1550
UTE MRI of Discovertebral Junction in Chronic Low Back Pain Subjects1Radiology, University of California, San Diego, San Diego, CA, United States
Synopsis
Keywords: Cartilage, MSK, Spine, Lumbar, Endplate, Intervertebral Disc
Motivation: Despite crucial roles in normal function of the lumbar spine, discovertebral junction (DVJ) is seldom evaluated during MRI.
Goal(s): Using ultrashort echo time (UTE) MRI, evaluate DVJ in subjects with chronic low back pain and asymptomatic controls.
Approach: Disc degeneration was assessed using Pfirrmann grading on the conventional spin echo T2, while DVJ morphology was assess using UTE MRI. Effect of low back pain on disc degeneration and abnormal DVJ morphology was assessed.
Results: UTE MRI of the DVJ was feasible in vivo. In the symptomatic group, statistically greater prevalence of disc degeneration and abnormal DVJ morphology were found, suggesting a possible pain-correlation.
Impact: This study advances MR imaging of the lumbar spine, suggesting that DVJ may be implicated in low back pain and the need for wider assessment of DVJ in routine lumbar MRI.
INTRODUCTION
Chronic low back pain (CLBP) is a significant health concern with a high socioeconomic cost. CLBP has been associated with intervertebral disc (IVD) degeneration,1 and vertebral endplate lesions such as Schmorl’s nodes.2 Discovertebral Junction (DVJ) is the interfacial region between the vertebral body and IVD, consisting of 1 to 2 mm thick cartilaginous endplate (CEP) and calcified cartilage, with important roles in mechanical stabilization and nutrient transport. MRI of the DVJ has been facilitated with advances in ultrashort echo time (UTE) MRI, with histological correlations establishing the basis for the UTE MR morphology of the DVJ. Normal DVJ exhibits distinct and continuous line of high signal intensity, while abnormal DVJ deviates from this morphology. The goal of this study was to evaluate DVJ in CLBP and normal subjects, to compare the prevalence of different UTE MR morphologies.METHODS
Subjects: A total of 48 subjects were recruited. These included 13 asymptomatic (Asx) volunteers (mean age 33.8+/-9.7 yo, 6 female) and 35 symptomatic (Sx) subjects (48.6+/-16.4 yo, 13 female).MRI: Imaging was performed on a 3-T system (GE Discovery 750) with posterior spine coil. Imaging protocol included sagittal fast spin echo (FSE) T2 weighted (Figure 1; TR=4600 ms, TE=102 ms, matrix=224x224, slice=3 mm, FOV=24 cm, time=2:14 min) and 3D UTE (Figure 2; TR=40 ms, TE=0.03 and 4.6 ms, number of spokes=6,000; matrix=256x256, slice=2 mm, FOV=24 cm, FA=2 deg, time = 4:00 min). For UTE, both the 1st echo image and digital subtraction image (1st echo minus 2nd echo) were evaluated. While the subtraction image provided a better contrast for the DVJ, when the image was too noisy, the 1st echo image was used instead. When the image quality was too poor (due to artifacts or low SNR for example), they were not included in the reading.
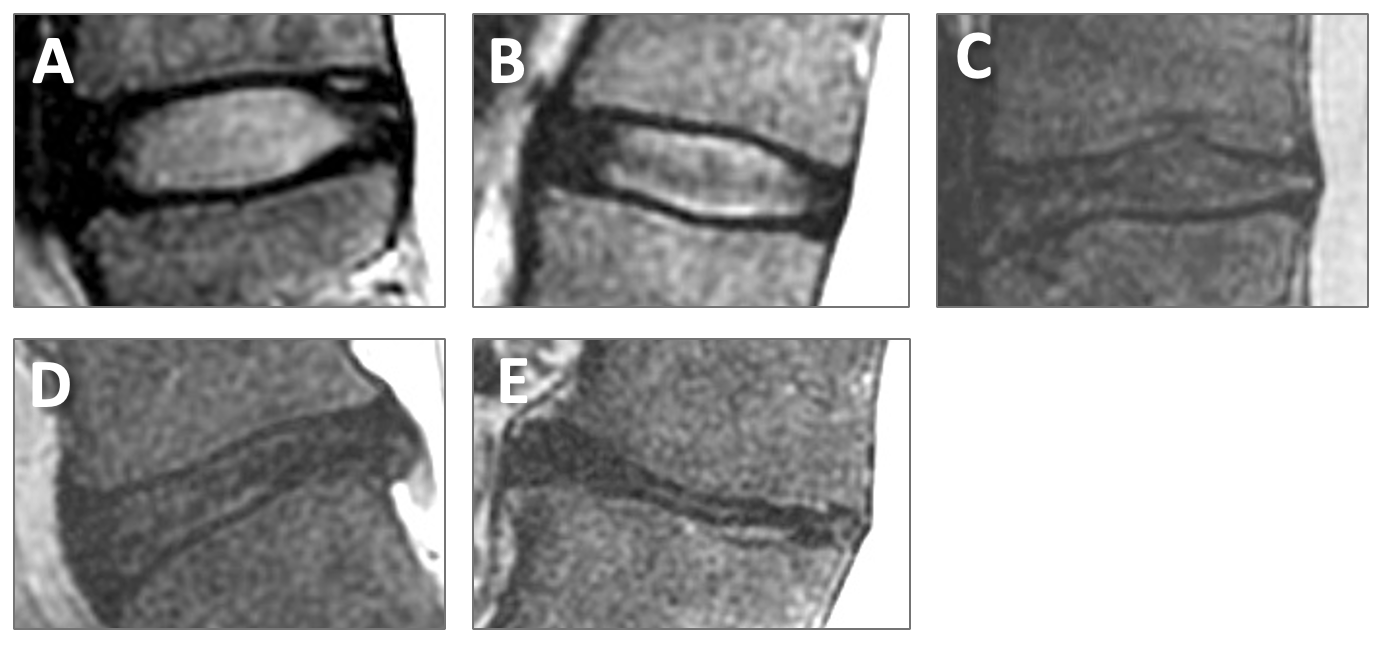
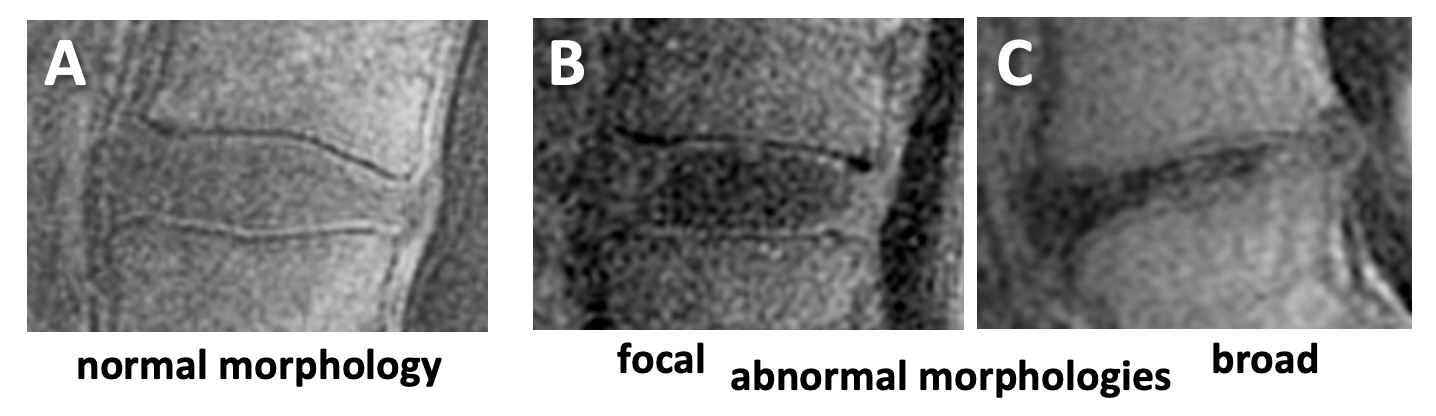
MR Evaluation: On FSE T2 images, Pfirrmann grading3 (Figure 1, grade 1=best, 5=worst) was used to assess disc degeneration. For DVJ morphology, we evaluated each DVJ independently: a normal DVJ morphology was a distinct and continuous line of high signal intensity (Figure 2A) and was given a DVJ grade of 0, while an abnormal DVJ morphology was any deviation from this, including signal loss, thickening, or irregularity. A Focal abnormality was graded as 1 (Figure 2B), while a broadly seen abnormality was graded as 2 (Figure 2C).
Statistics: To determine differences in mean values, t-test was used. To determine the differences between cohorts (Asx vs Sx) in the disc and DVJ grades, contingency table with chi-square test was used.
RESULTS
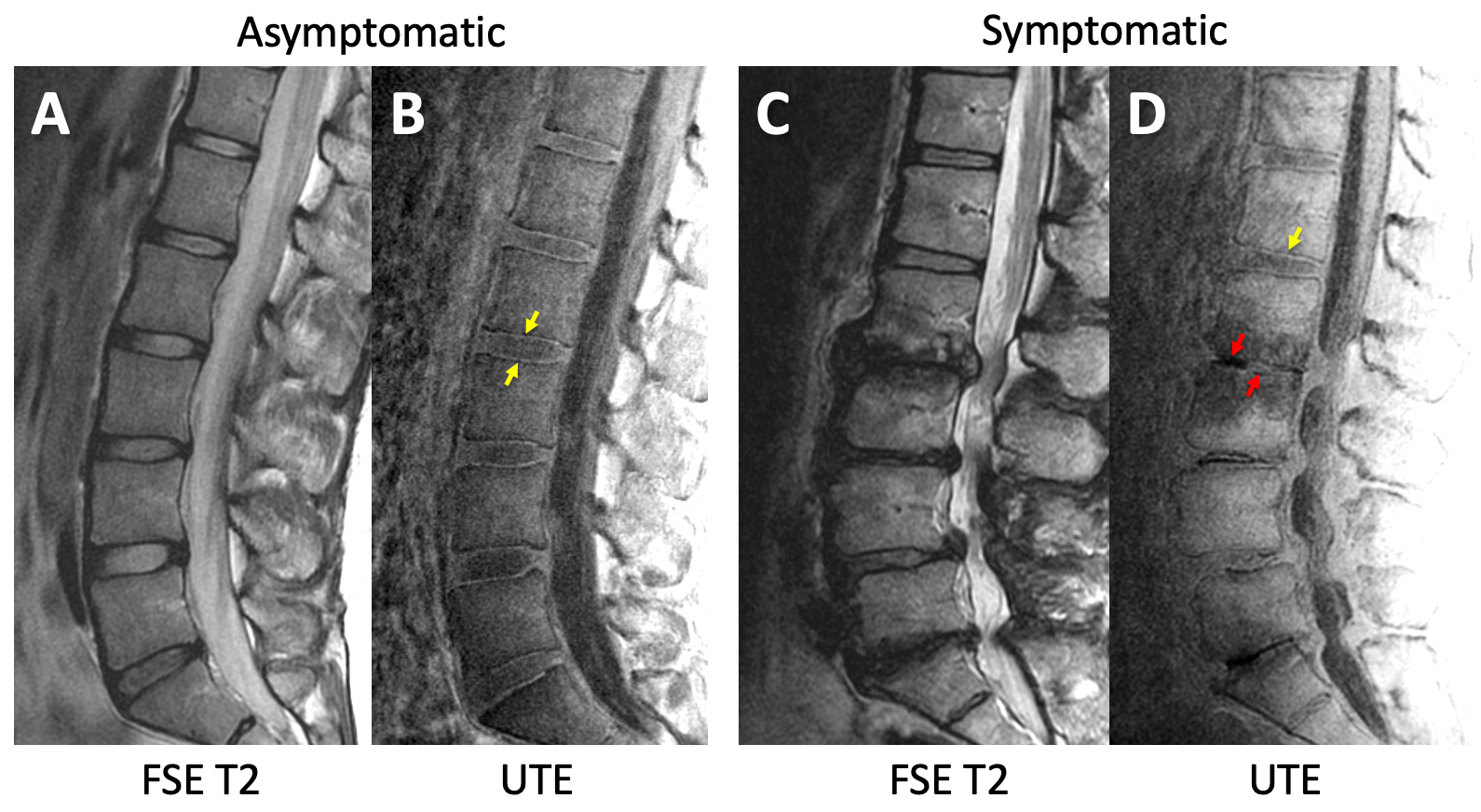
MR Appearances: Unlike to FSE T2 images that depicted DVJ with low signal intensity (Figure 3AC), UTE images showed distinct lines of high signal intensity at the DVJ in the majority of the discs (Figure 3BD, yellow arrows), which became irregular or lost in many of Sx spines (Figure 3D, red arrows). In addition to DVJ, UTE appearance of the vertebral body with Modic change was quite different from FSE T2 but this needs further investigation.Asx vs. Sx: In general, Asx subjects had IVDs and DVJs with lower grades, as shown representatively in Figure 3. While the older age of Sx subjects (p<0.01) certain contributed, in the total of 243 IVDs and 480 DVJs evaluated, we found a large difference in the distribution of IVD and DVJ (Table 1). Sx subjects had much greater proportion (chi-square p<0.0001) of abnormal DVJ (45%, combining focal loss and irregular DVJs) compared to Asx (6%). Likewise, Sx had greater proportion (p<0.0001) of discs with grades 3 or higher (45%) compared to Asx (11%). In Sx subjects, abnormal DVJs was found with slightly greater frequency at the lower lumbar levels (L3i and lower) but this was not statistically significant.
CONCLUSION
These results demonstrate the feasibility of UTE imaging of the lumbar spine to evaluate pathology of the DVJ. We found a strong association between chronic low back pain and DVJ abnormality as well as disc degeneration. One large limitation of this study is the unbalanced age of the two groups; in our recent cadaveric study,4 we found that only ~10% of the DVJ had abnormal morphology in donors <40 years of age. This increased to ~35% in age group 50-59. Another consideration is the meaning of various abnormal DVJ morphologies. We have shown5 that physical removal of uncalcified and calcified cartilaginous endplates results in a loss of signal at the DVJ. But it is unclear what other change can lead to a loss of signal intensity or irregularity.Acknowledgements
Research reported in this publication was supported in part by a research grant from National Institute of Health (R01 AR066622 and P30 AR073761) in support of Dr. Bae. The content is solely the responsibility of the authors and does not necessarily represent the official views of the sponsoring institutions.References
1. An HS, Anderson PA, Haughton VM, Iatridis JC, Kang JD, Lotz JC, Natarajan RN, Oegema TR, Jr., Roughley P, Setton LA, Urban JP, Videman T, Andersson GB, Weinstein JN. Introduction: disc degeneration: summary. Spine29: 2677-2678, 2004.
2. Abu-Ghanem S, Ohana N, Abu-Ghanem Y, Kittani M, Shelef I. Acute schmorl node in dorsal spine: an unusual cause of a sudden onset of severe back pain in a young female. Asian Spine J 7: 131-135, 2013. PMCID:3669699
3. Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine 26: 1873-1878, 2001.
4. Finkenstaedt T, Siriwananrangsun P, Masuda K, Bydder GM, Chen KC, Bae WC. Ultrashort time-to-echo MR morphology of cartilaginous endplate correlates with disc degeneration in the lumbar spine. Eur Spine J 32: 2358-2367, 2023.
5. Bae WC, Statum S, Zhang Z, Yamaguchi T, Wolfson T, Gamst AC, Du J, Bydder GM, Masuda K, Chung CB. Morphology of the Cartilaginous Endplates in Human Intervertebral Disks with Ultrashort Echo Time MR Imaging. Radiology 266: 564-574, 2013. PMCID:3558871
Figures