1527
Multi-B-Values-Fitting RESOLVE DWI in Evaluation of Disease Activity and Curative Effect of Axial Spondyloarthritis (axSpA)1Shengli Clinical Medical College of Fujian Medical University; Radiology department of Fujian Provincial Hospital, Fuzhou, China, 2Radiology department of Fuzhou Second Hospital, Fuzhou, China, 3Shengli Clinical Medical College of Fujian Medical University; Rheumatism department of Fujian Provincial Hospital, Fuzhou, China, 4MR Research Collaboration Team, Siemens Healthineers Ltd., Shanghai, China
Synopsis
Keywords: Bone, Diffusion/other diffusion imaging techniques, RESOLVE DWI; multi-b-values-fitting; axial spondyloarthritis; quantitative; tumour necrosis factor inhibitors
Motivation: Methods to quantitatively assess disease activity and efficacy of axSpA are still being explored.
Goal(s): To find a reliable quantitative indicator for evaluating disease activity and curative effect of axSpA, using multi-b-values-fitting RESOLVE DWI.
Approach: By comparing the ADC values calculated by fitting different b values between different groups, a relatively reliable b-values-fitting sequence was obtained, further evaluating curative effect of the treatment group in different cycles.
Results: Multi-b-values-fitting (b=50,500,700s/mm2) RESOLVE DWI has a certain advantage in evaluating disease activity and efficacy of axSpA, but the effect of short-term review (3 weeks or less) is unsatisfactory.
Impact: Multi-b-Values-Fitting RESOLVE DWI can differentiate the severity of axSpA disease activity more intuitively, by measuring the ADC values of bone marrow edema of sacroiliac joints, providing a new idea for clinical search for more objective and accurate quantitative parameters.
Introduction
AxSpA is a chronic systemic autoimmune disease involving sacroiliac joints (SIJs) with long course, poor prognosis 1. Several studies highlighted the inflammatory response, caused by inflammatory cells and factors, played a vital role in the occurrence and development of axSpA 2. The process of inflammatory reaction caused by inflammatory cells can be characterized by the formation of local bone marrow edema (BME). In 2009, Assessment of Spondyloarthritis international Society (ASAS) proposed that imaging changes of active inflammation of SIJs play an important role in the diagnosis of axSpA, especially MRI 3. In 2019, ASAS updated consensus definitions for MRI lesions of SIJs 4.Conventional DWI, a functional MRI technique to non-invasively evaluate the random motion of water molecules by measuring ADC values , is vulnerable to geometric distortion, T2*-induced blurring, and susceptibility artifacts. RESOLVE-DWI has been suggested as an alternative approach to overcome the limitations, whose core is that the k-space is divided into several segments along the direction of the readout 5. However, there were few reports on the application of RESOLVE DWI in the SIJs, and even fewer on the multiple b-values fitting.The clinical treatment decision of axSpA patients depends on the disease activity, widely evaluated by ASDAS score, a comprehensive assessment of clinical symptoms and laboratory data 6. At present, it’s recommended for patients with high activity (ASDAS≥2.1) to reducing disease activity by comprehensive treatment, including tumour necrosis factor inhibitors (TNFi) 7. ASAS/EULAR, jointly developed by axSpA guidelines in 2016, recommended that patients with continuous relief of inflammation should be considered for reducing TNFi 8. Although the ASDAS score is widely accepted in assessing disease activity of axSpA and clinical monitoring the curative effect of axSpA, it is affected by subjective factors of the patients, which may cause some bias.
In this study, multi-b-values fitting RESOLVE DWI was used in the examination of SIJs in each group to discuss the value of distinguishing axSpA disease activity and evaluating curative effect of axSpA.
Methods
This study collected 89 axSpA patients (axSpA group, mean age 32.0, 54 male) and 17 controls (no-axSpA group, mean age 39.0, 10 male). The axSpA group was classified into active (n=60) and inactive (n=29) groups based on ASDAS-CRP. The axSpA group was defined as patients who met the 2019 ASAS criteria for axSpA and had complete clinical and MRI data. The no-axSpA group met the following criteria: (a) patients who underwent SIJs MRI examination due to chronic lower back pain and (b) absence of positive signs in the subchondral bone marrow of bilateral SIJs in fat suppression proton density weighted imaging (PDWI-fs). All participants underwent SIJs MRI scans, including RESOLVE DWI, using a 1.5T MRI scanner (MAGNETOM Aera, SIEMENS Healthcare, Erlangen, Germany). RESOLVE DWI(b=50,500s/mm2) parameters were: TR/TE=4760/78138ms, FOV=240×240mm, scan matrix=100×100mm, slice thickness=3mm, scanning time 6min 38s. RESOLVE DWI(b=50,700s/mm2) parameters were: TR/TE=4830/80140ms, scanning time 6min 41s. RESOLVE DWI(b=50,500,700s/mm2) parameters were: TR/TE=4890/82144ms, scanning time 8min 58s. All MRI examination images of the participants were evaluated by two trained raters, who independently manually delineated regions of interest (ROIs). For data analysis, The Kruskal-Wallis test was used to compare the difference of ADC values obtained by fitting with different b values between each group. The ROC curve was used to evaluate the diagnostic efficiency of ADC values between each group. The Friedman test was used to compare the ADC values and ASDAS-CRP in the treatment group in different cycles (before treatment, 3 weeks, 6 weeks and 12 weeks after treatment).Results
The ADC values of SIJs in the axSpA group, inactive group and active group were all higher than those in the no-axSpA group (P<0.05). The ADC values of SIJs in the active group were all higher than those in the inactive group (P<0.05) (Fig. 1,2). ADC50,500,700 had the largest AUC, relative higher sensitivity and specificity while taking account of the image quality than ADC50,700 and ADC50,500 between different groups. In the treatment group, there was no significant difference in ADC values between pre-treatment and 3 weeks, 3 weeks and 6 weeks, 6 weeks and 12 weeks, while the decreased ADC values in the interval of 6 weeks or more were statistically significant (Fig. 2,3).Discussion & Conclusions
Multi-b-values-fitting (b=50,500,700s/mm2) RESOLVE DWI has a certain advantage in evaluating disease activity of axSpA. It was worth noting that short-term review (3 weeks or less) of RESOLVE DWI was unsatisfactory and review at 6 weeks or later would help to evaluate curative effect of axSpA.Acknowledgements
The authors wish to thank Ruobei Luo, Wei Zhang, Yijun Dai for the data collection, Shengmei Lin and Jiawei Su for technician, nurse Fang Huang for helping with the MR examination, and Fayang Lian, working in the hospital scientific research department, for providing scientific advice.References
1 Robinson PC, van der Linden S, Khan MA, et al. Axial spondyloarthritis: concept, construct, classification and implications for therapy. Nat Rev Rheumatol (2021) 17:109–118.
2 Wang DM, Lin L, Peng JH, et al. Pannus inflammation in sacroiliitis following immune pathological injury and radiological structural damage: a study of 193 patients with spondyloarthritis. Arthritis Res Ther (2018) 20:120.
3 Rudwaleit M, van der Heijde D, Landewé R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis (2009) 68:777–783.
4 Maksymowych WP, Lambert RG, Østergaard M, et al. MRI lesions in the sacroiliac joints of patients with spondyloarthritis: an update of definitions and validation by the ASAS MRI working group. Ann Rheum Dis (2019) 78:1550–1558.
5 Zhang H, Huang H, Zhang Y, Tu Z, et al. Diffusion-Weighted MRI to Assess Sacroiliitis: Improved Image Quality and Diagnostic Performance of Readout-Segmented Echo-Planar Imaging (EPI) Over Conventional Single-Shot EPI. AJR Am J Roentgenol (2021) 217:450–459.
6 Machado P, Landewé R, Lie E, et al. Assessment of SpondyloArthritis international Society. Ankylosing Spondylitis Disease Activity Score (ASDAS): defining cut-off values for disease activity states and improvement scores. Ann Rheum Dis (2011) 70:47–53.
7 Molnar C, Scherer A, Baraliakos X, et al. TNF blockers inhibit spinal radiographic progression in ankylosing spondylitis by reducing disease activity: results from the Swiss Clinical Quality Management cohort. Ann Rheum Dis (2018) 77:63–69.
8 van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis (2017) 76:978–991.
Figures
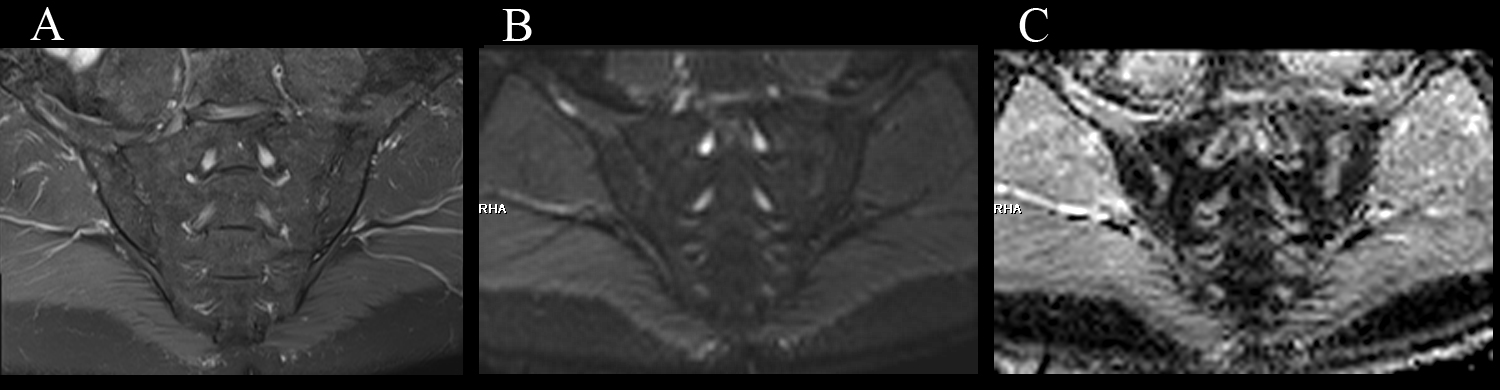
Fig.1, male, 61 years old, HLA-B27: +, CRP:2.85mg/L ASDAS-CRP:0.9, belonged to the inactive group. (A, B) The coronal plane of PDWI-fs and RESOLVE DWI (b=50,500,700s/mm2) did not show significant high signal intensity in subchondral bone marrow area of the SIJs. (C) The ADC maps (b=50,500,700s/mm2) showed the ADC values in bilateral SIJs were 0.593×10-3 mm2/s (iliac) and 0.723×10-3 mm2/s (sacral), respectively.
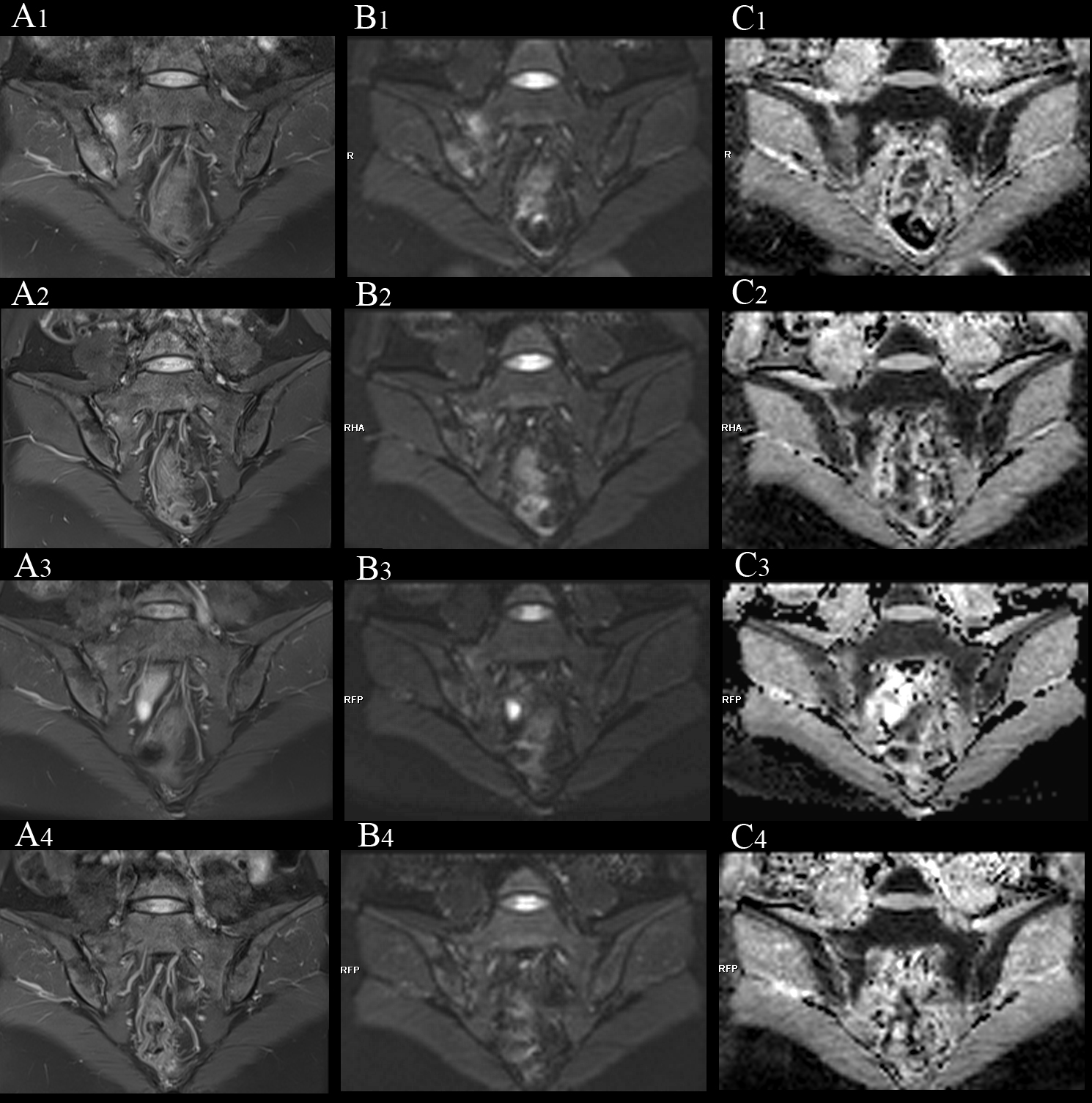
Fig. 2, female, 33 years old, HLA-B27: +, CRP:21.7mg/L, ASDAS-CRP:3.4, belonged to active group and treatment group; (A(1-4)-C(1-4)) showed the same patient before treatment and 3 weeks, 6 weeks and 12 weeks after treatment. (A, B) showed the coronal plane of PDWI-fs and RESOLVE DWI (b=50,500,700s/mm2); (C) showed the ADC maps. After treatment, the ASDAS-CRP score decreased (3.4, 0.6, 0.6, 0.6). (A(1-4), B(1-4)) showed the signal intensity in right SIJs decreased, gradually; (C(1-4)) showed the ADC values in the lesion decreased, gradually (1.483, 1.327, 1.027, 0.831×10-3 mm2/s).
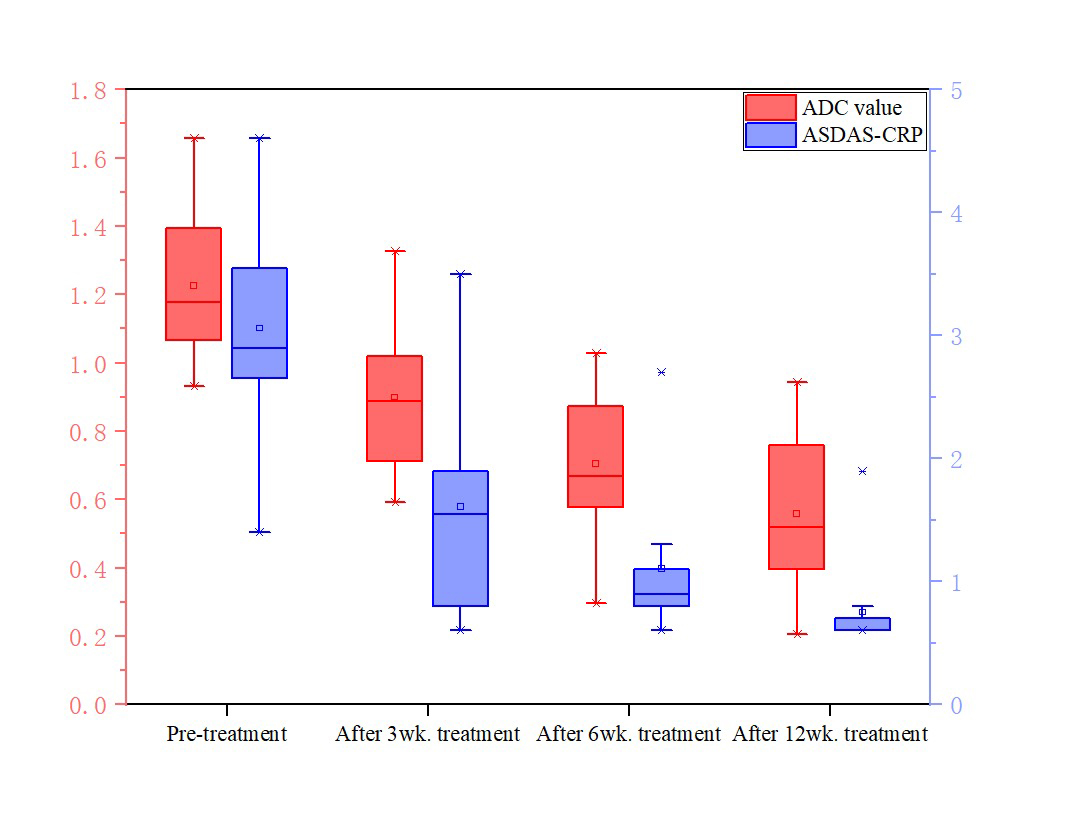
Fig. 3, Changes in ADC values and ASDAS-CRP in the treatment group. The values of ADC and ASDAS-CRP in the treatment group decreased synchronously with the treatment period.