1501
Novel iNAV-based 3D Whole-Heart Late Gadolinium Enhancement Low-Field (0.55T) Cardiovascular MRI1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 35Millenium Institute for Intelligent Healthcare Engineering, Santiago, Chile, 4MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 5Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Atherosclerosis, Low-Field MRI, Late gadolinium enhanced
Motivation: 3D whole-heart late gadolinium enhancement imaging has previously been demonstrated at 1.5T, but not at low-field (0.55T).
Goal(s): To develop a novel free breathing, whole-heart, late gadolinium enhancement imaging framework at low field.
Approach: Patients with known ischaemic heart disease were scanned and results of the proposed 3D sequence were compared with 2D LGE images.
Results: There is excellent agreement between the 3D and 2D datasets in the detection of myocardial scar.
Impact: Preliminary results demonstrate the feasibility of the proposed framework for comprehensive 3D whole-heart late gadolinium enhancement imaging for the detection of myocardial scar at 0.55T.
Introduction
Low-field (<1.5T) cardiac magnetic resonance imaging (CMR) is gaining attention due to its lower installation and operational costs, making it an attractive option to address CMR underutilisation. Other significant advantages of low-field CMR include diminished B0 inhomogeneities, lower specific absorption rate (SAR), reduced susceptibility artefacts and a wide bore making scanning more acceptable for claustrophobic and bariatric patients.1 Despite recent advances in technology, low-field scanners face inherent limitations in image quality associated with low signal-to-noise ratio (SNR)2. Late gadolinium enhancement (LGE) CMR plays a pivotal role in the diagnosis of myocardial infarction3 as well as the assessment of numerous non-ischaemic cardiomyopathies.4 In ischaemic heart disease, LGE serves as a key determinant in the assessment of myocardial viability and guides important management decisions including initiation of prognostic medications and coronary revascularisation.5–8 Conventional 2D inversion recovery (IR) and phase sensitive inversion recovery (PSIR) sequences have been widely incorporated into standard CMR protocols and have been adapted as research protocols for use at low-field. One of the inherent limitations at low-field is reduced T1 relaxivity, and therefore, reduced benefit from T1 lowering agents such as gadolinium-based contrast agents (GBCAs). 3D LGE imaging has previously been demonstrated at 1.5T.9 Here, we sought to develop an accelerated free-breathing, whole-heart, isotropic-resolution, 3D PSIR LGE imaging framework at 0.55T.Methods
The proposed framework (Fig.1) encompasses an ECG-triggered, free-breathing, 3D whole-heart, two-heartbeat, PSIR research sequence9 acquired with a 4.5-fold under-sampled variable-density Cartesian trajectory.10 Integration of low-resolution 2D image navigators (iNAV)11 ensures 100% respiratory scan efficiency and predictable scan durations. Image reconstruction involves iNAV-based beat-to-beat respiratory binning and intra-bin translational motion correction, bin-to-bin 3D non-rigid motion estimation, and non-rigid motion-corrected 3D patch-based low-rank denoising (PROST).12Image acquisition was performed on three patients with ischemic heart disease on a commercially available clinical 0.55T MRI scanner (MAGNETOM Free.Max, Siemens Healthineers AG, Erlangen, Germany) using the following parameters: coronal orientation, acceleration factor= 4.5 spatial resolution= 1.5mm3, FA = 110° and 80° for IR prepared magnitude and non-prepared reference volumes respectively and fat-sat pulse with FA=180° at each heart-beat. The trigger delay was defined by the diastolic rest period. A two-heartbeat TI look-locker scout was conducted prior to 2D and 3D acquisitions to determine the ideal TI for nulling the signal from the myocardium (bright-blood imaging). Following intravenous injection of GBCA (GADOVIST) at 0.2mmol/kg, free-breathing 2D PSIR LGE13 research sequences optimised for use at 0.55T were acquired in 4-chamber, 3-chamber, 2-chamber and short-axis stack views, followed by acquisition of the iNAV-based 3D PSIR LGE. The two datasets were compared for image quality and detection of LGE using the American Heart Association 17-segment model.14
Results
The iNAV-based 3D PSIR LGE research sequence at 0.55T was acquired within an average scan time of approximately 9 minutes. 3D PSIR LGE (reformatted to display typical LGE orientations) and 2D PSIR LGE images for a patient with ischemic heart disease are shown in Fig.2. The 2D images show subendocardial LGE in basal inferior and inferoseptal walls (2/17 segments) which is also well depicted in the proposed 3D framework, showing good qualitative agreement between the two sequences.Discussion
This proof-of-concept study demonstrates the feasibility of an accelerated 3D whole-heart isotropic resolution, free-breathing, motion-compensated bright-blood PSIR LGE research sequence on a commercially available 0.55T scanner. The technique demonstrated good concordance with 2D PSIR LGE acquisitions in a scan duration of less than 10 minutes, reducing the risk of the T1 relaxivity of scar reaching equilibrium with healthy myocardium before image acquisition is completed. This work provides further evidence for the potential of using low-field CMR in routine clinical work. Future efforts will focus on further optimisation of the sequence for efficiency and acquiring data on a substantial cohort of patients with known myocardial scar.Acknowledgements
The authors acknowledge financial support from: (1) King’s BHF Centre for Award Excellence RE/18/2/34213, BHF PG/18/59/33955, RG/20/1/34802 and FS/CRTF/20/24011 (2) EPSRC EP/V044087/1, EP/P001009/1, EP/P032311/1, EP/P007619, (3) Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1), (4) Millennium Institute for Intelligent Healthcare Engineering ICN2021_004, FONDECYT 1210637 and 1210638, (5) IMPACT, Center of Interventional Medicine for Precision and Advanced Cellular Therapy, Santiago, Chile. ANID—Basal funding for Scientific and Technological Center of Excellence, IMPACT, #FB210024 (6) the Department of Health through the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award, (7) NIHR Cardiovascular MedTech Co-operative and (8) the Technical University of Munich – Institute for Advanced Study. The views expressed are those of the authors and not necessarily those of the BHF, NHS, the NIHR or the Department of Health.
References
1. Campbell-Washburn AE, Varghese J, Nayak KS, Ramasawmy R, Simonetti OP. Cardiac MRI at Low Field Strengths. Journal of Magnetic Resonance Imaging. 2023;n/a(n/a). doi:https://doi.org/10.1002/jmri.288902. Arnold TC, Freeman CW, Litt B, Stein JM. Low-field MRI: Clinical promise and challenges. Journal of Magnetic Resonance Imaging. 2023;57(1):25-44. doi:https://doi.org/10.1002/jmri.28408
3. Kelle S, Roes SD, Klein C, et al. Prognostic Value of Myocardial Infarct Size and Contractile Reserve Using Magnetic Resonance Imaging. J Am Coll Cardiol. 2009;54(19):1770-1777. doi:https://doi.org/10.1016/j.jacc.2009.07.027
4. Aquaro GD, De Gori C, Faggioni L, et al. Diagnostic and prognostic role of late gadolinium enhancement in cardiomyopathies. European Heart Journal Supplements. 2023;25(Supplement_C):C130-C136. doi:10.1093/eurheartjsupp/suad015
5. Perera D, Clayton T, O’Kane PD, et al. Percutaneous Revascularization for Ischemic Left Ventricular Dysfunction. New England Journal of Medicine. 2022;387(15):1351-1360. doi:10.1056/NEJMoa2206606
6. Velazquez EJ, Lee KL, Deja MA, et al. Coronary-Artery Bypass Surgery in Patients with Left Ventricular Dysfunction. New England Journal of Medicine. 2011;364(17):1607-1616. doi:10.1056/NEJMoa1100356
7. Garcia MJ, Kwong RY, Scherrer-Crosbie M, et al. State of the Art: Imaging for Myocardial Viability: A Scientific Statement From the American Heart Association. Circ Cardiovasc Imaging. 2020;13(7):e000053. doi:10.1161/HCI.0000000000000053
8. Choi KM, Kim RJ, Gubernikoff G, Vargas JD, Parker M, Judd RM. Transmural Extent of Acute Myocardial Infarction Predicts Long-Term Improvement in Contractile Function. Circulation. 2001;104(10):1101-1107. doi:10.1161/hc3501.096798
9. Milotta G, Munoz C, Kunze KP, et al. 3D whole-heart grey-blood late gadolinium enhancement cardiovascular magnetic resonance imaging. Journal of Cardiovascular Magnetic Resonance. 2021;23(1):62. doi:10.1186/s12968-021-00751-2
10. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary mra using golden-step Cartesian acquisition. Journal of Magnetic Resonance Imaging. 2015;41(3):738-746. doi:https://doi.org/10.1002/jmri.24602
11. Luo J, Addy NO, Ingle RR, et al. Nonrigid Motion Correction With 3D Image-Based Navigators for Coronary MR Angiography. Magn Reson Med. 2017;77(5):1884-1893. doi:https://doi.org/10.1002/mrm.26273
12. Bustin A, Rashid I, Cruz G, et al. 3D whole-heart isotropic sub-millimeter resolution coronary magnetic resonance angiography with non-rigid motion-compensated PROST. Journal of Cardiovascular Magnetic Resonance. 2020;22(1):24. doi:10.1186/s12968-020-00611-5
13. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement†. Magn Reson Med. 2002;47(2):372-383. doi:https://doi.org/10.1002/mrm.10051
14. Cerqueira MD, Weissman NJ, et al. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart. Circulation. 2002;105(4):539-542. doi:10.1161/hc0402.102975
Figures
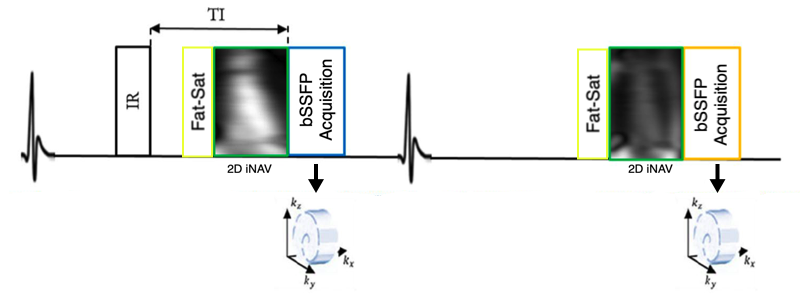
The iNAV-based PSIR 3D LGE research sequence at 0.55T consists of an ECG-triggered free-breathing bSSFP acquisition with interleaved IR-prepared and non-prepared acquisitions. Acquisition is performed with a 4.5-fold under-sampled variable-density Cartesian trajectory. 2D image navigators (iNAV) precede the 3D data acquisitions to enable non-rigid respiratory motion-corrected reconstruction. Prior to image acquisition fat-saturation pulses (FA = 180°) are used at each heartbeat to null epicardial fat and improve myocardial depiction.
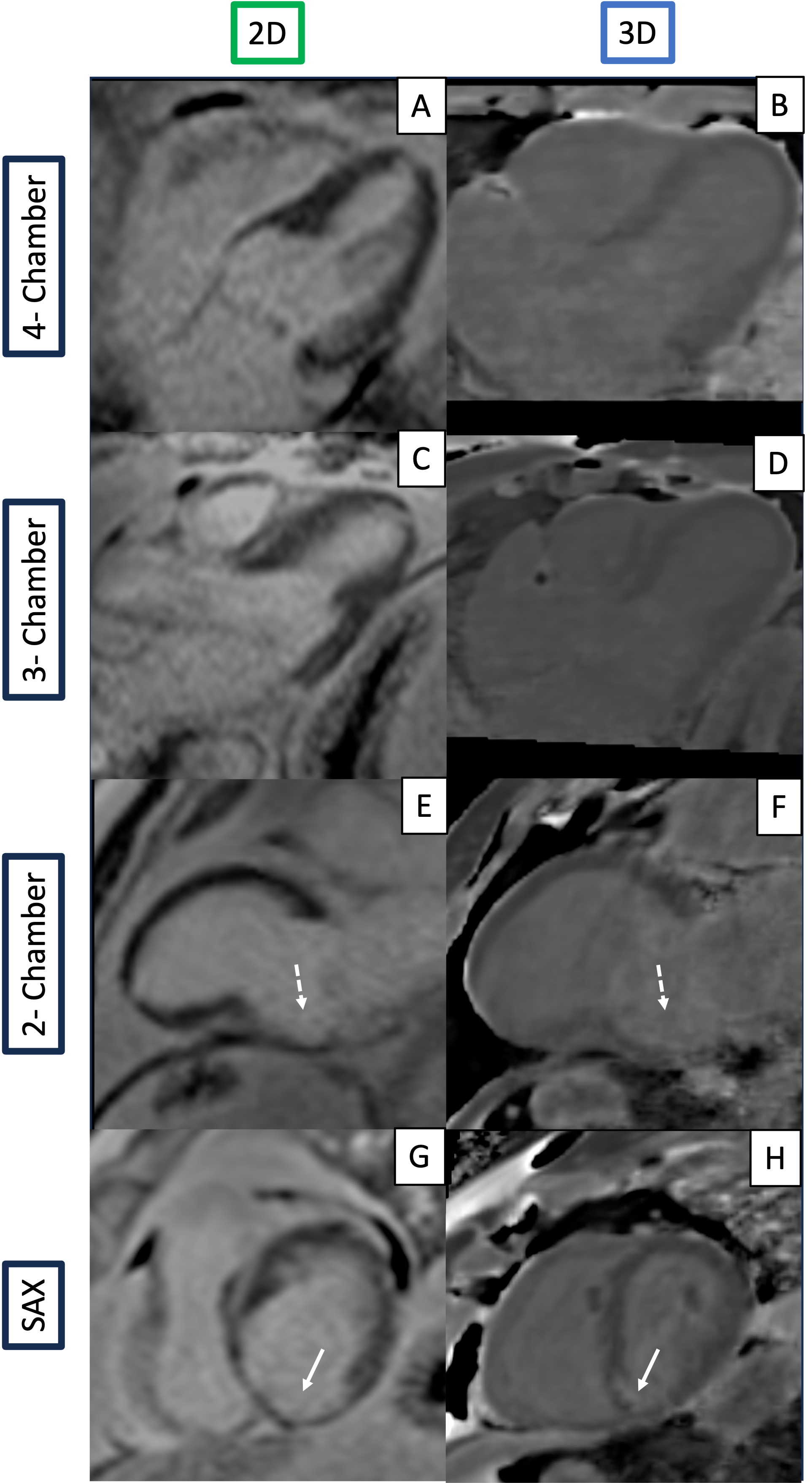
2D (left) and 3D whole-heart (right) LGE PSIR images acquired on a patient with ischaemic heart disease. Both the 2D and 3D show good agreement in depicting subendocardial LGE in the basal inferior and inferoseptal walls. A-B: 4-chamber views; C-D: 3-chamber views; E-F: 2-chamber views; short-axis (SAX) view. In the 2-chamber view, LGE is depicted in the basal inferior wall (dashed white arrows). In the SAX view, LGE is depicted in the inferior and inferoseptal walls (solid white arrows).