1502
Non-Contrast Myocardium Perfusion using Stacks-of-Stars (SoS) Time-SLIP1Radiology, University of California San Diego, San Diego, CA, United States, 2Cardiology, University of California San Diego, San Diego, CA, United States
Synopsis
Keywords: Myocardium, Cardiovascular
Goal(s): To introduce Time-SLIP technique with Stack-of-Stars (SoS) sequence for more inclusive myocardial assessments without the need for contrast mediums.
Approach: Implemented diaphragm navigator echoes and T2-prep with the SoS sequence, refined through phantom trials, for tagging the proximal aortic root blood flow to visualize myocardial perfusion.
Results: Preliminary in-vivo scans indicate reduced stent-related artifacts and the feasibility of non-contrast perfusion quantification.
Impact: Our non-contrast myocardial perfusion approach offers a safer CAD evaluation, reducing risks from contrast agents. This method opens doors for inclusive patient assessments and encourages further refinement in non-invasive cardiac diagnostics.
Introduction
Cardiovascular diseases particularly Coronary Arterial Disease (CAD), continue to be a predominant health concern worldwide (1). Central to the evaluation of CAD is the assessment of myocardial perfusion, which traditionally hinges on stress tests to amplify differences between normal and stenotic or ischemic myocardium. These stress tests, combined with imaging modalities, often necessitate the use of contrast agents, bringing about inherent risks to certain patient groups (2). However, with the evolution of imaging techniques, the medical community is now presented with safer non-contrast alternatives that obviate the need for these stress agents (3-6). Our novel approach delves deeper into this realm, utilizing a refined Stack-of-Stars (SoS) sequenced integrated with Time-SLIP for gated myocardial perfusion assessments, complemented by diaphragm navigator echoes. In a notable departure from convention, our methodology modifies the segmentation order in accordance with the cardiac cycle, transitioning from slice dimension to radial trajectory dimension, subsequently optimized post phantom trials. Preliminary in-vivo findings are promising, highlighting not only diminished stent-associated artifacts but also suggesting a future where perfusion quantification can be achieved without resorting to stress agents or contrast mediums.Methods
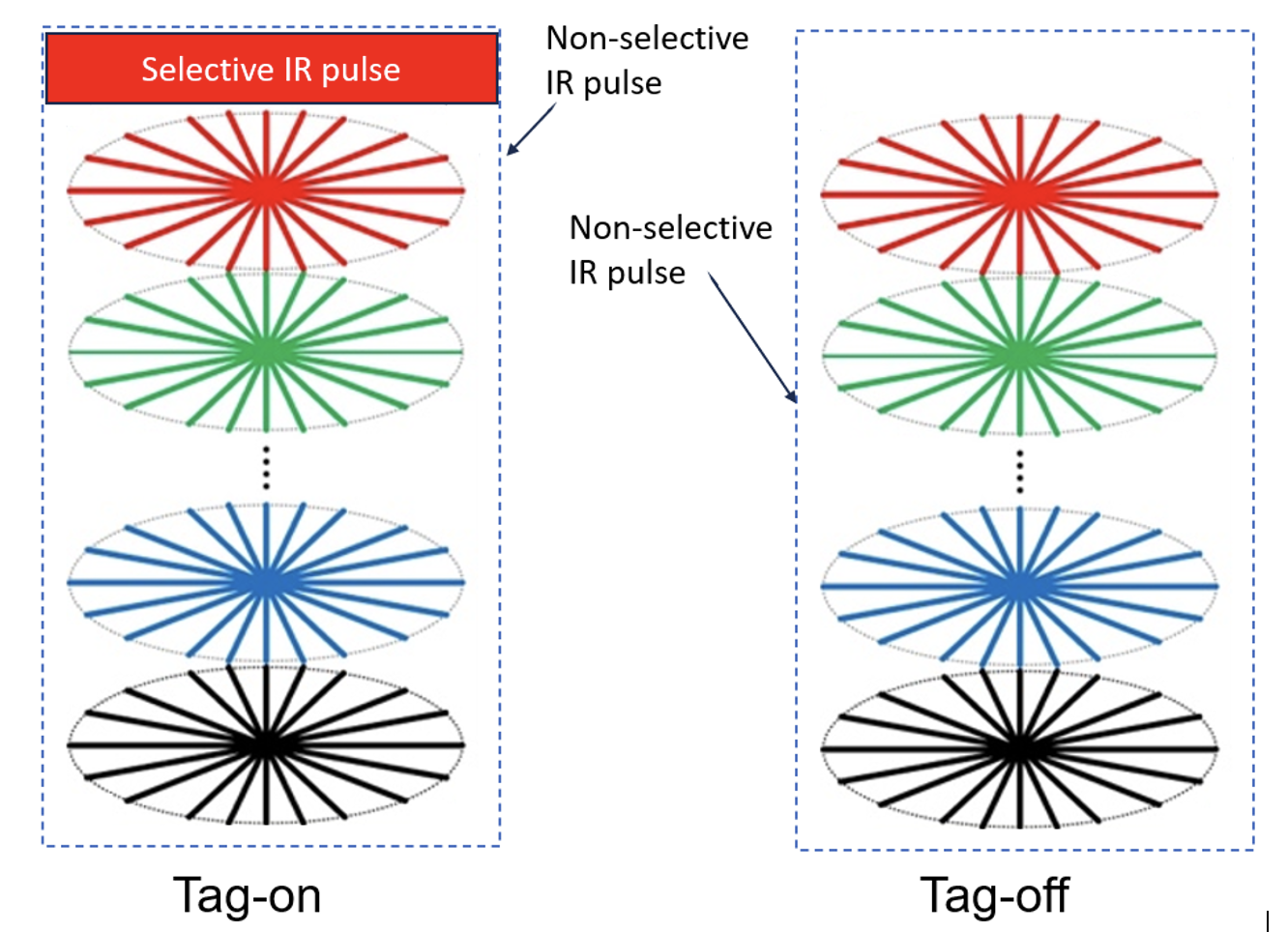
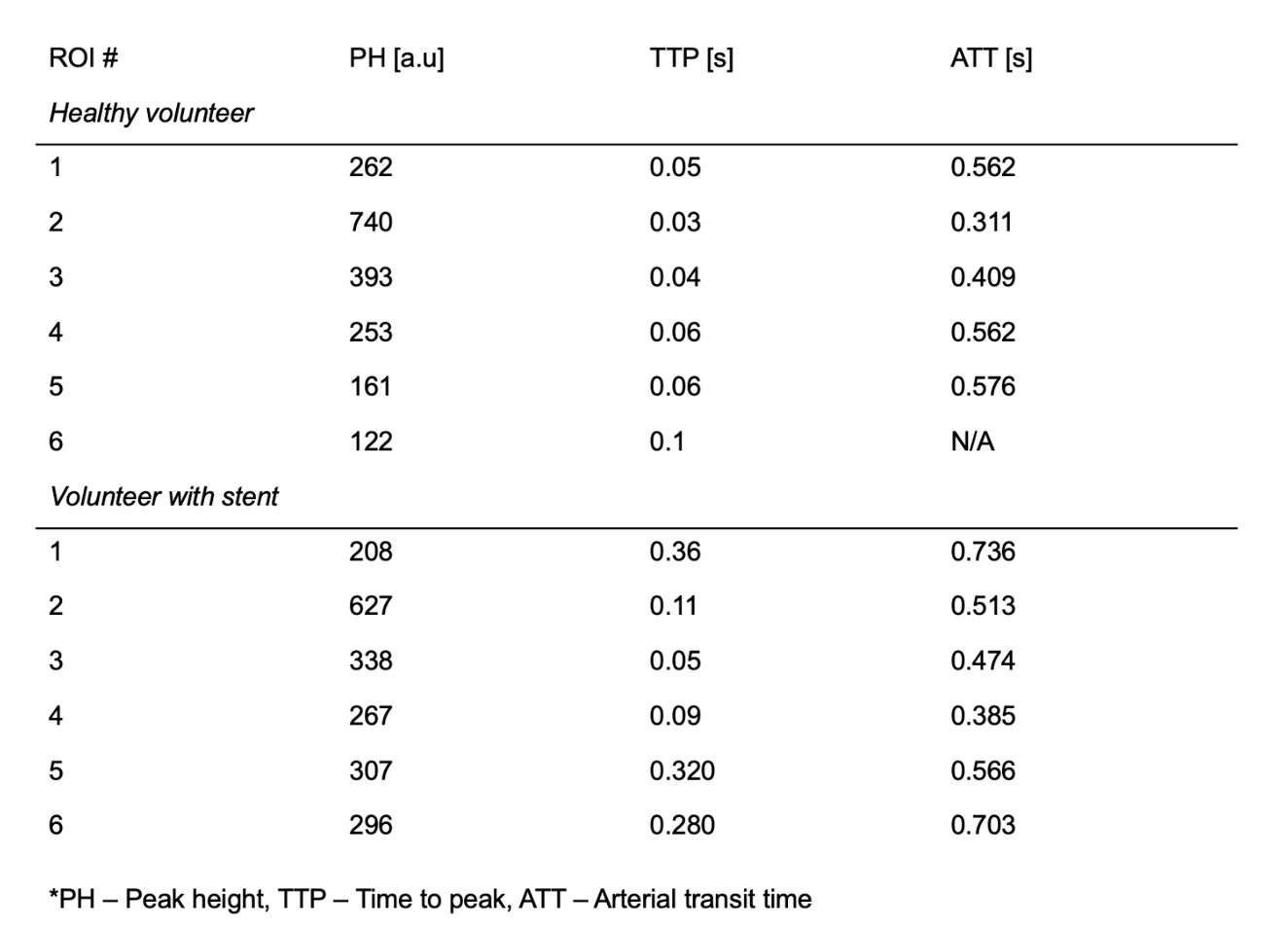
The study was approved by the Institutional Review Board. All MR imaging data were obtained with a clinical 3-T MR imager (Vantage Galan 3T, Canon Medical Systems, Japan). In-vivo scans were obtained on a healthy female 26 years old and a male volunteer 79 years old with a myocardial stent after obtaining written consent. Scanning protocol included SoS sequence with diaphragm navigator echoes, T2 prep, and Time-Slip with 6 inversion times (TI): 0.15 s, 0.3 s, 0.6 s, 0.9 s. The SoS pulse sequence with T2 preparation module and diaphragm navigator echoes was implemented. 4D Time-SLIP with 3D balanced steady-state free precession (bSSFP) was used to study non-contrast myocardial perfusion (used as a control). The tag position with both selective inversion recovery (sel-IR) and non-selective-IR (non-sel-IR) pulses is at the proximal aortic root, making only the tagged bright blood flow-out to the myocardium visible. Schematic is shown in Figure 1. Data was analyzed by fitting the subtraction (tag on - tag off) signal intensity yielding the following metrics: PH – peak height, TTP – time to peak in seconds and ATT – arterial transit time in seconds.Results
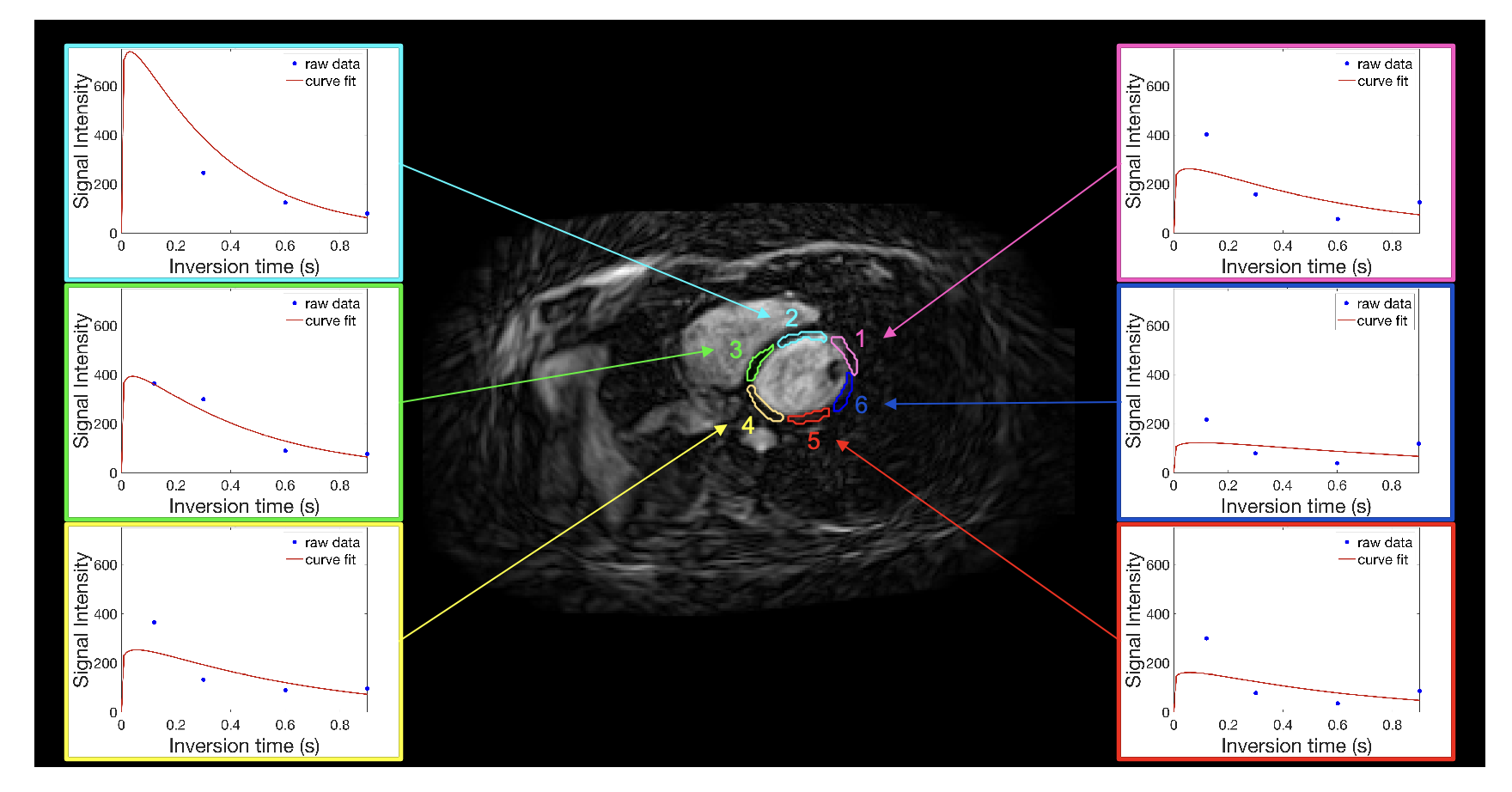
In Figure 2, a myocardium image from healthy female volunteer is featured, accompanied by perfusion fits for distinct myocardium segments. Table 1 summarizes the perfusion metrics of both the healthy female and male volunteer with stent.Discussion
Merging the Time-SLIP approach with adapted SoS sequence, we developed a methodology with promising implications for the future of non-contrast myocardial perfusion imaging. By incorporating diaphragm navigator echoes, adding T2 prep module and altering the segmentation dimension, we’ve seen enhancements in imaging quality without breath-hold and extending acquisition duration. Initial findings are promising and, when compared to conventional methods like bSSFP, highlight the feasibility of myocardial perfusion quantification even in subjects with stents. The core novelty is in our strategy of tagging blood flow at the proximal aortic root, rendering only the designate blood visible as it flows to the myocardium. This approach effectively suppresses extraneous myocardial and fat signals upon subtraction. In instances of stenosis, we anticipate that the resultant peaks will be attenuated and delayed. As the severity of the stenosis escalates, these peaks are expected to exhibit a more pronounced shift with an extended transition period.Conclusion
These advancements combined will enable an MR evaluation without the use of a gadolinium-based contrast agent.Acknowledgements
This work was supported by an NIH grant R01 HL154092 and a grant by Canon Medical Systems, Japan (35938).References
[1] Roth GA., et. al., J Am Coll Cardiol. 2020;76(25):2982-3021.
[2] Maddox TG., Am Fam Physician. 2002;66(7):1229-1234.
[3] Salerno M., et. al., Circ Cardiovasc Imaging. 2017 Jun;10(6):e003951.
[4] Chen, L., et. al., Medical physics, 39(8), 5204– 5211.
[5] Miyazaki M, et. al., Microvasc Res. 2015;98:94-101.
[6] Henningsson M, et. al., MAGMA. 2022;35(5):711-718.
Figures