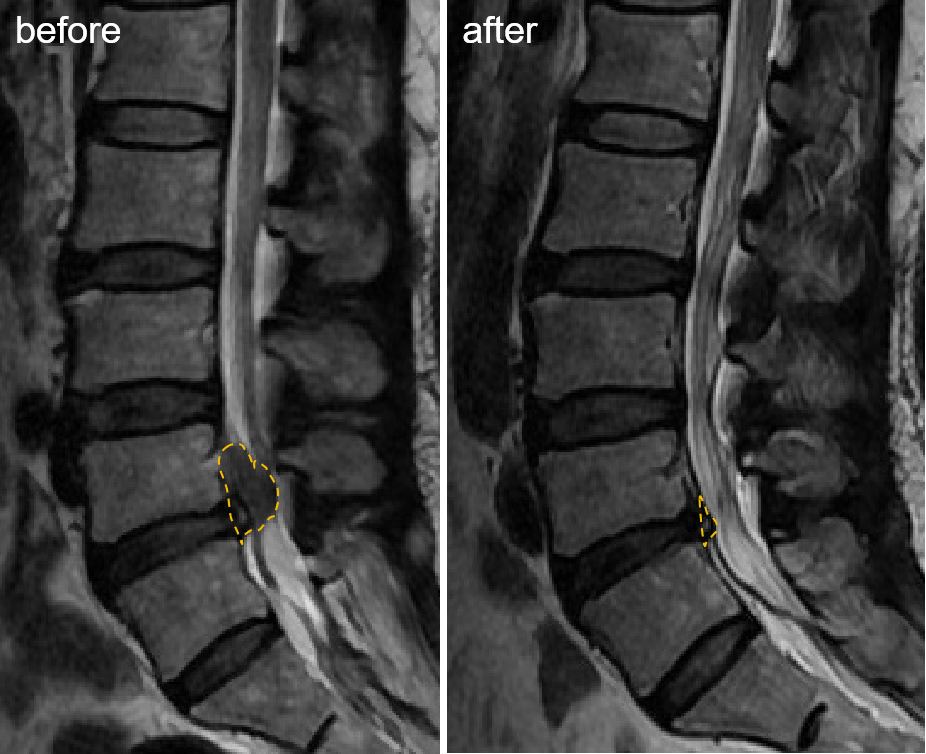
Data processing: The maximum protrusion area of the disc beyond the posterior longitudinal ligament was manually delineated in sagittal MRI images of the first and second scan, respectively. Patients with resorption rate [(first area-review area) / first area * %] > 30% were divided into resorption group (Figure 2), and patients with ≤ 30% were divided into non-resorption group. The degree of disc herniation was graded according to MSU classification4 and the classification of disc migration5 (Figure 1). The presence or absence of a baseline MC is determined based on the most commonly used MC concepts6.
Statistical analysis: All analyses were performed using SPSS 22.0 software and GraphPad Prism (GraphPad Software, San Diego, CA). Paired sample t test and paired sample rank sum test were used to analyze whether RLDH patients had reabsorption before and after nonsurgical treatment. Chi-square tests were used to analyze differences in MSU classification, classification of disc migration, and baseline MC distribution between reabsorbed and non-reabsorbed groups. Binary logistic regression was used to determine whether baseline MC was an independent factor in disc herniation resorption.
Results
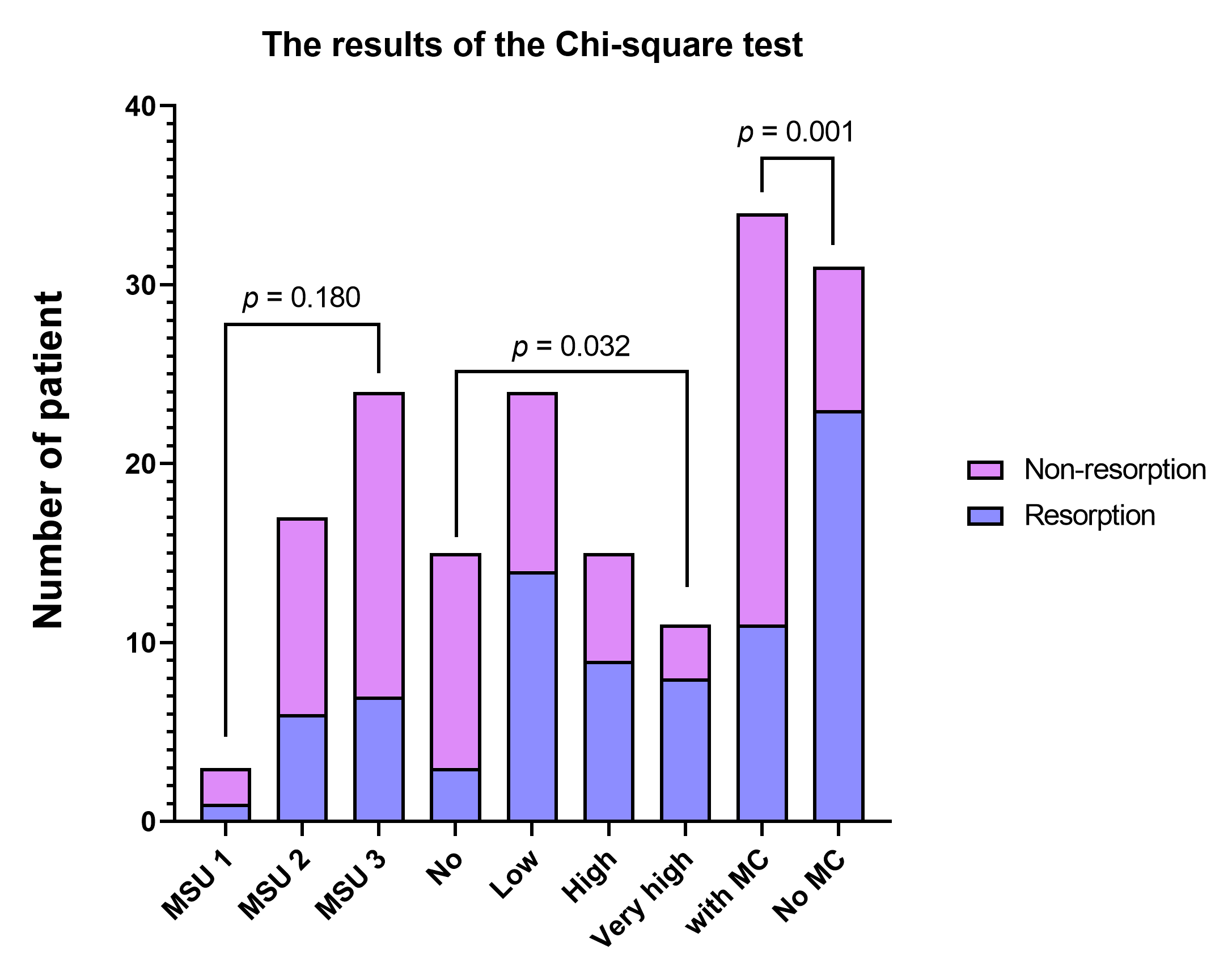
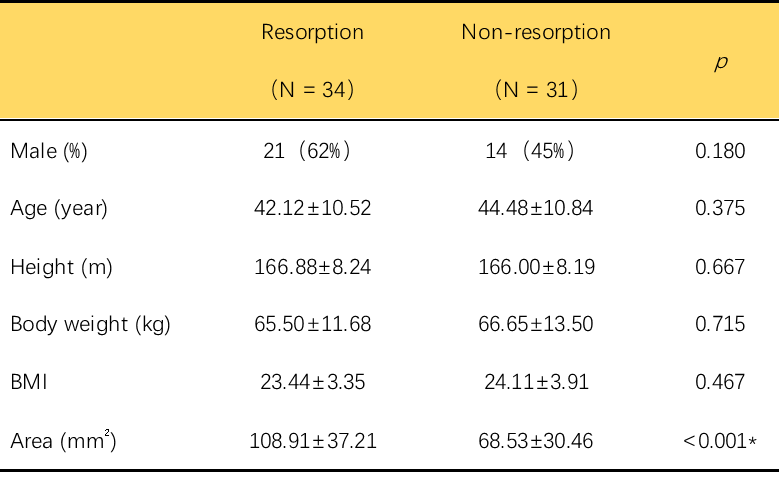
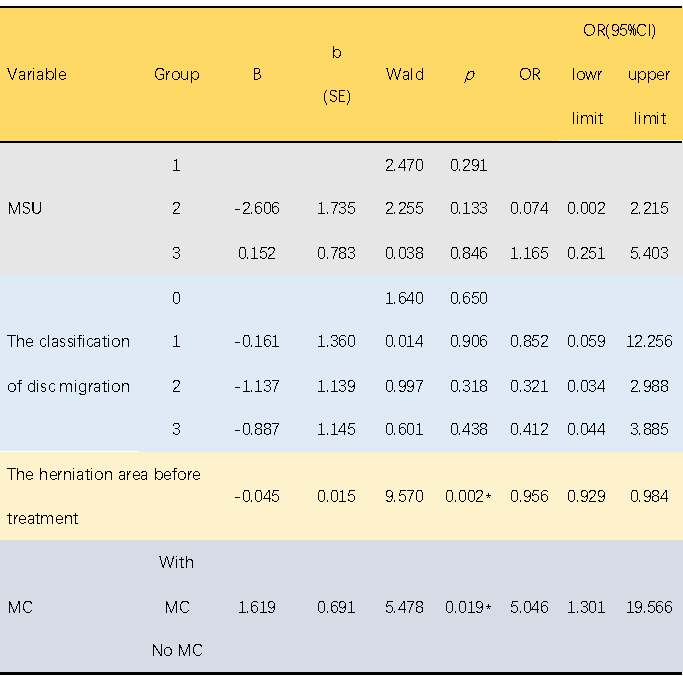
34 RLDH patients (52%) occurred resorption in all subjects. As shown in Table 1, there were no statistically significant differences in sex, age, height and body weight between resorption group and non-resorption group. There were significant differences in protrusion area (before, 89.65±39.52; after, 59.10±32.34; p<0.001), MSU Classification (p<0.001) and the classification of disc migration (p=0.001) between the twice examinations (Figure 3). There were significant differences in the herniation area (p<0.001), the classification of disc migration (p=0.032) and MC (p=0.001) at baseline between resorption group and non-resorption group. Table 2 shows that the herniation area before treatment and baseline MC were independent factors affecting resorption.Discussion
Our study confirmed the possibility of PLDH resorption after nonsurgical treatment, which is consistent with previous studies1,3. The MSU classification and the classification of disc migration were significantly improved after conservative treatment, which suggesting that resorption not only be a radiographic change but also reflects the improvement of the patient's symptoms. This study found that MC is an independent risk factor that prevents ruptured disc resorption. MC is often secondary to endplate rupture7, indicating that the disc herniated tissue near the MC may include endplate fragments, which is one of the reasons for the failure of resorption. The blood supply of the intervertebral disc adjacent to MC will be abnormally affected. According to the mechanism of disc resorption8,9, the blood supply around the protrusion will be reduced, and the apoptosis, dehydration, and phagocytosis of macrophages will be weakened, resulting in the failure of resorption. The larger the area of the protrusion, the greater the possibility of resorption, this is because the increase of the contact area between the nucleus pulposus and the dural sac is conducive to resorption, which is consistent with previous studies10.Conclusion
It is possible for RLDH to reabsorb through nonsurgical treatment. RLDH patients with MC are less likely to reabsorb, and clinicians should pay attention to the effect of MC when estimating resorption in patients using non-surgical treatment.Acknowledgements
No acknowledgement found.References
1. Wang Y, Dai G, Jiang L, et al. The incidence of regression after the non-surgical treatment of symptomatic lumbar disc herniation: a systematic review and meta-analysis. BMC Musculoskelet Disord 2020;21(1):530; doi: 10.1186/s12891-020-03548-z.
2. Hong J, Ball PA. IMAGES IN CLINICAL MEDICINE. Resolution of Lumbar Disk Herniation without Surgery. N Engl J Med 2016;374(16):1564; doi: 10.1056/NEJMicm1511194.
3. Ma Z, Yu P, Jiang H, et al. Conservative Treatment for Giant Lumbar Disc Herniation: Clinical Study in 409 Cases. Pain Physician 2021;24(5):E639–E648.
4. Mysliwiec LW, Cholewicki J, Winkelpleck MD, et al. MSU Classification for herniated lumbar discs on MRI: toward developing objective criteria for surgical selection. Eur Spine J 2010;19(7):1087–1093; doi: 10.1007/s00586-009-1274-4.
5. Kim CH, Chung CK, Woo JW. Surgical Outcome of Percutaneous Endoscopic Interlaminar Lumbar Discectomy for Highly Migrated Disk Herniation. Clinical Spine Surgery: A Spine Publication 2016;29(5):E259–E266; doi: 10.1097/BSD.0b013e31827649ea.
6. Herlin C, Kjaer P, Espeland A, et al. Modic changes—Their associations with low back pain and activity limitation: A systematic literature review and meta-analysis. Grasso G. ed. PLoS ONE 2018;13(8):e0200677; doi: 10.1371/journal.pone.0200677.
7. Feng Z, Liu Y, Yang G, et al. Lumbar Vertebral Endplate Defects on Magnetic Resonance Images: Classification, Distribution Patterns, and Associations with Modic Changes and Disc Degeneration. Spine 2018;43(13):919–927; doi: 10.1097/BRS.0000000000002450.
8. Cunha C, Silva AJ, Pereira P, et al. The inflammatory response in the regression of lumbar disc herniation. Arthritis Res Ther 2018;20(1):251; doi: 10.1186/s13075-018-1743-4.
9. Elkholy AR, Farid AM, Shamhoot EA. Spontaneous Resorption of Herniated Lumbar Disk: Observational Retrospective Study in 9 Patients. World Neurosurgery 2019;124:e453–e459; doi: 10.1016/j.wneu.2018.12.115.
10. Latif R, Imran S, Ahmad I, et al. Vertebral Endplate Changes Correlate with Presence of Cartilaginous Endplate in the Herniated Disc Tissue: Factor Predicting Failure of Conservative Treatment. Asian Spine J 2022;16(2):212–220; doi: 10.31616/asj.2021.0106.
Figures