1551
Correlation between MRI manifestations of lumbar disc herniation and fatty infiltration of paravertebral muscles and chronic low back pain1The First Affiliated Hospital of Kunming Medical University, kunming, China, 2GE HealthCare MR Research, beijing, China
Synopsis
Keywords: Muscle, Quantitative Imaging
Motivation: Chronic low back pain (CLBP) is frequently associated with fatty infiltration and alterations in the cross-sectional area (CSA) of the paravertebral muscles. However, the precise relationship between disc-related changes and paravertebral muscles remains incompletely understood.
Goal(s): Study correlation between lumbar disc herniation, paravertebral muscle fat infiltration, CSA and chronic low back pain.
Approach: MRI images of the lumbar spine were analyzed in patients with chronic low back pain to correlate findings with paraspinal muscle CSA and PDFF.
Results: CLBP patients with disc herniation had lower PDFF in the multifidus muscle at L4/5 and reported higher pain levels (VAS score) than the control group.
Impact: This study provides valuable insights for clinicians, enabling them to implement targeted interventions for CLBP patients based on specific MRI findings and key characteristics of muscle remodeling.
Introduction
The lumbar paraspinal muscles are crucial in maintaining the stability of the spine, but in chronic low back pain (CLBP) patients1,2, these muscles undergo size reduction and fat infiltration3. Imaging techniques such as CT, MRI, and US are used to assess these changes. Reduction in paraspinal muscle cross-sectional area is an indicator of muscle atrophy, but some studies suggest that there is no significant reduction in CLBP patients. This may be due to the replacement of atrophied muscle fibers by fat4. Therefore, it is essential to observe micro-level fat infiltration in the paraspinal muscles. However, there is still controversy surrounding research results due to differences in measurement methods5.Method
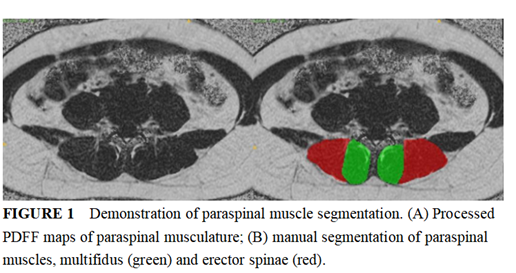
The study received approval from the institutional review board, and verbal informed consent was obtained from all participants.A total of 494 patients with chronic low back pain (201 males and 293 females) were prospectively collected, with an average age of 45.75 years.All patients underwent standard preoperative MRI examination on a 3.0T MR scanner (SIGNA Architect, GE Healthcare, USA) with 32-channels flexible coil. The key sequence parameters and scanning time were as follows: the sagittal T1WI and axial T2WI of the lumbar spine conventional sequence, as well as the quantitative sequence 2D-IDEAL axis and 3D-IDEAL-IQ axis.Two radiologists will discuss and agree on any disagreements. Muscle CSA of the bilateral multifidus and erector spinae muscles at the central level of the L4-S1 intervertebral disc was measured using in-phase and anti-phase images. The PDFF value of the paravertebral muscles was measured using the IDEAL-IQ sequence. The shapes of the muscles were outlined manually in the images.SPSS 26.0 software by IBM Corp was used for statistical analysis. Categorical variables were presented using counts and percentages. Mann-Whitney U test and Kruskal-Wallis test were used to compare groups and examine differences in lumbar disc herniation, muscle fat infiltration, and cross-sectional area. Non-parametric tests were used to analyze the correlation between CLBP, intervertebral disc herniation, VAS, and paravertebral muscles CSA and PDFF.Results
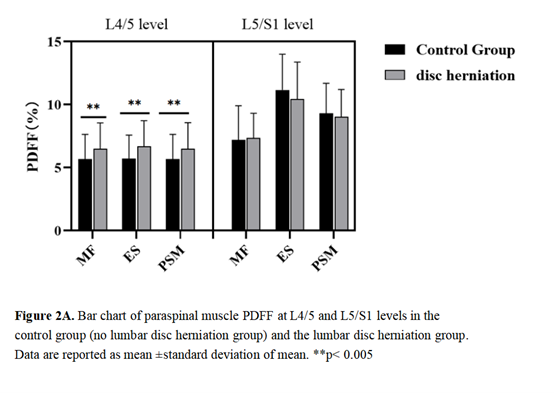
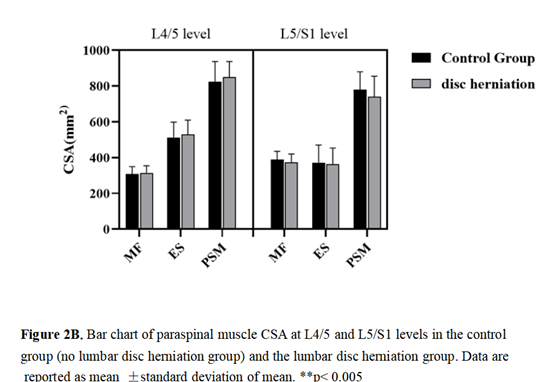
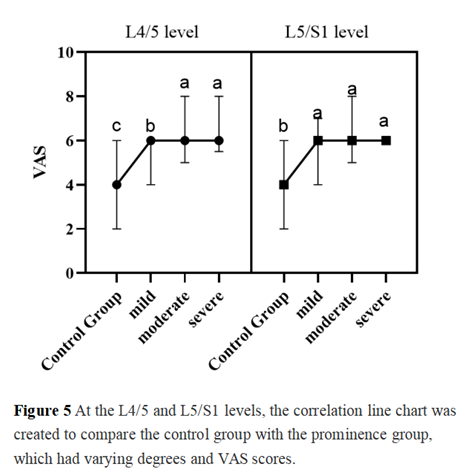
patients with CLBP and disc herniation exhibited a significantly smaller PDFF of the multifidus muscle at the L4/5 level compared to those with herniation alone (p<0.05). Additionally, CLBP patients with disc herniation reported a significantly higher VAS score for pain (4, range 2-6) than the control group (6, range 4-6) (p<0.05). However, there was no significant difference in the change of paravertebral muscle cross-sectional area between patients with low back pain with and without intervertebral disc herniation.Discussion
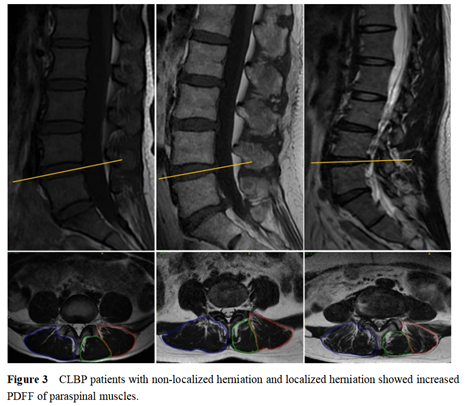
Our study found that patients with CLBP and LDH at the L4/5 level had higher PDFF than those without LDH. Additionally, the severity and type of disc herniation were associated with pain levels. CLBP poses significant challenges to clinical diagnosis and management due to its prolonged course and uncertainty regarding the source of pain6, 7, 8. Our study found that disc herniation type and presence are significantly associated with pain in patients with CLBP and lumbar disc herniation at L4/5 and L5/S1 levels. The severity of disc herniation is positively correlated with higher visual pain scores. However, there is no correlation between the CSA and PDFF of the corresponding paravertebral muscles and pain. Factors such as inflammation, nerve compression, and disc herniation are more likely to influence pain in CLBP patients than changes in the paravertebral muscles. Nerve root compression caused by the protruding disc structure is the main cause of lower back pain in patients with CLBP and concomitant lumbar disc herniation.Conclusions
For those with chronic low back pain due to intervertebral disc herniation, surgery and paravertebral muscle function enhancement are recommended for best results. Rehabilitation should be pursued alongside surgical intervention.Acknowledgements
No acknowledgement found.References
1. Rezazadeh, F.; Taheri, N.; Okhravi, S. M.; Hosseini, S. M., The relationship between cross-sectional area of multifidus muscle and disability index in patients with chronic non-specific low back pain. Musculoskelet Sci Pract 2019, 42, 1-5.
2. Ranger, T. A.; Cicuttini, F. M.; Jensen, T. S.; Heritier, S.; Urquhart, D. M., Paraspinal muscle cross-sectional area predicts low back disability but not pain intensity. Spine J 2019, 19 (5), 862-868.
3. Paalanne, N.; Niinimaki, J.; Karppinen, J.; Taimela, S.; Mutanen, P.; Takatalo, J.; Korpelainen, R.; Tervonen, O., Assessment of association between low back pain and paraspinal muscle atrophy using opposed-phase magnetic resonance imaging: a population-based study among young adults. Spine (Phila Pa 1976) 2011, 36 (23), 1961-8.
4. Ranger, T. A.; Cicuttini, F. M.; Jensen, T. S.; Peiris, W. L.; Hussain, S. M.; Fairley, J.; Urquhart, D. M., Are the size and composition of the paraspinal muscles associated with low back pain? A systematic review. Spine J 2017, 17 (11), 1729-1748
5. Huang, Y.; Wang, L.; Zeng, X.; Chen, J.; Zhang, Z.; Jiang, Y.; Nie, L.; Cheng, X.; He, B., Association of Paraspinal Muscle CSA and PDFF Measurements With Lumbar Intervertebral Disk Degeneration in Patients With Chronic Low Back Pain. Front Endocrinol (Lausanne) 2022, 13, 792819.
6. Hu, Y.; Yang, Z.; Li, Y.; Xu, Y.; Zhou, X.; Guo, N., Anxiety Symptoms and Associated Factors Among Chronic Low Back Pain Patients in China: A Cross-Sectional Study. Frontiers in Public Health 2022, 10. 7. Nguyen, C.; De Sèze, M.; Rannou, F., The challenges of precision medicine in chronic low back pain: Lessons learned from active discopathy. Annals of Physical and Rehabilitation Medicine 2021, 64 (2).
8. Bailey, J. F.; Fields, A. J.; Ballatori, A.; Cohen, D.; Jain, D.; Coughlin, D.; O'Neill, C.; McCormick, Z.; Han, M.; Krug, R.; Demir-Deviren, S.; Lotz, J. C., The Relationship Between Endplate Pathology and Patient-reported Symptoms for Chronic Low Back Pain Depends on Lumbar Paraspinal Muscle Quality. Spine (Phila Pa 1976) 2019, 44 (14), 1010-1017.
Figures