1518
Long-T2 Suppressed ZTE with subspace reconstruction for bone imaging1Department of Neuroimaging, Institute of Psychiatry Psychology and Neuroscience, King's College London, London, United Kingdom
Synopsis
Keywords: Bone, Bone, ZTE long-T2 subspace
Motivation: Recent work has shown that achieving CT-like contrast highlighting bone can be obtained either indirectly through contrast inversion or directly through long-T2 suppression. While direct methods offer advantages, existing techniques are inefficient, resulting in long scan times.
Goal(s): To create an efficient long-T2 suppressed bone imaging MR scan.
Approach: We combined inversion recovery long-T2 suppression in a Zero Echo-Time sequence with subspace reconstruction to allow continuous data collection during the scan, eliminating dead time and improving efficiency.
Results: A two minute silent scan that produces bright bone and suppressed soft tissues
Impact: We have created a fast positive contrast bone MRI scan that has potential as an alternative to CT
Introduction
MRI is commonly seen as a soft tissue imaging method, with CT being the go-to for visualising hard tissues such as bone. However, recent studies challenge this belief, demonstrating that MRI can produce diagnostically useful images of bone 1. Various techniques are currently employed for this purpose, such as contrast inversion of "black bone" gradient-echo or Zero Echo-Time (ZTE) images 2 and long-T2 suppression via either dual-echo subtraction or inversion/saturation recovery 3,4.Contrast inversion methods generally use Proton-Density weighted images. These have the advantage of fast scans, but have the drawback that upon simple inversion background regions become bright and hence due to partial volume affects tissue/air interfaces can appear with bone-like contrast. Long-T2 suppressed methods avoid this problem but generally require longer data acquisition. This is particularly acute for inversion/saturation recovery ZTE, where previously acquisition can only occur in a short window where the correct contrast is obtained 3.
We eliminated this drawback to long-T2 suppressed ZTE by instead acquiring data throughout the transient following an inversion pulse, and then using physics-based subspace reconstruction 5 to produce a high SNR image of the desired positive bone contrast.
Method
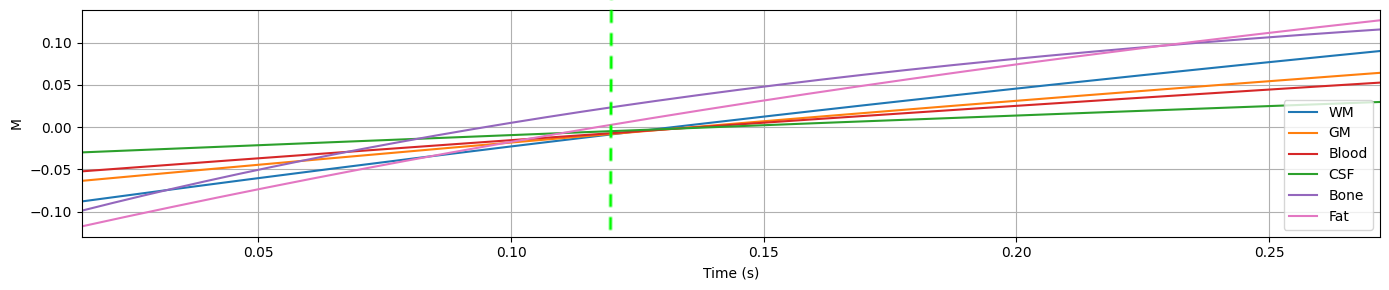
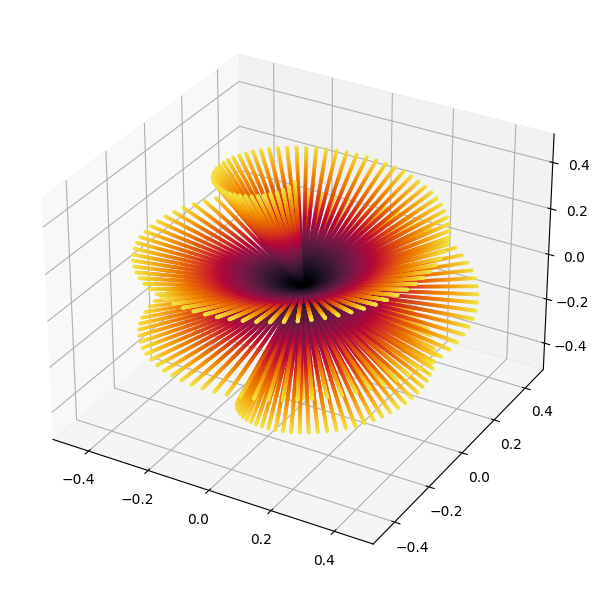
We first developed a simulation framework for segmented, magnetization-prepared sequences using homogenized Bloch equations and an eigenanalysis to find the steady state6. We used this to simulate an Inversion Recovery ZTE sequence3 where readouts occur for the whole period between inversion pulses. The simulated tissues were White Matter, Grey Matter, Blood, CSF, Bone, and Fat with T1s of 1.0, 1.6, 1.95, 4.3, 0.2, 0.4 and relative Proton Densities of 0.7, 0.8, 0.8, 1.0, 0.2, 0.4 respectively. We then optimized the sequence parameters to maximize the positive contrast for bone. The final simulation is shown in Figure 1.A healthy volunteer was scanned with this sequence in a 3T magnet equipped with a 48 channel head coil (GE Premier). The sequence parameters were readout bandwidth ±41kHz, 250 spokes per segment, 220mm FOV, 1mm isotropic voxel size, flip angle 2°, scan-time 2 minutes. The trajectory within a segment was a spiral phyllotaxis7, which was rotated by 2D golden means8 between segments (Figure 2) to produce an overall incoherent trajectory. Low-resolution segments were acquired with the gradients ramped down by a factor of 8 to fill the dead-time gap9.
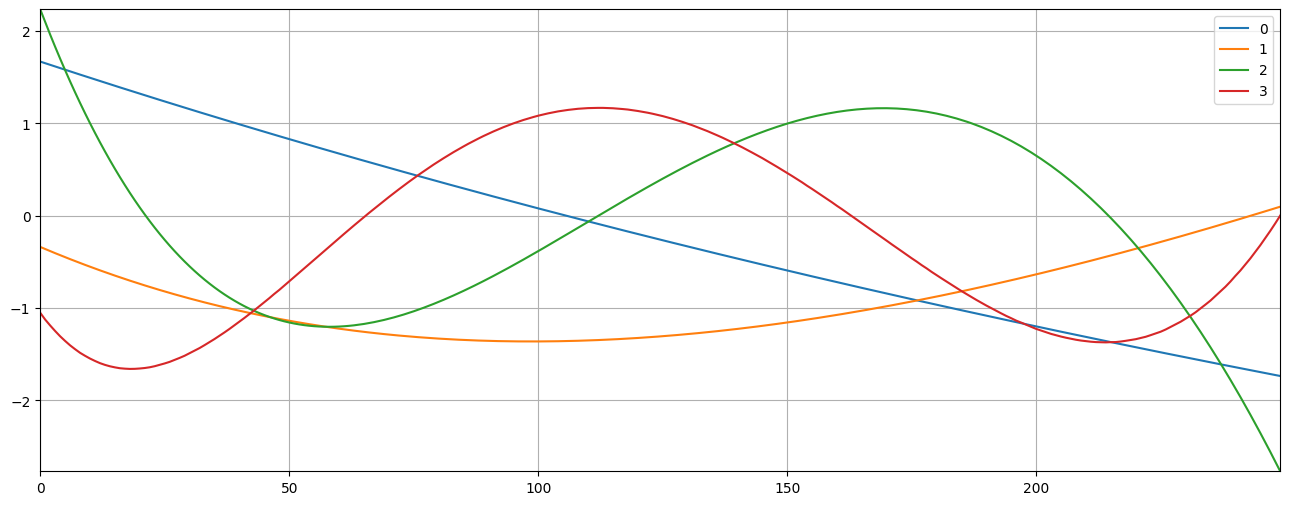
The data was reconstructed with the RIESLING toolbox10. To construct the subspace basis vectors, the evolution of 128 samples from each of the above tissue types with T1 ranges of 0.30-0.50, 0.80-1.10, 1.20-1.70, 1.30-1.80 and 3.80-4.80 was simulated using the framework, and then a Singular Value Decomposition taken. The resulting basis vectors are shown in Figure 3. Sensitivity maps were calculated directly from the data11.
Results
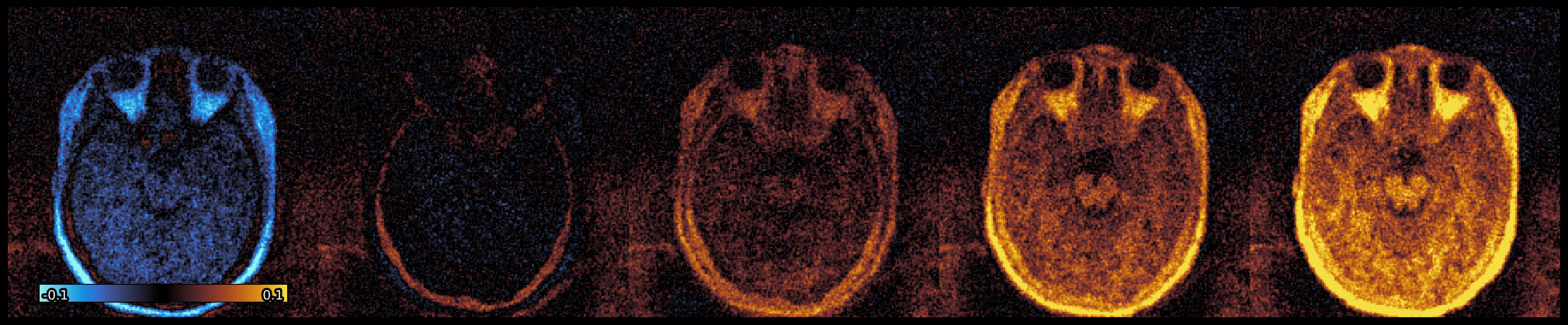
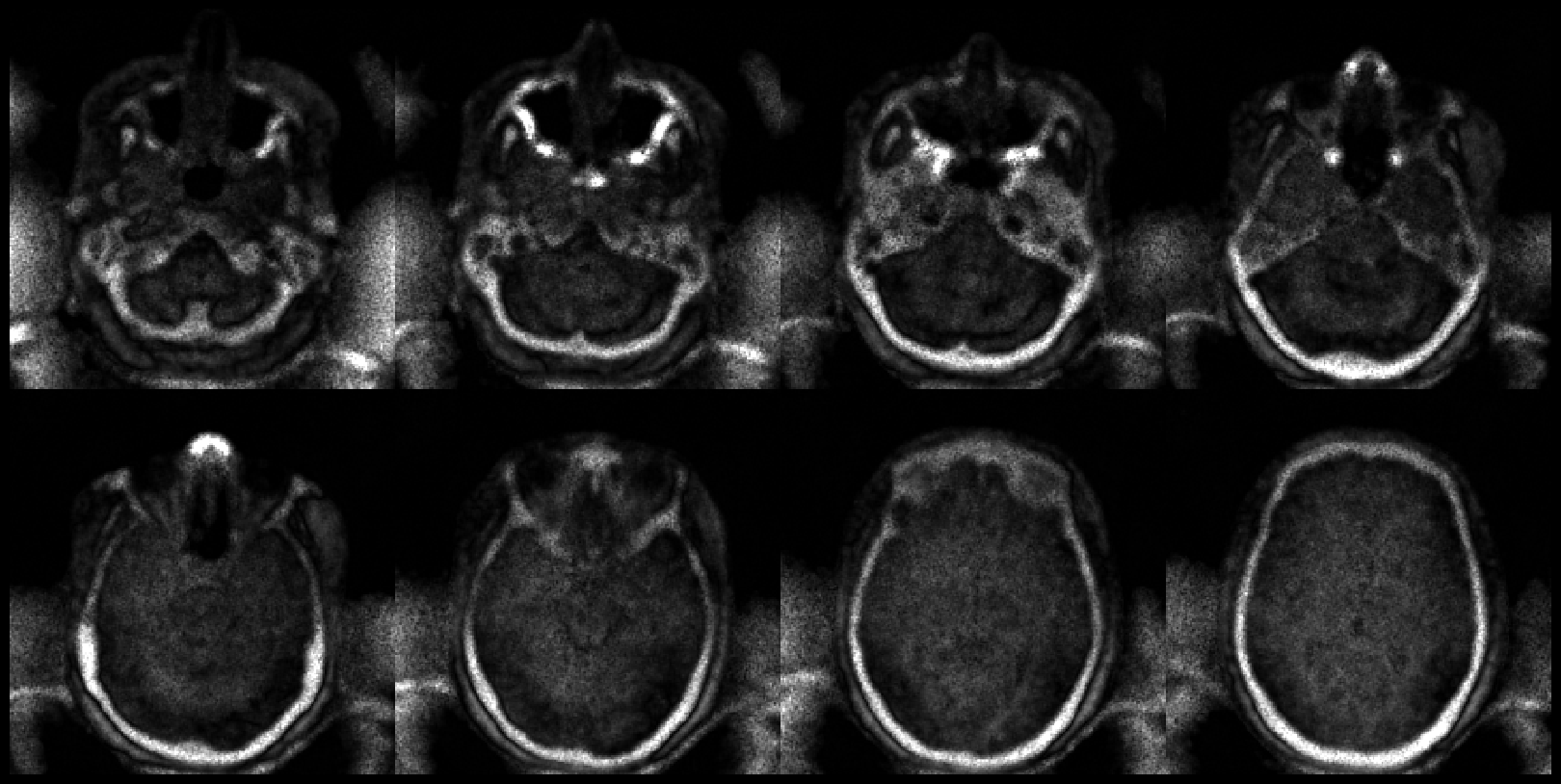
Figure 4 shows the real-valued reconstructed at time-points 25, 75, 125, 175 (spokes within segment) after the inversion pulse. The expected pattern of longitudinal recovery can be observed, particularly in bone with the shortest T1. Figure 5 shows multiple slices through time-point T=72, chosen to maximize positive bone contrast while minimizing the signal from soft tissues including fat. The cortical bone can clearly be seen, and importantly both tissue and air show low to no signal.Discussion and Conclusion
We have eliminated a significant drawback of the inversion recovery long-T2 suppression technique – namely that the desired contrast exists for only a small proportion of the overall imaging time. By accurately modelling the magnetization evolution and incorporating this physics knowledge into the reconstruction, we were able to acquire data almost continuously, significantly shortening the overall scan time while maintaining high image quality.Acknowledgements
No acknowledgement found.References
1. F. Wiesinger and M.-L. Ho, ‘Zero-TE MRI: principles and applications in the head and neck’, BJR, p. 20220059, Jun. 2022, doi: 10.1259/bjr.20220059.
2. F. Wiesinger et al., ‘Zero TE-based pseudo-CT image conversion in the head and its application in PET/MR attenuation correction and MR-guided radiation therapy planning’, Magnetic Resonance in Medicine, vol. 80, no. 4, pp. 1440–1451, Oct. 2018, doi: 10.1002/mrm.27134.
3. M. Weiger et al., ‘ZTE imaging with long-T2 suppression’, NMR Biomed., vol. 28, no. 2, pp. 247–254, Feb. 2015, doi: 10.1002/nbm.3246.
4. M. Weiger and K. P. Pruessmann, ‘Short-T2 MRI: Principles and recent advances’, Progress in Nuclear Magnetic Resonance Spectroscopy, vol. 114–115, pp. 237–270, Oct. 2019, doi: 10.1016/j.pnmrs.2019.07.001.
5. X. Wang, Z. Tan, N. Scholand, V. Roeloffs, and M. Uecker, ‘Physics-based reconstruction methods for magnetic resonance imaging’, Phil. Trans. R. Soc. A., vol. 379, no. 2200, p. 20200196, Jun. 2021, doi: 10.1098/rsta.2020.0196.
6. S. J. Malik, R. P. A. G. Teixeira, D. J. West, T. C. Wood, and J. V. Hajnal, ‘Steady‐state imaging with inhomogeneous magnetization transfer contrast using multiband radiofrequency pulses’, Magnetic Resonance in Medicine, Sep. 2019, doi: 10.1002/mrm.27984.
7. E. Ljungberg, T. C. Wood, A. B. Solana, S. C. R. Williams, G. J. Barker, and F. Wiesinger, ‘Motion corrected silent ZTE neuroimaging’, Magnetic Resonance in Med, p. mrm.29201, Apr. 2022, doi: 10.1002/mrm.29201.
8. R. W. Chan, E. A. Ramsay, C. H. Cunningham, and D. B. Plewes, ‘Temporal stability of adaptive 3D radial MRI using multidimensional golden means’, Magn. Reson. Med., vol. 61, no. 2, pp. 354–363, Feb. 2009, doi: 10.1002/mrm.21837.
9. Y. Wu et al., ‘Water- and fat-suppressed proton projection MRI (WASPI) of rat femur bone’, Magnetic Resonance in Medicine, vol. 57, no. 3, pp. 554–567, Mar. 2007, doi: 10.1002/mrm.21174.
10. T. Wood, E. Ljungberg, and F. Wiesinger, ‘Radial Interstices Enable Speedy Low-volume Imaging’, JOSS, vol. 6, no. 66, p. 3500, Oct. 2021, doi: 10.21105/joss.03500.
11. E. N. Yeh et al., ‘Inherently self-calibrating non-cartesian parallel imaging’, Magnetic Resonance in Medicine, vol. 54, no. 1, pp. 1–8, Jul. 2005, doi: 10.1002/mrm.20517.
12. [1]
Figures