1507
The diagnostic accuracy of model-based quantitative perfusion cardiac MR at 3.0T for the detection of flow-limiting coronary artery disease1Radiology, Mie University Hospital, Tsu, Japan, 2Cardiology and Nephrology, Mie University Hospital, Tsu, Japan
Synopsis
Keywords: Atherosclerosis, Cardiovascular, Myocardial Perfusion
Motivation: Model-based quantitative myocardial perfusion MRI is feasible. However, few studies have investigated its diagnostic accuracy in detecting significant coronary artery disease (CAD).
Goal(s): To evaluate the diagnostic accuracy of quantitative stress myocardial perfusion MRI using Patlak plot method for the detection of significant CAD.
Approach: Myocardial blood flow (MBF) and myocardial flow reserve (MFR) determined by Patlak analysis of stress perfusion MRI with LV blood saturation correction were compared with fractional flow reserve.
Results: Model-based quantitative stress perfusion MRI has a high diagnostic accuracy for detecting significant CAD with the AUC of 0.739 and 0.745 for stress MBF and MFR, respectively.
Impact: Absolute quantification of myocardial blood flow and myocardial flow reserve by stress-rest myocardial perfusion MRI with model-based approach permits accurate and objective assessment of myocardial ischemia due to flow-limiting obstructive coronary artery disease, which can aid daily routine clinical practice.
Introduction
Visual analysis of stress perfusion cardiac magnetic resonance (CMR) requires long learning curve for accurate diagnosis of significant coronary artery disease (CAD). Fully quantitative analysis of myocardial perfusion CMR may permit an accurate, objective assessment of myocardial ischemia in patients with suspected CAD. Accurate MBF quantification by myocardial perfusion CMR relies on a linear relationship between signal intensity (SI) and gadolinium concentration. This can be corrected by using dual-bolus technique employing dilute pre-bolus 1. Patlak plot method, which is based on a single-tissue compartment model, allows for measurement of the transfer constants from the blood to the tissue compartment, K1, of gadolinium contrast medium by linear least-square fitting, substantially simplifying the analytical procedures. K1 can be converted to absolute MBF employing the predetermined relationship between MBF and K1. Consequently, model-based Patlak plot analysis of perfusion CMR with corrections of blood saturation and flow-dependent alteration in extraction fraction of gadolinium contrast medium can provide quantification of absolute MBF 2. However, few studies have investigated the diagnostic accuracy of quantitative perfusion CMR using model-based Patlak plot method. The purpose of this study was to evaluate the diagnostic accuracy of quantitative analyses of stress myocardial perfusion CMR using model-based Patlak plot method against a reference standard of fractional flow reserve (FFR).Methods
Fifty-seven patients with suspected CAD who underwent both CMR including stress perfusion MRI at 3.0T and FFR within 6 months were studied. CMR included cine MRI, pre-bolus perfusion MRI for the correction of T1 saturation of LV blood pool, stress and rest perfusion MRI, and late gadolinium enhanced (LGE) MRI. Gadolinium contrast medium (Gd-DOTA) (0.03 mmoL/kg) was administered during stress and rest perfusion MRI at a flow rate of 4 mL/s, followed by a 20-mL saline flush. Stress CMR was induced by adenosine triphosphate (ATP). For pre-bolus perfusion CMR, a bolus of 10%-dilute gadolinium contrast medium (0.003 mmol/kg) was injected with same injection protocol as stress and rest perfusion MR. Dual-bolus method was used to correct for T1 saturation of LV blood during first-pass of gadolinium contrast medium using a saturation ratio (SR) defined as 10-times peak SI of dilute pre-bolus scan divided by SI of non-dilute perfusion scan. Alternatively, fixed SR value of 1.67, that was mean SR at the peak LV gadolinium concentration (3.5mM) 3, was used in single-bolus approach for the saturation correction. Myocardial unidirectional influx constant (K1) was calculated by Patlak plot method using blood input and myocardial output functions. The relationship between the extraction fraction (E) of Gd-DOTA and MBF was previously determined as E=1-exp(-(0.24xMBF+0.63)/MBF). Absolute MBF were obtained from K1 with correction of E. MBF was determined within the AHA 16 myocardial segments. These 16 segments were further subdivided into 32 segments, considering both endocardial and epicardial halves. Myocardial flow reserve (MFR) was calculated as the ratio of stress to rest MBF. The flow-limiting obstructive CAD was defined as FFR <0.80 or luminal diameter reduction of >75%. Coronary territory was visually adapted blind to the result of invasive coronary angiography.Results
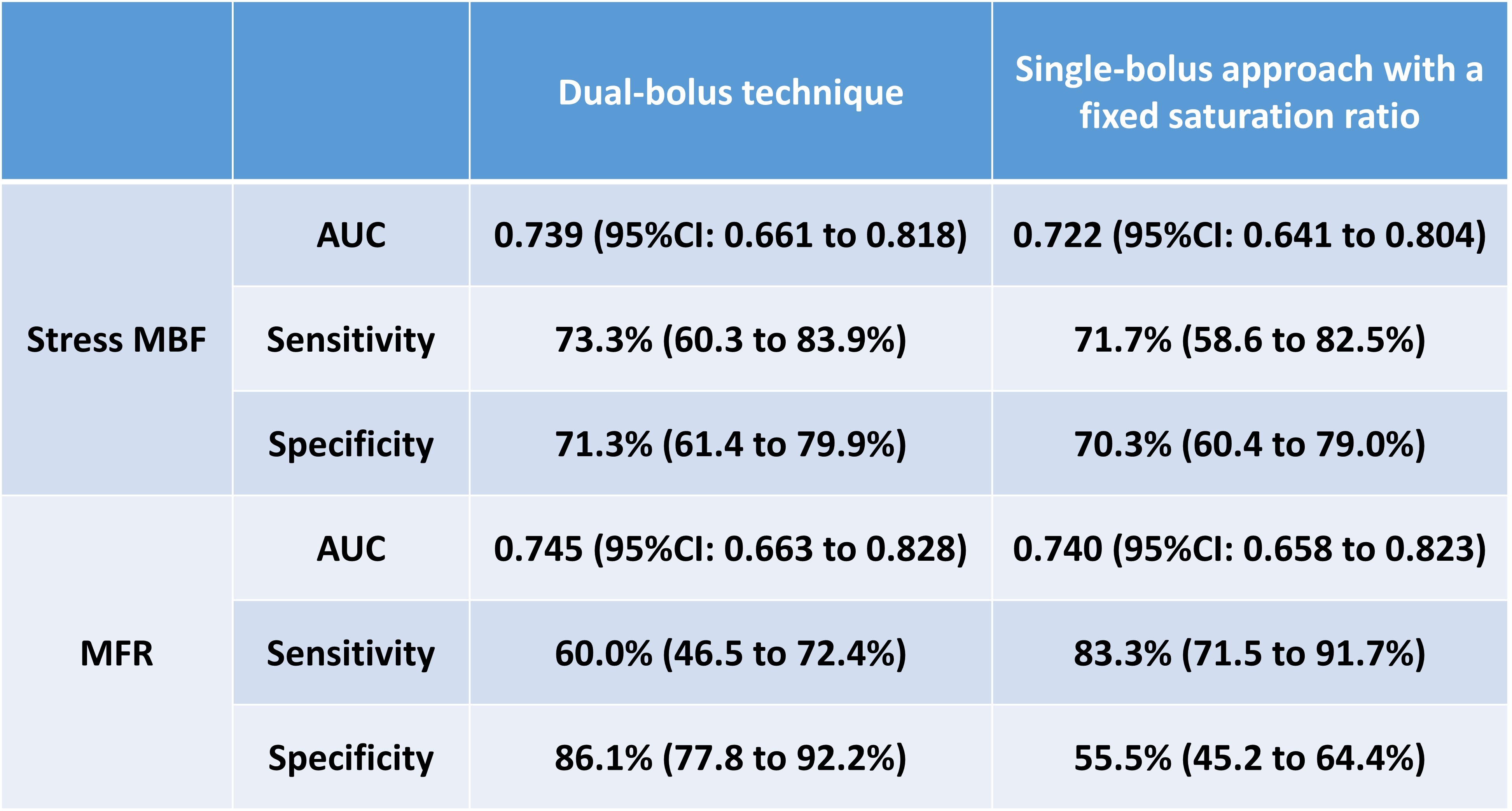
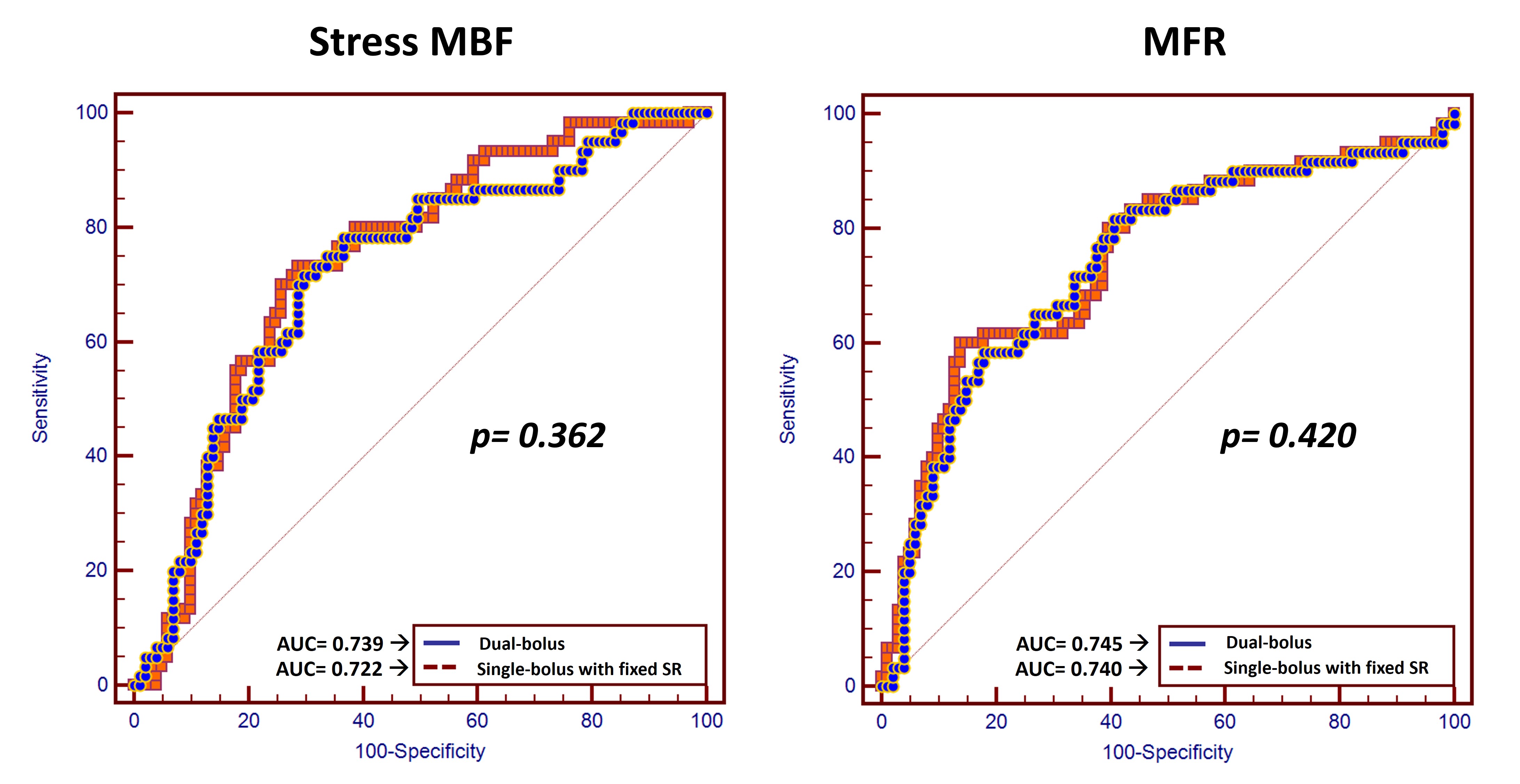
Total of 161 vessels of 57 patients were evaluated. Ten vessels were excluded from analysis due to hypoplasty or technical difficulty of FFR. Sixty of 161 (37.3%) vessels had obstructive CAD. The area under the receiver-operating characteristic curve (AUC) for stress MBF and MFR was 0.739 and 0.745 with a sensitivity of 73.3% and 60.0%, and specificity of 71.3% and 86.1% for dual-bolus technique, and 0.722 and 0.740 with a sensitivity of 71.7% and 83.3%, and specificity of 70.3% and 55.5% for single-bolus approach, respectively (Figure 1). No significant difference were observed in AUC between dual-bolus technique and single-bolus approach with fixed saturation ratio in both stress MBF (p=0.362) and MFR (p=0.420) (Figure 2).Discussion
Quantitative perfusion CMR employing model-based Paltak plot method with the correction of T1 saturation of the LV blood pool is feasible and provide similar diagnostic accuracy with either the dual-bolus technique or the single-bolus approach with a fixed value of SR for detecting hemodynamically significant coronary artery disease. Further, stress MBF and MFR provided similar diagnostic accuracy. These findings suggest that by employing our proposed model-based quantitative perfusion CMR can eliminate the rest perfusion scan from the protocol for the assessment of patients with suspected CAD.Conclusion
Quantitative analyses of stress myocardial perfusion CMR using model-based Patlak plot method has a high diagnostic accuracy for detecting hemodynamically significant coronary artery disease, both with the dual-bolus technique and the single-bolus approach with a fixed value of the ratio, for T1 saturation correction of LV blood signal.Acknowledgements
No acknowledgement found.References
1. Ichihara T, Ishida M, Kitagawa K, et al. Quantitative analysis of first-pass contrast-enhanced myocardial perfusion MRI using a Patlak plot method and blood saturation correction. Magn Reson Med. 2009;62(2):373-383.
2. Ishida M, Ichihara T, Nagata M, et al. Quantification of myocardial blood flow using model based analysis of first-pass perfusion MRI: extraction fraction of Gd-DTPA varies with myocardial blood flow in human myocardium. Magn Reson Med. 2011;66(5):1391-1399.
3. Ishida M, Sakuma H, Murashima S, et al. Absolute blood contrast concentration and blood signal saturation on myocardial perfusion MRI: estimation from CT data. J Magn Reson Imaging. 2009;29(1):205-210.
Figures