1503
The prediction value of CMR first-pass perfusion parameters for left ventricular reverse remodeling in dilated cardiomyopathy1The Second Affiliated Hospital of Nanchang University, Nanchang, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiomyopathy
Motivation: CMR first-pass-perfusion imaging (FPI) had revealed coronary microvascular dysfunction (CMD) in dilated cardiomyopathy (DCM). However, it’s unknown if FPI could predict left ventricular reverse remodeling (LVRR) in DCM.
Goal(s): Investigating the value of FPI parameters for predicting LVRR.
Approach: 94 DCM patients and 35 healthy controls were enrolled. FPI as well as the left ventricular structure, function and late gadolinium enhancement (LGE) parameters were analyzed.
Results: FPI showed more serious CMD in non-LVRR than LVRR. Timemax of FPI as well as left ventricular remodeling index and LGE extent were independent predictors.
Impact: This study firstly showed the role of FPI in predicting LVRR in DCM.
Introduction
Dilated cardiomyopathy (DCM) is a common disease leading to heart failure[1]. It is characterized by the enlargement and systolic dysfunction of ventricles that aren’t due to abnormal loading conditions such as hypertension or valve disease, or coronary artery disease[2, 3]. With the improvement of heart failure treatment, more patients are experiencing left ventricle reverse remodeling (LVRR) resulting with favorable long-term prognosis[3, 4]. Therefore, the prediction of LVRR would be beneficial for DCM patient management. Cardiac magnetic resonance (CMR) first-pass perfusion imaging (FPI) has been widely used to assess coronary microvascular dysfunction (CMD) in DCM patients[5]. Some studies reported CMD had incremental prediction value for poor prognosis in DCM patients. However, the relationship between myocardial perfusion and LVRR in DCM remains unknown. Thus, this study aimed at investigating if CMR FPI could be used for predicting the LVRR in DCM.Materials and Methods
94 DCM patients were retrospectively selected including 53 non-LVRR and 41 LVRR. 35 healthy volunteers were also recruited.All CMR were acquired on a 3T MRI system (Discovery MR750W; GE Healthcare, Milwaukee, CA, USA). Cine images were acquired by standard SSFP sequence before the injection of contrast agency. CMR FPI was obtained using FSE sequence with the intravenous injection of gadobutrol (Gadovist, Bayer HealthCare Pharmaceuticals, Germany). 10-15 minutes after contrast administration, an inversion recovery gradient echo sequence was used to acquire late gadolinium enhancement (LGE) imaging.
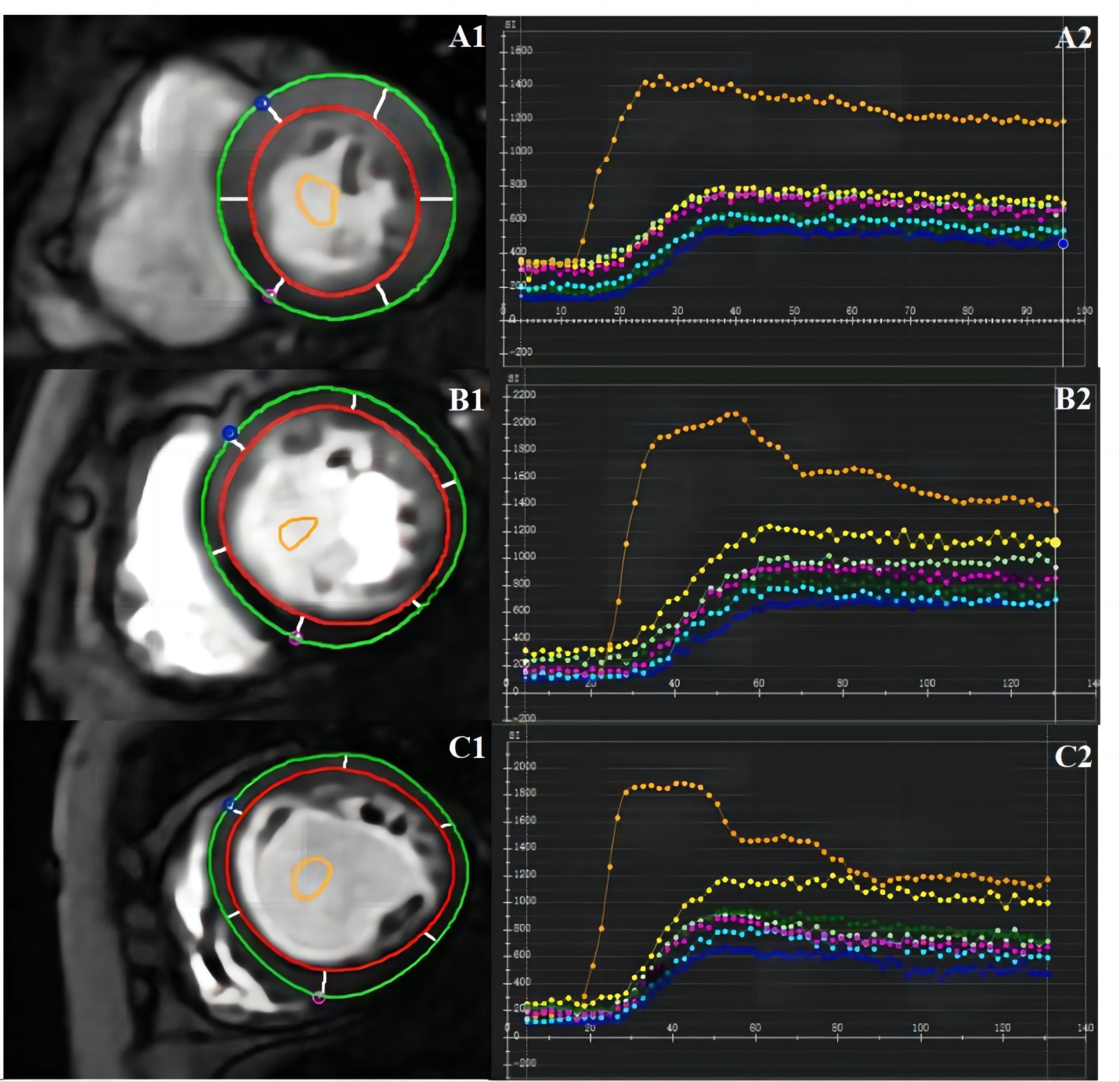
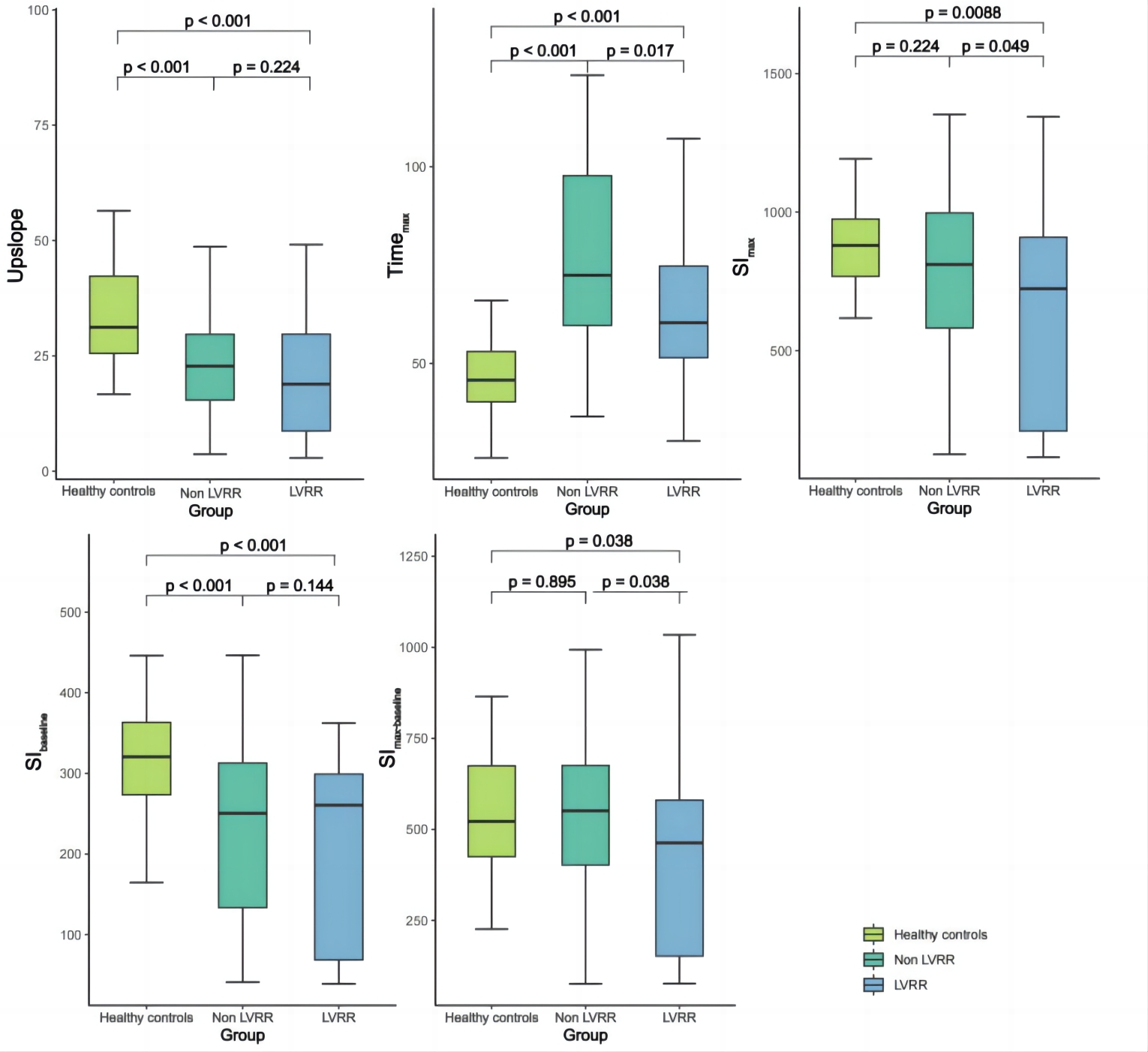
CVI was used to analysis cine, FPI and LGE images. As shown in Figure 1, the perfusion parameters includes upslope, Timemax, SImax, SIbaseline and SImax-baseline. They were automatically obtained from the myocardial time-signal intensity curves using CVI. One-way ANOVA was used to compare parameters among healthy control, LVRR and non-LVRR. Independent t-test was used for post hoc test. Univariable and multivariable logistic regression analyses were used to determine predictors of LVRR. Receiver operating characteristic (ROC) curve was used to assess the prediction performance. P < 0.05 was considered statistical significance.
Results
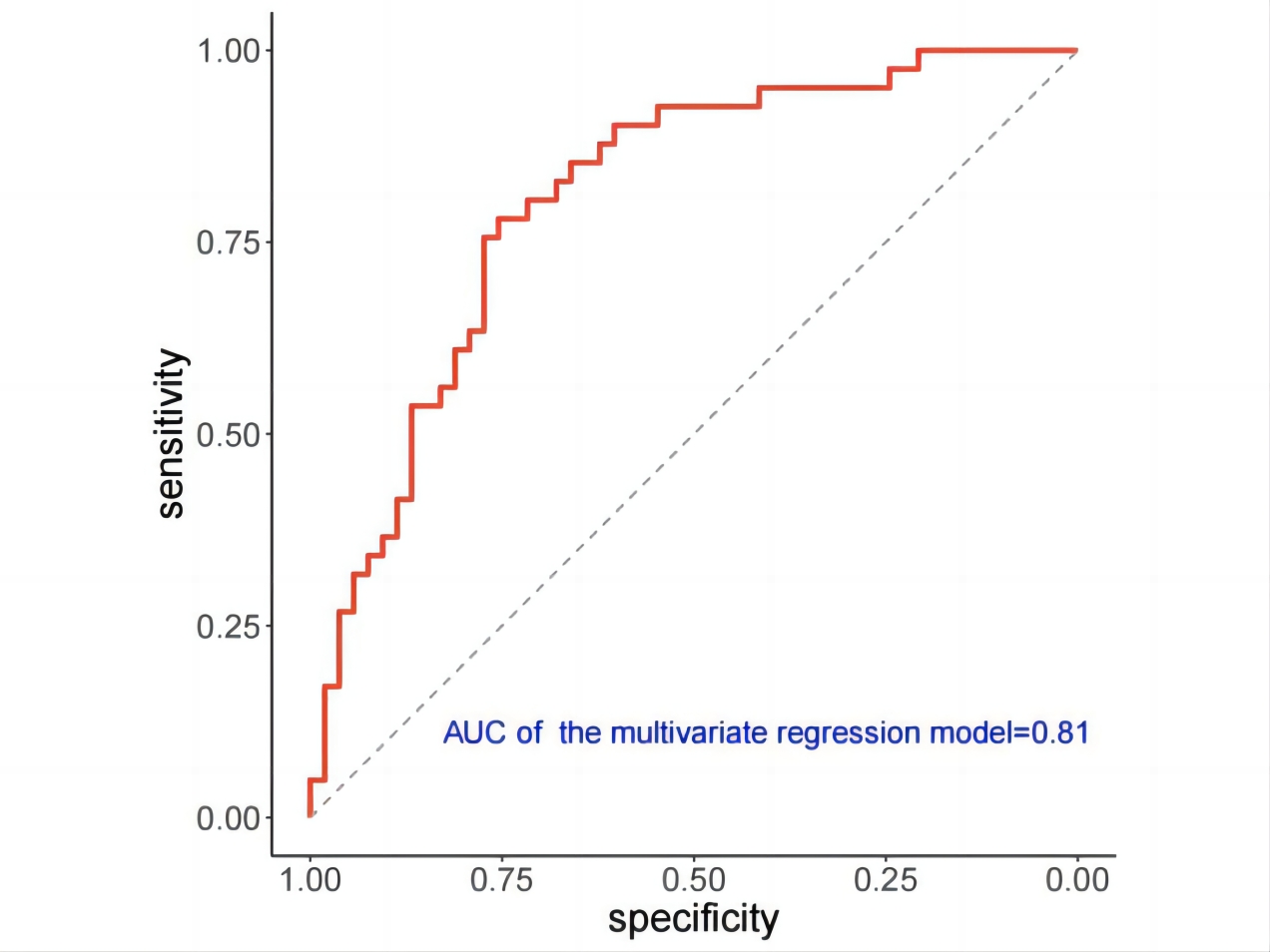
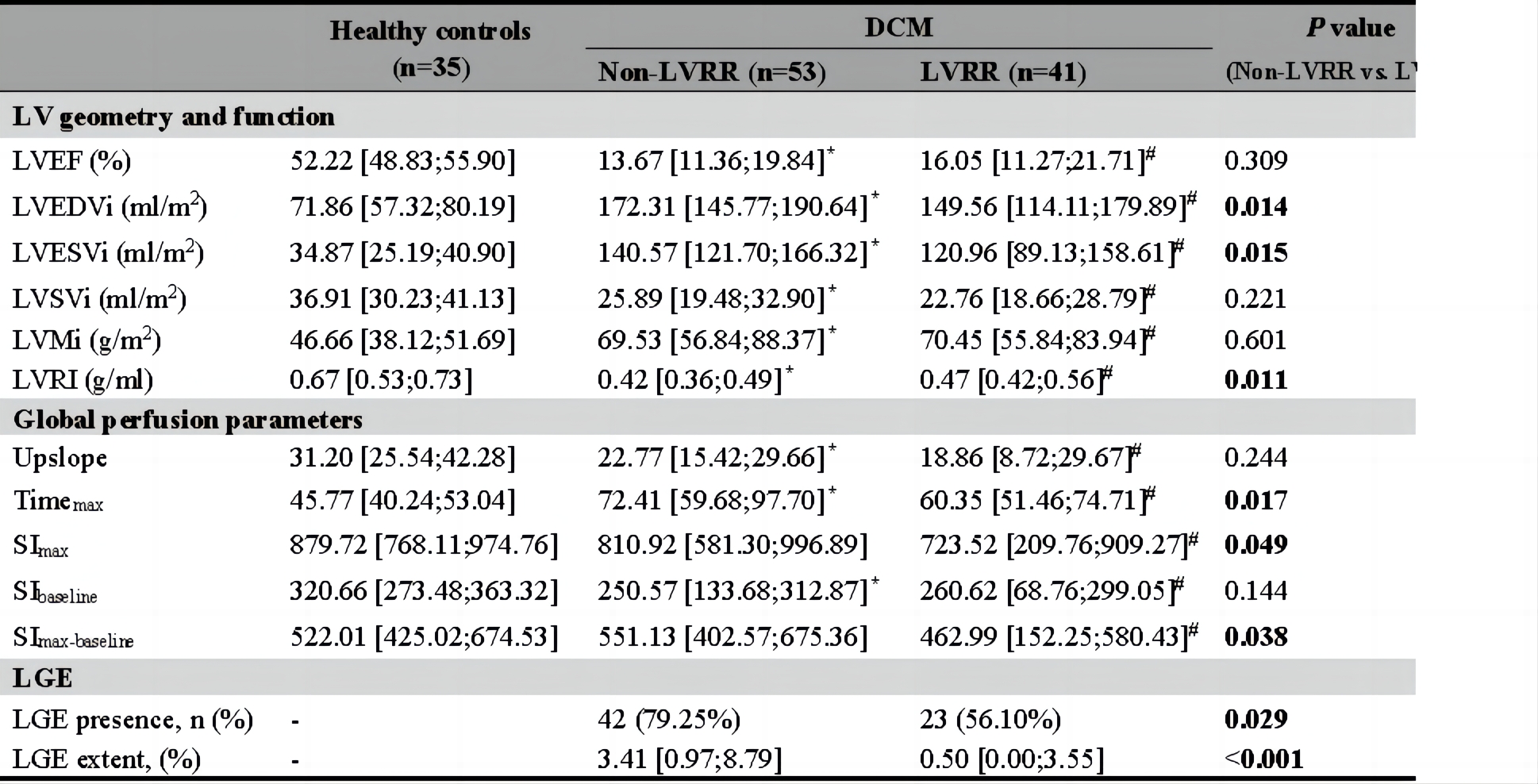
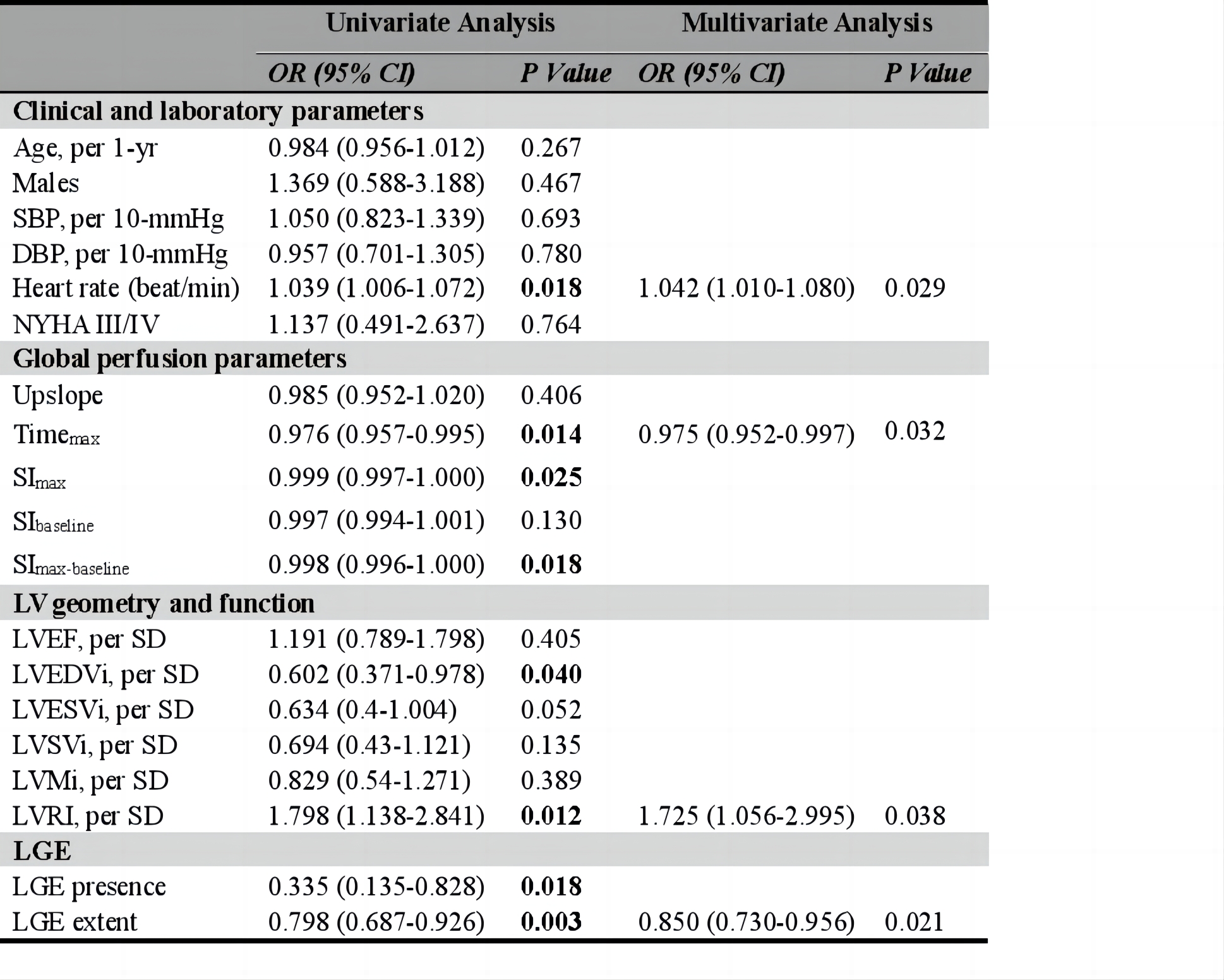
As shown in Table 1 and Figure 2, the healthy controls had better left ventricle (LV) function, including higher leftventricular remodeling index (LVRI) and lower LV geometry parameters than DCM patients (all p<0.05). Compared with healthy controls, DCM patients had worse myocardial perfusion, which was indicated by significantly lower upslope, SIbaseline, and increased Timemax values (all p<0.001). Compared to non-LVRR, LVRR had significantly decreased geometry parameters but increased LVRI at baseline. The Timemax, SImax and SImax-baseline were lower in the LVRR than the non-LVRR (all p<0.05). The other perfusion parameters and LV function parameters were not significantly different between the LVRR and non-LVRR. The non-LVRR had larger LGE extent than the LVRR group (p<0.001). The univariate analysis showed that heart rate, Timemax, SImax, SImax-baseline, LVEDVi, LVRI, LGE presence and LGE extent at baseline were significant correlated with LVRR (Table 2). The multivariate analysis revealed that heart rate (OR 1.042; 95% CI 1.010-1.080; p=0.029), Timemax (OR 0.975; 95% CI 0.952-0.997; p=0.032), LVRI (OR 1.725; 95% CI 1.056-2.995; p=0.038) and LGE extent (OR 0.850; 95% CI 0.730-0.956; p=0.021) were independent predictors of LVRR. The AUC of the multivariate model was 0.81 (95%CI, 0.71-0.88) (Figure 3).Discussion and conclusion
In this study, we investigated the value of CMR first-pass perfusion parameters for predicting LVRR in DCM patients. Our results showed Timemax of perfusion curve was a novel independent predictor of LVRR. Consistent with previous studies, the heart rate, LVRI and LGE extent were also independent predictors[6]. The combination of the four predictors could improve the prediction performance. The improvement in LV septal perfusion was associated with LVRR in nonischemic cardiomyopathy patients[7]. This suggests a potential correlation between myocardial perfusion and ventricular remodeling. Bietenbeck et al. reported DCM patients had CMD at rest by using CMR FPI, which was in line with the lower upslope, SIbaseline, and increased Timemax value in our study[8]. We firstly verified higher Timemax was an independent predictor of LVRR in DCM patients. Higher Timemax meant a longer wash-in time in damaged myocardium which caused by severer CMD. The CMD plays an important role in the progression of heart failure which has been verified by endomyocardial biopsy of DCM patients and animal models. It seemed the aggravated CMD may result with the progressive ventricular functional deterioration and adverse remodeling, which may hinder the occurrence of LVRR.In conclusion, the Timemax of CMR first-pass perfusion imaging was an independent predictor of LVRR in DCM patients.Acknowledgements
No acknowledgements found.
References
[1] Weintraub R G, Semsarian C, Macdonald P. Dilated cardiomyopathy[J]. Lancet, 2017,390(10092):400-414.
[2] Pinto Y M, Elliott P M, Arbustini E, et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position statement of the ESC working group on myocardial and pericardial diseases[J]. Eur Heart J, 2016,37(23):1850-1858.
[3] Hoshikawa E, Matsumura Y, Kubo T, et al. Effect of left ventricular reverse remodeling on long-term prognosis after therapy with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers and beta blockers in patients with idiopathic dilated cardiomyopathy[J]. Am J Cardiol, 2011,107(7):1065-1070.
[4] Kubanek M, Sramko M, Maluskova J, et al. Novel predictors of left ventricular reverse remodeling in individuals with recent-onset dilated cardiomyopathy[J]. J Am Coll Cardiol, 2013,61(1):54-63.
[5] Bietenbeck M, Florian A, Shomanova Z, et al. Reduced global myocardial perfusion reserve in DCM and HCM patients assessed by CMR-based velocity-encoded coronary sinus flow measurements and first-pass perfusion imaging[J]. Clin Res Cardiol, 2018,107(11):1062-1070.
[6] Ota S, Orii M, Nishiguchi T, et al. Implications of multiple late gadolinium enhancement lesions on the frequency of left ventricular reverse remodeling and prognosis in patients with non-ischemic cardiomyopathy[J]. J Cardiovasc Magn Reson, 2021,23(1):32.
[7] Ogano M, Iwasaki Y K, Tanabe J, et al. Cardiac resynchronization therapy restored ventricular septal myocardial perfusion and enhanced ventricular remodeling in patients with nonischemic cardiomyopathy presenting with left bundle branch block[J]. Heart Rhythm, 2014,11(5):836-841.
[8] Bietenbeck M, Florian A, Shomanova Z, et al. Reduced global myocardial perfusion reserve in DCM and HCM patients assessed by CMR-based velocity-encoded coronary sinus flow measurements and first-pass perfusion imaging[J]. Clin Res Cardiol, 2018,107(11):1062-1070.
Figures