1508
Ferumoxytol-enhanced Cardiac MRI for Delineation of Intramyocardial Hemorrhage1Division of Cardiology, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, Los Angeles, CA, United States, 2Radiation Oncology, University of Washington, Seattle, WA, United States, 3Physics and Biology in Medicine Graduate Program, University of California Los Angeles, Los Angeles, CA, United States, 4Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 5Pathology and Laboratory Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
Keywords: Myocardium, Myocardium, hemorrhage, intramyocardial hemorrhage, myocardial infarction, ischemia-reperfusion injury, ischemia , animals, blood, blood vessels, cardiovascular, contrast agents, contrast mechanisms, heart, novel contrast mechanism, preclinical
Motivation: Intramyocardial hemorrhage (IMH) frequently occurs in acute myocardial infarction (AMI) and is associated with adverse outcomes. While T2* cardiac magnetic resonance (CMR) imaging has emerged as the reference standard for noninvasive IMH detection, it relies on the paramagnetic properties of hemoglobin breakdown products, usually detectable between 1 and 3 days following IMH.
Goal(s): We demonstrate an alternative approach that can more promptly detect active myocardial bleeding.
Approach: We leveraged the T1 shortening effects of intravascular ferumoxytol to identify IMH following acute ischemia-reperfusion injury.
Results: Ferumoxytol-enhanced CMR depiction of IMH were in agreement with gross and histologic evaluations.
Impact: We demonstrate the effectiveness of ferumoxytol-enhanced cardiovascular magnetic resonance (FE-CMR) in detecting active intramyocardial hemorrhage after ischemia-reperfusion injury. This may facilitate the development, testing, and clinical adoption of strategies to mitigate IMH-associated complications.
Introduction
Intramyocardial hemorrhage (IMH) reflects the extravasation and aggregation of erythrocytes into the extravascular space as a consequence of severe microvascular injury. It is a frequent complication following revascularization in the setting of acute ST-elevation myocardial infarction (MI). IMH is associated with larger MI size, adverse left ventricular (LV) remodeling, and increased late arrhythmogenic risk due to iron deposition in the myocardium1,2. Cardiac magnetic resonance (CMR) techniques using T2* imaging are currently regarded as the reference standard for in vivo post-infarct IMH detection3. However, this method relies on the accumulation of hemoglobin breakdown products, which typically occur between 1 and 3 days following IMH. Ferumoxytol is an ultrasmall superparamagnetic iron-oxide nanoparticle approved by the U.S. Food and Drug Administration for intravenous treatment of iron deficiency anemia in adults with chronic kidney disease. However, its unique magnetic properties, high relaxivity, and long intravascular half-life (approximately 14-15 hours) are useful for a variety of emerging magnetic resonance imaging applications4. We aim to demonstrate an alternative approach to T2* imaging for identifying active myocardial bleeding. We hypothesize that the intravascular properties of ferumoxytol, which shortens the myocardial T1 value, can detect the leakage of ferumoxytol and blood into the extravascular space in the setting of IMH following ischemia-reperfusion injury.Methods
Swine (N=22, Yorkshire breed, all males, 25-35 kg) were subjected to percutaneous coronary balloon occlusion of the left anterior descending (LAD) coronary artery. After two brief preconditioning balloon inflations, total occlusion of the vessel was verified by cineangiography and was maintained for 8-50 minutes, depending on how well the animal tolerated the intervention. Collagenase (3.5-3.9 mg, Clostridium Histolyticum, Type VII-S) was directly injected intracoronary distal to the inflated balloon. Ferumoxytol-enhanced cardiovascular magnetic resonance (FE-CMR) (ferumoxytol 4 mg/kg) was performed on a 3.0 T clinical grade magnet (Prisma, Siemens Medical Solutions, Malvern, PA, USA) immediately after intervention. Pre-contrast cine steady-state free precession (SSFP) and post-contrast cine gradient echo imaging, as well as pre- and post-contrast T1 mapping was performed using the 5(3)3(3)3 modified Lock-Locker inversion (MOLLI) recovery sequence5. Animals were subsequently euthanized, and hearts were explanted. Gross examination and histological staining were performed.Results
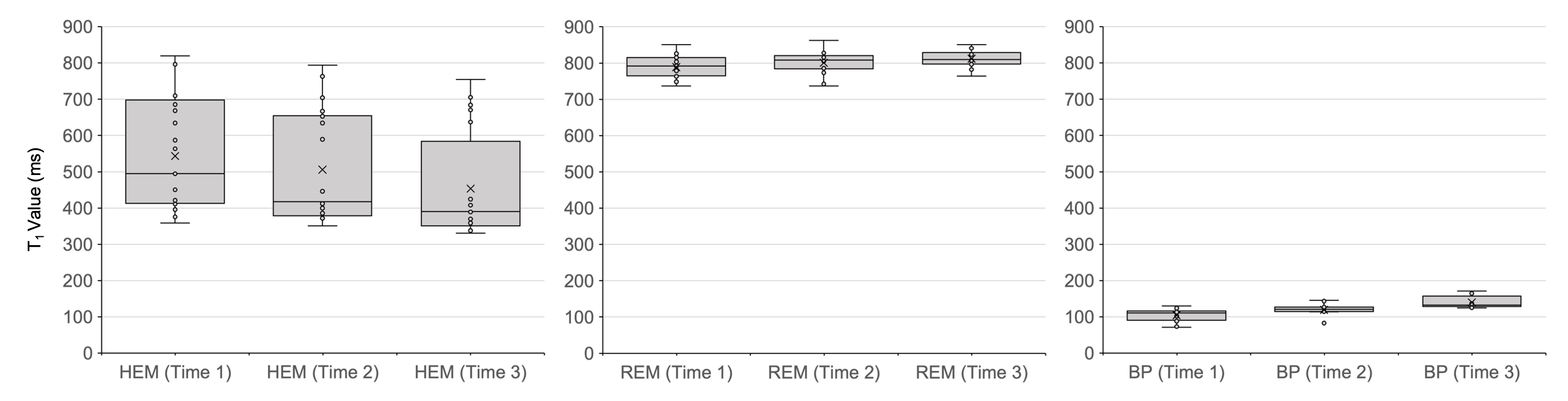
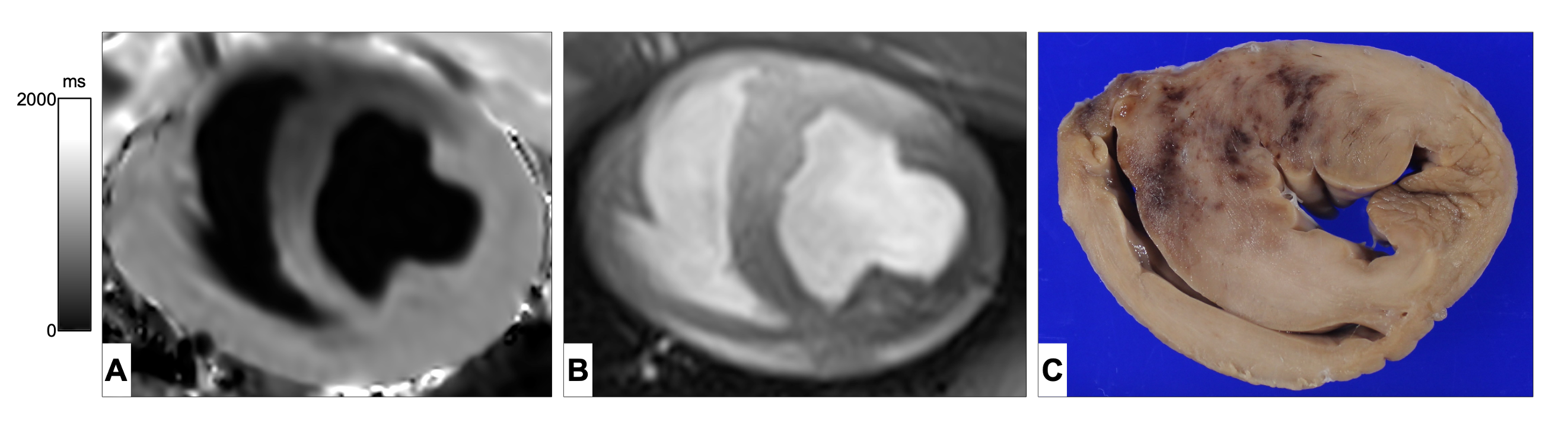
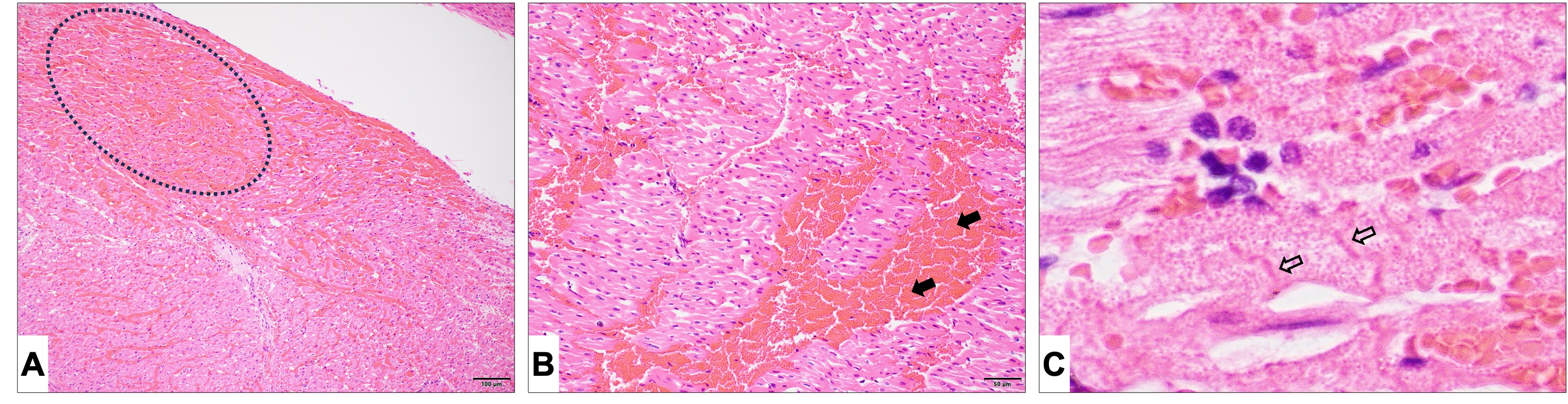
Nine animals (out of 22) died during the interventional procedure (n=3 pre-collagenase; n=6 post-collagenase) and 4 animals died post procedure but prior to completing the FE-CMR examination, representing an overall mortality rate of 59%. This resulted in n=9 that survived the intervention and completed the study. In 4 of the 9 animals (–IMH group) that completed the study, no signs of hemorrhage were found on FE-CMR, gross examination, or histopathological analysis. These animals experienced an average balloon occlusion time of 29.8 ± 15.9 minutes. Hemorrhage was detected in the remaining 5 surviving animals (+IMH), which experienced an average balloon occlusion time of 43.2 ± 7.7 minutes. In the +IMH group, post-contrast T1 values in the anteroseptal region supplied by the LAD coronary artery (hemorrhagic zone) were significantly shorter compared to remote tissue in the lateral myocardial region, reflecting leakage of ferumoxytol and blood into the extravascular space. The median [IQR] T1 value for the hemorrhagic and remote tissues were 420 ms [380.5, 656.3] and 806.0 ms [781.0, 818.8] (p < 0.0001), respectively. Over a period of 1.5 hours post-interventional procedure, the mean post-contrast T1 percent change in the hemorrhagic zone decreased by 10.2% (Figure 1). Conversely, in remote tissue and blood pool, the mean post-contrast T1 percent change increased by 2.6 and 23.5%, respectively. FE-CMR findings were in agreement with gross and microscopic evaluations (Figures 2 and 3).Conclusion:
FE-CMR offers a unique means of identifying acute, active intramyocardial bleeding. These findings may facilitate future research aimed at developing and testing novel therapeutics and/or interventions to mitigate IMH burden in the setting of ischemia-reperfusion injury.Acknowledgements
We thank Mimi Li, Guowen Shao, Zixuan Zhao, Fatima Mussina, and staff members at the UCLA Radiology Translational Research Imaging Center and the UCLA Division of Laboratory Animal Medicine for their assistance. This work was supported in part by the National Institutes of Health (R01HL169695) and the Veterans Health Administration (I01CX001901). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.References
1. Cokic I, Kali A, Yang HJ, et al. Iron-Sensitive Cardiac Magnetic Resonance Imaging for Prediction of Ventricular Arrhythmia Risk in Patients With Chronic Myocardial Infarction: Early Evidence. Circulation Cardiovascular imaging. Aug 2015;8(8)doi:10.1161/circimaging.115.003642
2. Mather AN, Fairbairn TA, Ball SG, Greenwood JP, Plein S. Reperfusion haemorrhage as determined by cardiovascular MRI is a predictor of adverse left ventricular remodelling and markers of late arrhythmic risk. Heart. 2011;97(6):453-459.
3. O'Regan DP, Ahmed R, Karunanithy N, et al. Reperfusion hemorrhage following acute myocardial infarction: assessment with T2* mapping and effect on measuring the area at risk. Radiology. 2009;250(3):916-922.
4. Knobloch G, Colgan T, Wiens CN, et al. Relaxivity of Ferumoxytol at 1.5 T and 3.0 T. Invest Radiol. May 2018;53(5):257-263. doi:10.1097/RLI.0000000000000434
5. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med. Jul 2004;52(1):141-6. doi:10.1002/mrm.20110
Figures