1543
Improving the assessment of myotendinous injuries on professional athletes using Ultrasound-MRI fusion exploration1Medical Department of Futbol Club Barcelona (FIFA Medical Center of Excellence), Barcelona, Spain, 2Department of Radiology, Hospital de Barcelona, SCIAS, Barcelona, Spain, 3Canon Medical Systems Spain and Portugal, Barcelona, Spain, 4Canon Medical Systems Corporation, Tochigi, Japan, 5Canon Medical Systems Europe, Amstelveen, Netherlands
Synopsis
Keywords: Tendon/Ligament, Multimodal, Ultrasound-MRI fusion, myotendinous injury, sports medicine, injury prognosis, lesion follow-up
Motivation: US-MRI fusion could provide more accurate information for muscle injury evaluation and follow-up. To date, some works were conducted in the scope of prostate pathology, but only a few focused on musculoskeletal imaging.
Goal(s): This study aimed to evaluate if US-MRI fusion would allow more detailed and precise characterization of myotendinous injuries.
Approach: US only and US-MRI fusion images were reviewed and scored in terms of muscle injury detection, as well as scar, tendon and edema visualization.
Results: US-MRI fusion allowed a better characterization of lesions and healing process on professional athletes suffering from myotendinous injuries compared to US alone.
Impact: Diagnosis of muscle injuries by US is a challenge, so MRI is still the gold standard in most cases. Combining both techniques, we can better characterize and follow-up lesions, detecting a slowdown in healing or complications as soon as possible.
Introduction
Ultrasound (US) and magnetic resonance imaging (MRI) are the two main imaging techniques to evaluate myotendinous pathology1. Advances in technologies such as hardware (e.g. transducers) and software allow the visualization of the muscle architecture at an in-plane resolution of less than 200 µm 2. US presents some advantages compared to MRI: it allows dynamic exploration, it is fast, cheaper, and allows real-time intervention guidance2,3. However, MRI remains the gold standard for muscle injuries4,5 , given its ability to correctly detect the injured histoarchitecture6,7, and its potential to analyze deep muscle structures8. Deep understanding of the injured histoarchitecture is essential to assess the prognosis of an injury5,7, but the images can also be used to monitor the scar, to detect healing complications as soon as possible9 and to evaluate the best return to competition period9,10. US-MRI fusion allows muscle injury assessment with additional information and more precision1. Several works have been carried out on US-MR fusion mainly around prostate pathology. However, in the field of musculoskeletal (MSK) imaging, only few works highlighted the benefits of this technique in muscle injury1. Therefore, the aim of this study was to compare US only and US-MRI fusion images at different time points of the healing process, to evaluate if US-MRI fusion allows additional information and/or precision in the context of myotendinous injuries assessment.Methods
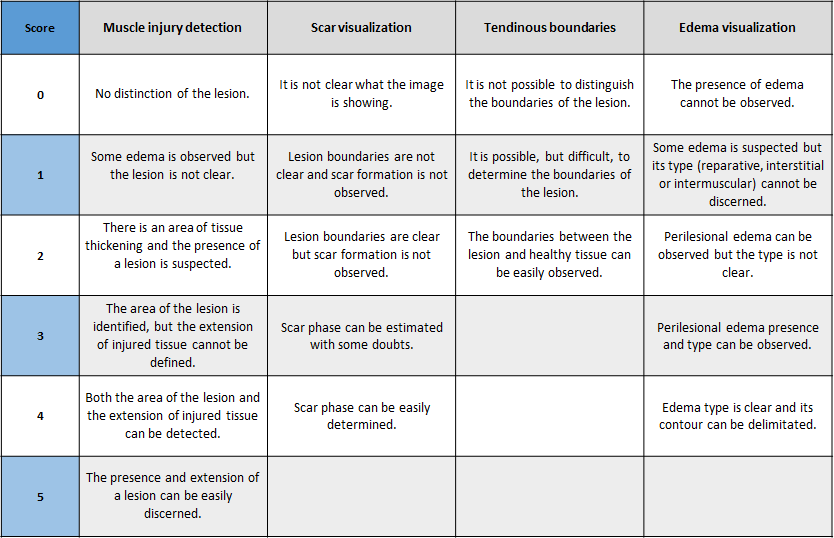
10 professional athletes from various sports (soccer, hockey and handball) with acute myotendinous injury (hamstring and rectus femoris injuries) were included in this study. They were explored the same day with a Vantage Galan 3T MRI system (Canon Medical Systems, Tochigi, Japan) and an Aplio i800 US system (Canon Medical Systems, Tochigi, Japan). All subjects underwent baseline scans at less than two weeks post-diagnosis (excepting by one scanned at three weeks and a half) and half of them underwent a follow-up scan at between one week and a half and three weeks post-baseline. MRI explorations included a 3D FSE T2-weighted FS scan, with an isotropic 0.7 mm resolution and a scan time of 15 minutes and 20 seconds, using an Atlas SPEEDER body coil. A strap on the feet was used to fix the limbs and to standardize the athlete’s position. MRI images were processed with the fusion software of the US equipment, and muscle injuries were explored performing the US. The athlete’s position during the MRI exploration was reproduced during the US examination. All the images were randomly evaluated by two experienced sports physicians and one experienced MSK radiologist in terms of muscle injury detection, as well as scar, tendinous boundaries of the lesion, and edema visualization. The scoring criteria used by the observers is described in Table 1. A paired T-test was used for the statistical analysis. Values of p<0.05 were considered statistically significant.Results and Discussion
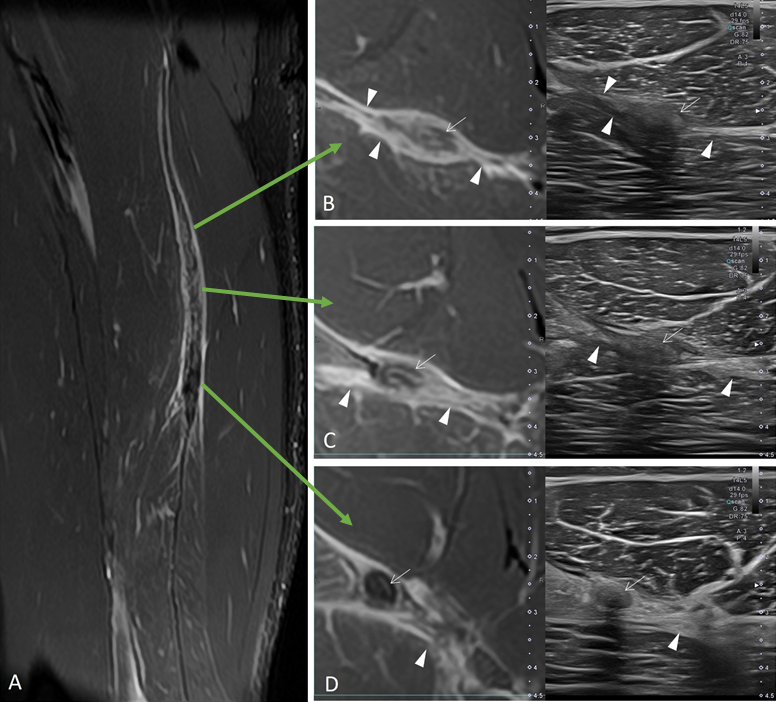
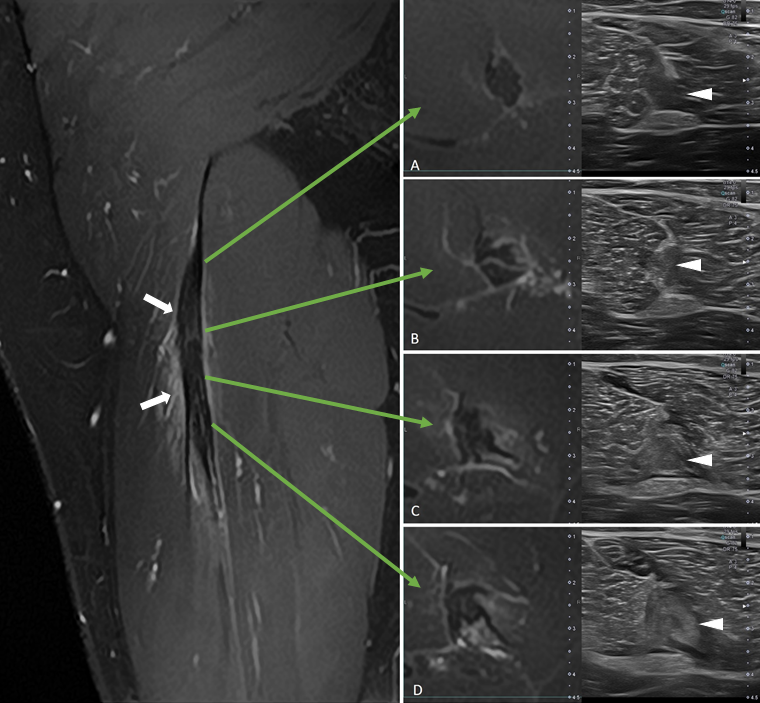
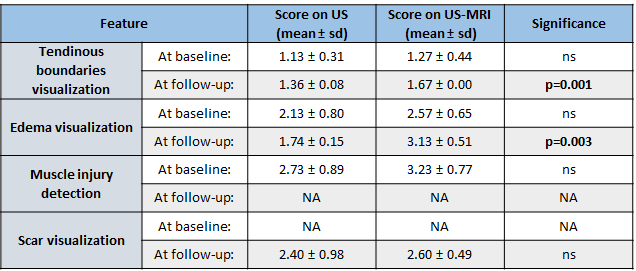
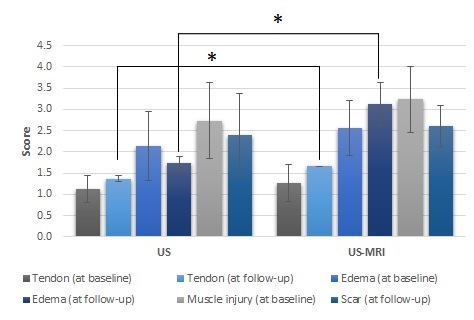
The exploration with US-MRI fusion images allowed the assessment of the healing process for each injury, as illustrated in Figure 1 and 2. The resulting scores from the qualitative evaluation are reported in Table 2. These scoring criteria include important variables in terms of prognosis and return-to-play assessment. Tendon injuries are more clearly characterized using US-MRI fusion, allowing a better understanding of the injury and increased knowledge on scar progression during follow-up. As seen in Figure 1, independent of the time point, all the features were scored higher when US-MRI fusion images were considered for the evaluation. However, the increase was statistically significant only at the follow-up exam, for tendinous boundaries and edema visualization scores. This could reflect an improved understanding of the injury and its healing process, which is consistent with a previous work1. Nevertheless, larger cohorts of athletes and multiple time points should be analyzed for determining the potential of US-MRI fusion in the assessment of sports-related injuries. The absence of significant differences between modalities at baseline could be due to the higher standard deviations observed at this time point, which might reflect the complexity of qualitatively evaluating those features at early phases of the healing process. In addition, further research would be needed for improving the assessment of mild injuries using US-MRI fusion, since most of them are identified on MRI but not seen on US.Conclusion
The fusion of MRI images during the US exploration allowed a better visualization of structures and a better characterization of lesions on professional athletes suffering from myotendinous injuries. Likewise, it seems to provide a better analysis of the healing process or of the scar. Future works will evaluate if new biomarkers could be proposed to determine the optimal return-to-play period without risk of re-injury.Acknowledgements
The authors sincerely thank to all FC Barcelona players and staff involved in the data collection process.References
1. Wong-On M, Til-Pérez Ll, Balius R. Evaluation of MRI-US fusion technology in Sports-Related Musculoskeletal Injuries. Adv Ther. 2015; 32:580-594.
2. Guermazi A, Roemer FW, Robinson P, Tol JL, Regatte RR, Crema MD. Imaging of muscle injuries in Sports Medicine: Sports Imagins Series. Radiology 2017; 285(3):1063.
3. Kerkhoffs GM, van ES N, Wieldraaijer T, Sierevelt IN Ekstrand J, Van Dijk CN. Diagnosis and prognosis of acute hamstring injuries in athletes. Knee Surg Sports Traumatol Arthrosc. 2013; 21(2):500-509
4. Costa AF, Di Primio GA, Schweitzer ME. Magnetic resonance imaging of muscle disease: a pattern-based approach. Muscle Nerve. 2012; 46:465–81. doi:10.1002/mus.23370
5. Kumaravel M, Bawa P, Murai N, Magnetic resonance imaging of muscle injury in elite American football players: predictors for return to play and performance, European Journal of Radiology 2018; 108:155-164. doi: 10.1016/j.ejrad.2018.09.028.
6. Balius R, Alomar X, Pedret C et al. Role of the Extracellular Matrix in Muscle injuries. The Orthopaedic Journal of Sports Medicine, 6(9), 2325967118795863 DOI: 10.1177/2325967118795863
7. Study Group of the Muscle and Tendon System from the Spanish Society of Sports Traumatology, Balius R, Blasi M. The Orthopaedic Journal of Sports Medicine, 8(3), 2325967120909090 DOI: 10.1177/2325967120909090
8. Balius R, Rodas G, Pedret C, Capdevila L, Alomar X, Bong D. Soleus muscle injury: sensitivity of ultrasound patterns. Skeletal Radiol. 2014; 43: 805–12.
9. Baldock J, Wright S, McNally E, et al. Intratendinous hamstring injuries: sequential MRIs as a tool to reduce the risk of reinjury in elite sport. BMJ Case Rep 2021; 14:e241365.
10. Isern-Kebschull J, Pedret C, Mechó S et al. 2022 MRI findings prior to return to play as predictors of reinjury in professional athletes: a novel decision-making tool. Insights Into Imaging 2022; 13:203.
Figures