1514
3 Contrasts in 3 Minutes: Rapid, High-Resolution, and CT-like Head and Neck Imaging by Dual-RF, Dual-Echo UTE1Department of Radiology, University of Pennsylvania, Philadelphia, PA, United States, 2Department of Bioengineering, University of Pennsylvania, Philadelphia, PA, United States, 3School of Electronics Engineering, Kyungpook National University, Daegu, Korea, Republic of, 4Department of Orthopaedic Surgery, University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Keywords: Bone, Head & Neck/ENT, craniosynostosis, skull, ultrashort echo time, dual-echo
Motivation: Reduction of ionizing radiation for repeat CT imaging of pediatric patients with craniosynostosis.
Goal(s): Develop an MRI method for rapid, high-resolution skull imaging with CT-like contrast.
Approach: A dual-echo UTE sequence acquires 2 image echoes (proton density-weighted and T1-weighted) in 3 minutes at a voxel size of 0.65x0.65x0.65 mm. A new joint ℓ0-wavelet regularizer and an improved method for calculating the third image with CT-like contrast are developed.
Results: In 3 minutes of scan time, 3 co-registered high-resolution images with 3 different contrasts are simultaneously acquired. Image quality is not hindered by the aggressive acceleration factor. Short-T2 specific images strongly resemble CT images.
Impact: We present a bone-specific dual-echo UTE MRI method that facilitates unimodal, single-session radiology for pediatric patients with craniosynostosis. The method does not involve ionizing radiation and may reduce the lifetime risk of cancer for patients indicated for repeat CT scans.
Introduction
Repeat CT imaging for craniofacial anomalies results in excessive ionizing radiation exposure in pediatric patients1. Patients with bony malformations can also develop intracranial soft-tissue complications where MRI is indicated for preoperative assessment2. Dual-echo ultrashort echo (UTE) methods acquire data at two echo times to produce two image contrasts. Echo subtraction creates a third image with CT-like contrast. The result is a single MRI scan for simultaneous assessment of soft-tissue and bone. Scan times are 6 minutes with voxel sizes of 1.1 mm. Furthermore, bright-bone images often have suboptimal bone specificity at the sinuses due to the presence of air3-5. This work uses parallel imaging and a joint ℓ0-wavelet regularizer to reduce the scan time to 3 minutes and the voxel size to 0.65 mm. An iterative method is presented to improve bone specificity in the CT-like image subtraction.Methods
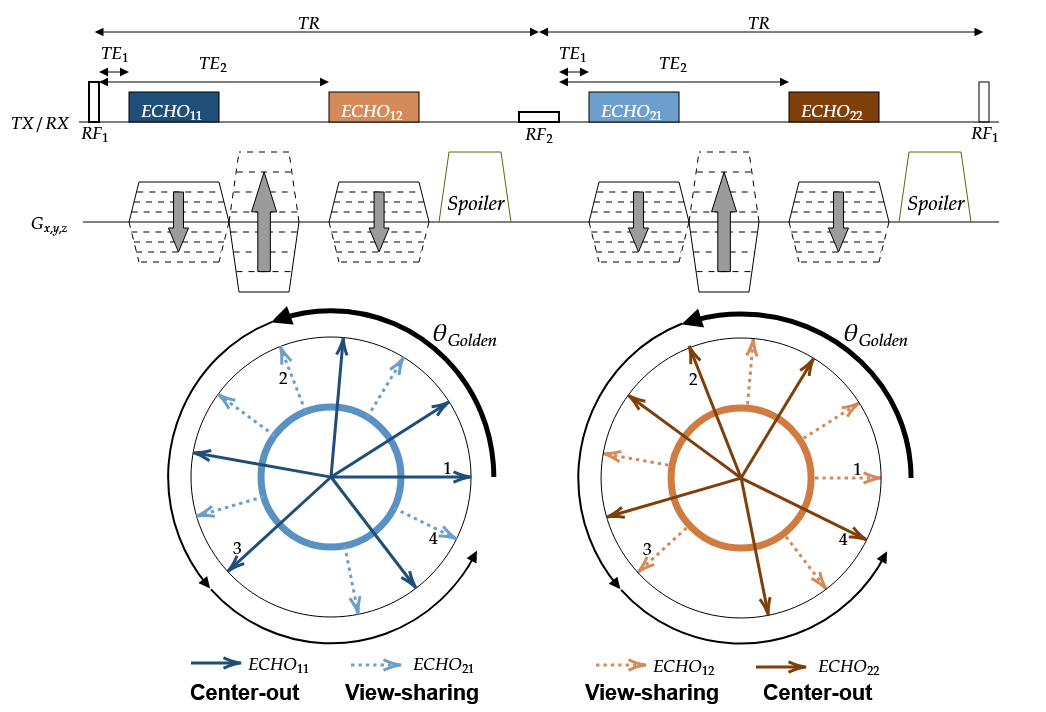
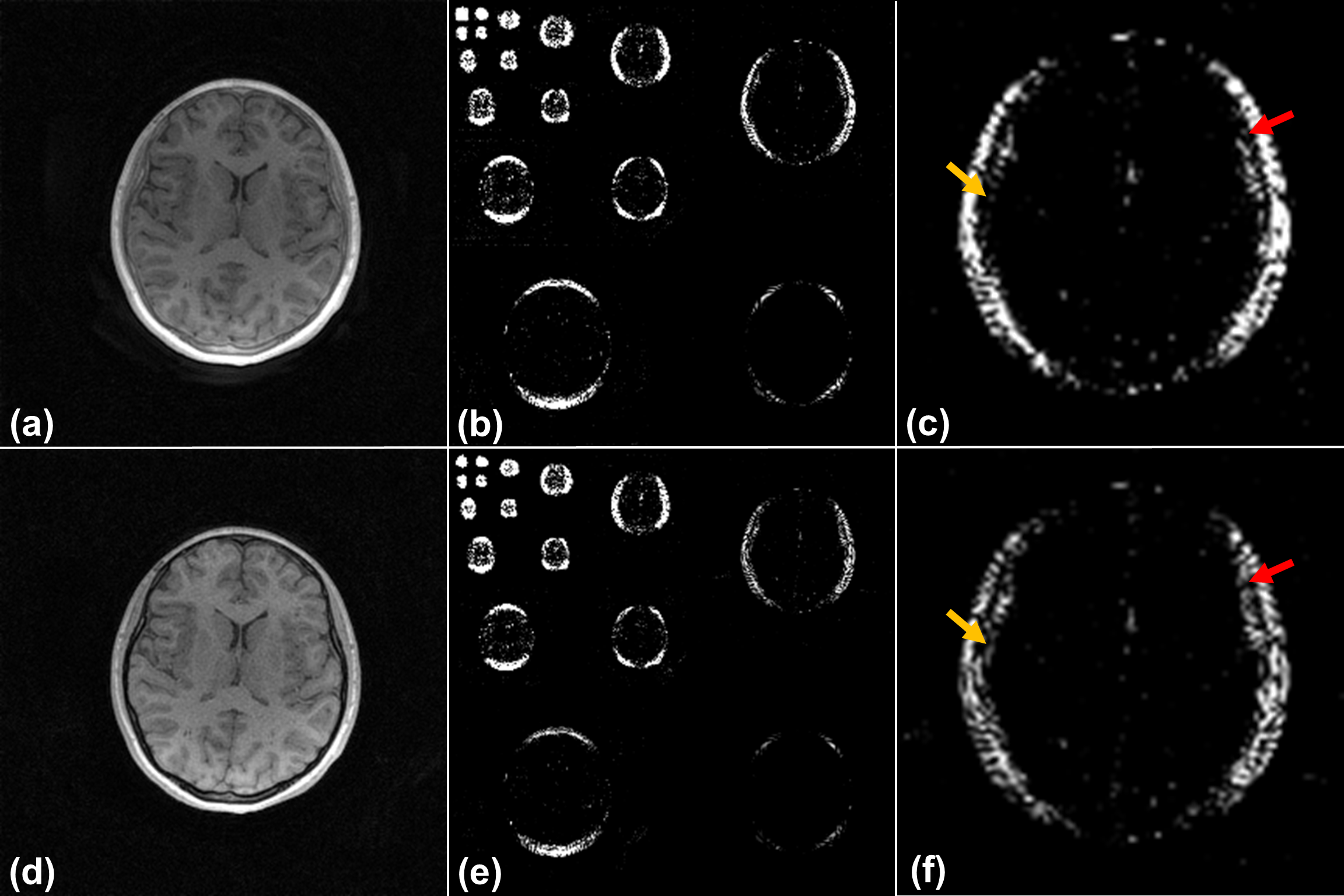
Figure 1 shows the dual-RF, dual-echo sequence used in this work. Alternating TRs with “fast” and “slow” RF pulses enhance short-T2 conspicuity3,6. Each RF is followed by two echoes which are sorted and combined in a view-sharing scheme to produce k-space datasets of two distinct contrasts. Center-out readouts are acquired in a 3D golden-angle ordering scheme to facilitate trajectory incoherence. An FOV of 280x280x280 mm and voxel size of 0.65x0.65x0.65 mm are used.Interleaved acquisition of ultrashort and conventional echoes produces two images which are perfectly registered with shared edges. Figure 2 demonstrates that the spatial positions of high-magnitude wavelet coefficients are highly correlated between both echo images. However, the T2-decay of bound water protons in the cortical bone produces new nonzero wavelet coefficients in the conventional echo image because of the generation of new image edges. To preserve edge sharpness in the echo subtraction, a joint ℓ0-wavelet regularizer is used, and its proximal operation7 on one of the image echoes $$$\boldsymbol{\nu}$$$ is computed by element-wise joint hard-thresholding with the other echo $$$\boldsymbol{x}$$$:
$$\text{prox}_{\lambda\text{JointL}_0}(\boldsymbol{\nu},\boldsymbol{x})=\begin{cases}\nu,&\sqrt{|\nu|^2+|x|^2}>\lambda\\0,&\sqrt{|\nu|^2+|x|^2}\leq\lambda\end{cases}.$$
Therefore, both echo images ultimately have the same set of nonzero wavelet coefficients. This facilitates accurate calculation of the CT-like image subtraction. Image reconstruction then minimizes:
$$\min_{\boldsymbol{x}_1,\boldsymbol{x}_2}||\boldsymbol{E}_1\boldsymbol{x}_1-\boldsymbol{y}_1||_2^2+||\boldsymbol{E}_2\boldsymbol{x}_2-\boldsymbol{y}_2||_2^2+\lambda\text{JointL}_0(\boldsymbol{x}_1,\boldsymbol{x}_2).$$
$$$\boldsymbol{E}_1$$$ and $$$\boldsymbol{E}_2$$$ are operators which encode trajectories and coil sensitivities for images $$$\boldsymbol{x}_1$$$ and $$$\boldsymbol{x}_2$$$. $$$\boldsymbol{y}_1$$$ and $$$\boldsymbol{y}_2$$$ are the acquired data for each contrast. Coil sensitivities were estimated by NLINV8 and a k-space preconditioner9 was used.
Johnson, et al. proposed a method for echo subtraction followed by a normalization step to highlight short-T2 species6. However, the normalization performs voxel-wise division that results in noise amplification at spatial positions where proton signal does not exist (e.g. air in the sinuses). This motivates the reformulation of the echo subtraction as an optimization,
$$\min_{\boldsymbol{x}_s}||(|\boldsymbol{x}_1|+|\boldsymbol{x}_2|)\odot\boldsymbol{x}_s-(|\boldsymbol{x}_1|-|\boldsymbol{x}_2|)||_2^2+\lambda_s||\boldsymbol{x}_s||_2^2,$$
which is solvable by conjugate gradient. The ℓ2-regularizer promotes the minimum-energy normalized image subtraction (i.e., with no noise amplification).
Results
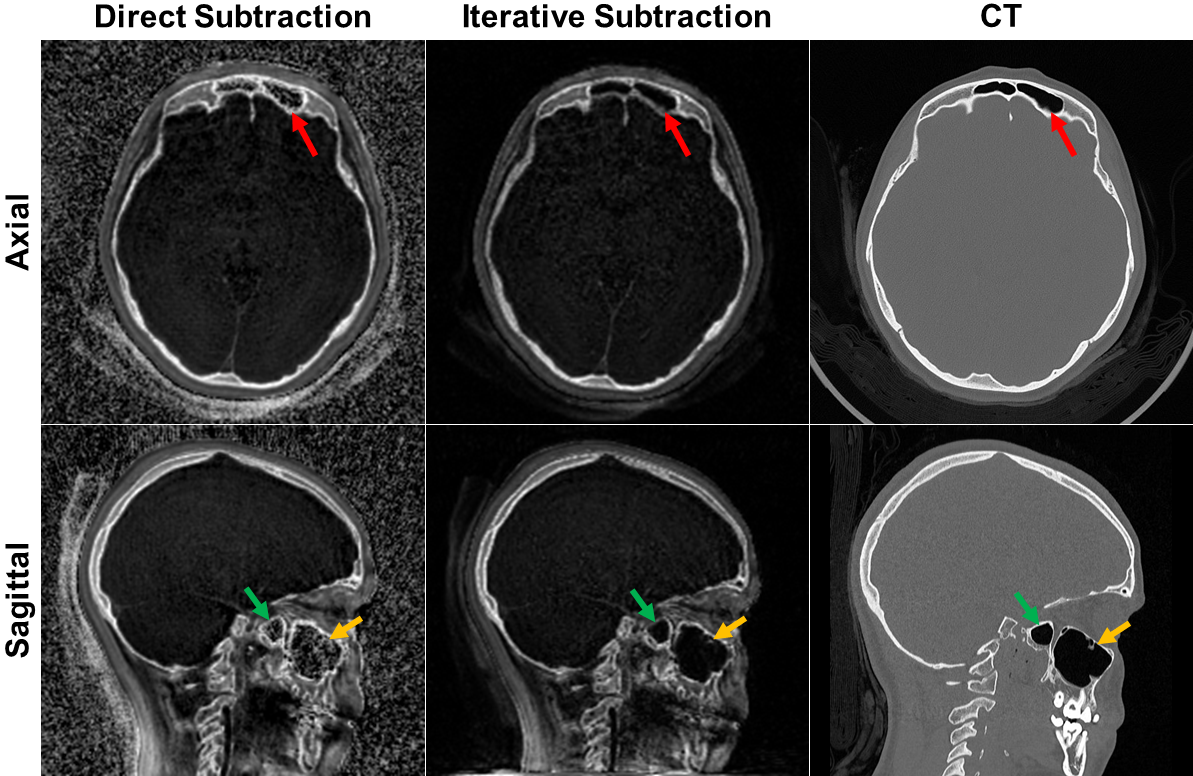
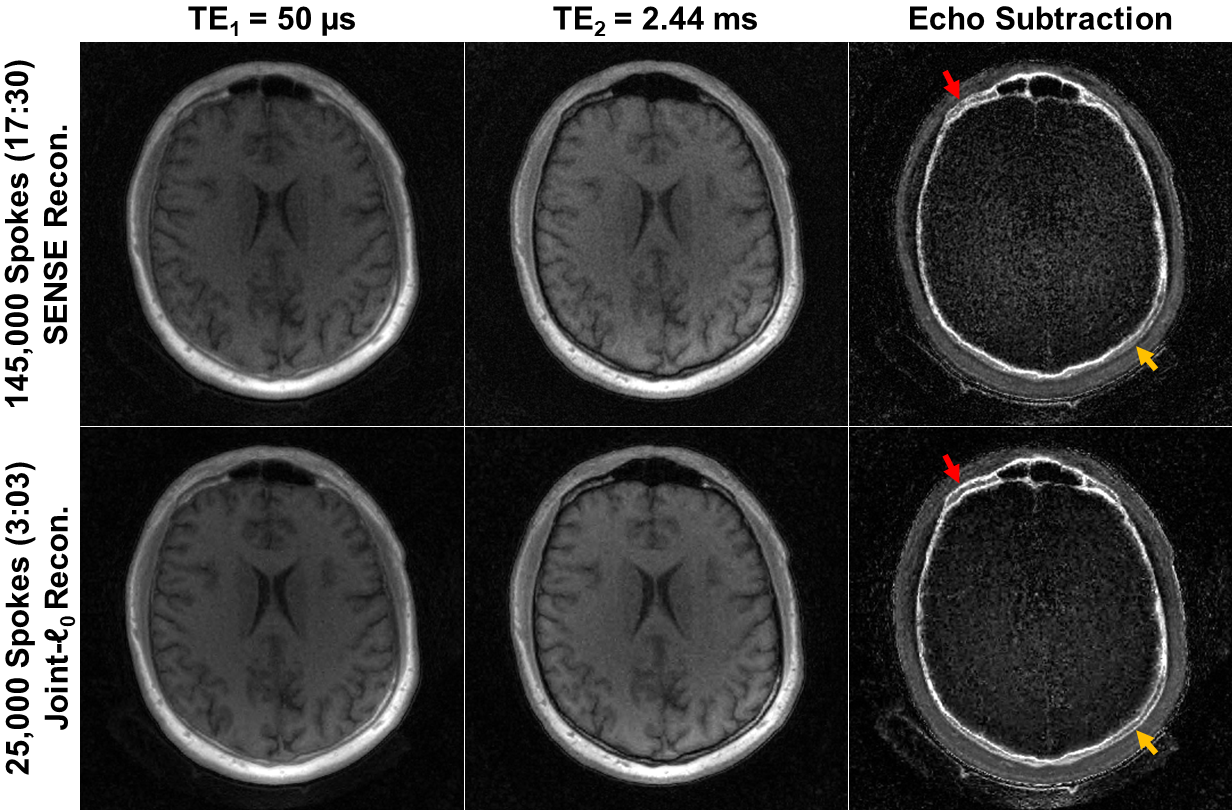
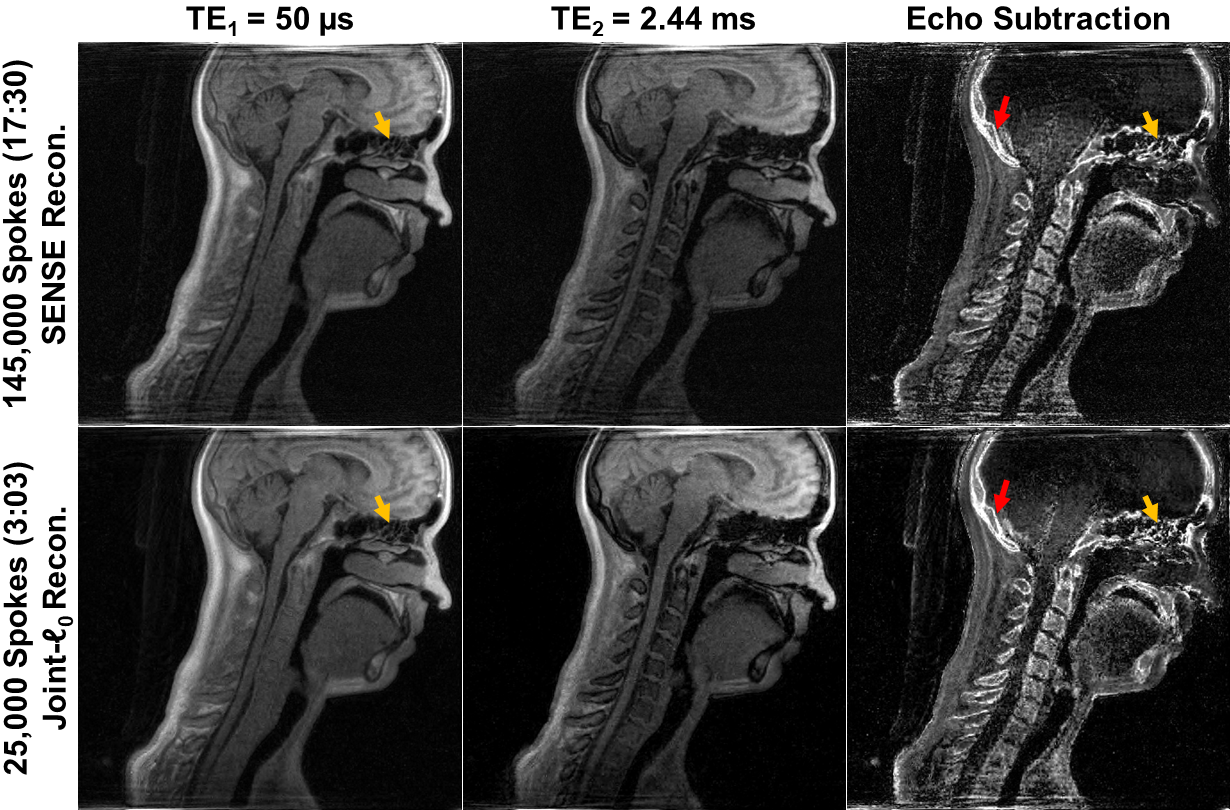
Figure 3 shows images of a pediatric patient acquired previously at 1.1 mm voxel size. While the direct echo subtraction amplifies background noise and produces false signal in the sinuses, the subtraction recomputed by conjugate gradient avoids these artifacts. Small structures are more easily visualized in the sinuses and at air-tissue interfaces. The resulting image contrast bears closer resemblance to CT.Figures 4 & 5 show axial and sagittal images acquired using the high-resolution dual-echo sequence for scan times of 17.5 (satisfying about half the Nyquist rate) and 3 minutes. A 3-minute scan reconstructed with joint ℓ0-wavelet regularization has comparable quality to the 17.5-minute scan for both ultrashort and conventional echo images. However, the depiction of cortical bone edges in the image subtraction is much sharper in the 3-minute scan. Acquisition and reconstruction at 0.65 mm voxel side length enables visualization of the cribriform plate bony structures.
Discussion
Rapid and high-resolution dual-echo imaging is made possible by parallel imaging and a joint ℓ0-wavelet regularizer, which ensures that the reconstructions of both echoes share the same set of nonzero wavelet coefficients. A shorter scan mitigates the possibility for motion blurring, and the joint regularizer suppresses noise while preserving image edges. These factors contribute towards the higher image quality seen in the echo subtraction of the shorter scan in Figures 4 & 5. Computation of the echo subtraction by conjugate gradient produces an image with contrast that closely resembles that of CT. Small bony structures near air cavities are better visualized in the high-resolution echo subtraction.Conclusion
This work details a dual-RF, dual-echo method for rapid high-resolution imaging of the hard and soft tissues in the head and neck. A joint regularizer and improved echo subtraction algorithm enables simultaneous acquisition of 3 image contrasts in 3 minutes.Acknowledgements
NIH R01 AR50068, R01 AR068382, R01 AR076392, R21 DE028417, T32 EB009384. This material is based upon work supported by the National Science Foundation under Grants No. 2026906 and 1845298.References
1. Kirmi O, Lo SJ, Johnson D, Anslow P, editors. Craniosynostosis: a radiological and surgical perspective. Seminars in Ultrasound, CT and MRI; 2009: Elsevier.
2. Mönninghoff C. Radiological Investigations of Craniofacial Malformations. Fundamentals of Craniofacial Malformations: Vol 1, Disease and Diagnostics: Springer; 2021. p. 321-44.
3. Lee H, Zhao X, Song HK, Zhang R, Bartlett SP, Wehrli FW. Rapid dual-RF, dual-echo, 3D ultrashort echo time craniofacial imaging: A feasibility study. Magn Reson Med. 2019;81(5):3007-16. Epub 20181218. doi: 10.1002/mrm.27625. PubMed PMID: 30565286; PMCID: PMC6414254.
4. Zhang R, Lee H, Zhao X, Song HK, Vossough A, Wehrli FW, Bartlett SP. Bone-selective MRI as a nonradiative alternative to CT for craniofacial imaging. Academic radiology. 2020;27(11):1515-22.
5. Zimmerman CE, Khandelwal P, Xie L, Lee H, Song HK, Yushkevich PA, Vossough A, Bartlett SP, Wehrli FW. Automatic Segmentation of Bone Selective MR Images for Visualization and Craniometry of the Cranial Vault. Academic radiology. 2022;29:S98-S106.
6. Johnson EM, Vyas U, Ghanouni P, Pauly KB, Pauly JM. Improved cortical bone specificity in UTE MR Imaging. Magnetic resonance in medicine. 2017;77(2):684-95.
7. Parikh N, Boyd S. Proximal algorithms. Foundations and trends® in Optimization. 2014;1(3):127-239.
8. Uecker M, Hohage T, Block KT, Frahm J. Image reconstruction by regularized nonlinear inversion—joint estimation of coil sensitivities and image content. Magnetic Resonance in Medicine. 2008;60(3):674-82.
9. Ong F, Uecker M, Lustig M. Accelerating non-Cartesian MRI reconstruction convergence using k-space preconditioning. IEEE transactions on medical imaging. 2019;39(5):1646-54.
Figures