1497
Accelerating Free Breathing Motion-Corrected Late Gadolinium Enhancement Imaging Using Simultaneous Multi-Slice Imaging1King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 3Cardiovascular predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4MR Research Collaborations, Siemens Healthcare Limited, Melbourne, Australia, 5Department of Radiology, The University of Melbourne, , Melbourne, Australia, 6Royal Brompton Hospital, London, United Kingdom
Synopsis
Keywords: Myocardium, Heart, LGE
Motivation: Free breathing motion-corrected late gadolinium enhancement (FB-MOCO-LGE) is commonly used for scar assessment in patients unable to breathhold. Reduction of FB-MOCO-LGE scan time will contribute reducing overall examination time and cost.
Goal(s): To evaluate the potential of simultaneous multi-slice (SMS) imaging in reducing FB-MOCO-LGE acquisition time while maintaining image quality.
Approach: To Implement a 2x SMS-bSSFP technique with phase-sensitive inversion recovery (PSIR) reconstruction. Evaluation of FB-MOCO-LGE and SMS FB-MOCO-LGE was conducted on 20 patients.
Results: The SMS approach demonstrated a significant two-fold reduction in acquisition time without compromising myocardial sharpness or signal-to-noise ratio and minimal impact on image quality.
Impact: SMS-enabled FB-MOCO-LGE enables halves acquisition time with minimal on image quality. Therefore, this approach show promise for reducing LGE protocol duration and cost of cardiac MRI examination.
Background
Late Gadolinium Enhancement (LGE) MRI is the gold standard for imaging of myocardial scar and fibrosis. LGE-MRI is commonly performed using a 2D imaging technique, where each slice of the left ventricular stack is acquired in one breath hold. Free breathing motion corrected and averaged LGE (FB-MOCO-LGE) MRI is an alternative clinical solution for patients unable to breath hold (1, 2). It is based on the repeated ECG-triggered acquisition of the same slice, which are then co-registered and averaged for enhanced quality. Reducing the scan time of these protocols is of great importance to minimize cost, facilitate adoption and allow higher patient throughput (3). In this study, we sought to evaluate the potential of simultaneous multi-slice (SMS) imaging for accelerated FB-MOCO-LGE protocol.Methods
A research sequence with SMS balanced steady-state free precession (bSSFP) with GC-LOLA banding correction and a ‘lean’ implementation for slice separation (4) was implemented into a FB-MOCO-LGE protocol with PSIR reconstruction (5). A multiband factor of two was implemented to provide a two-fold net acceleration of this protocol. Eight averages were acquired. The two most dissimilar images based on center of mass were first discarded and the remaining 6 images were co-registered and averaged. All imaging was conducted on a 1.5 T MRI scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen Germany). Twenty patients (12 male and 8 female, mean age: 57±18 years old) referred for clinical CMR were recruited. Both standard FB-MOCO-PSIR-LGE and proposed SMS FB-MOCO-PSIR-LGE sequences were acquired in randomized order across subjects. A stack of 16 slices were prescribed in the short-axis orientation to achieve full left ventricular coverage without slice gaps under free breathing conditions and the following imaging parameters: TR/TE: 2.71ms/1.15ms, flip angle: 45°, FOV: 380×380mm2, acquired resolution: 1.48x1.98mm2, slice thickness: 8mm, in- acceleration factor: 2.5, bandwidth: 1085Hz/px. To accommodate larger patients the FOV was adjusted up to max. 450mm depending on a patient. Quantitative assessments of myocardial sharpness and blood signal-to-noise ratio (SNR) as well as qualitative assessment of image quality (1:poor, 2:major artefacts, 3:minor artefacts, 4:excellent) by two independent readers blinded from patient information and imaging techniques were performed.Results
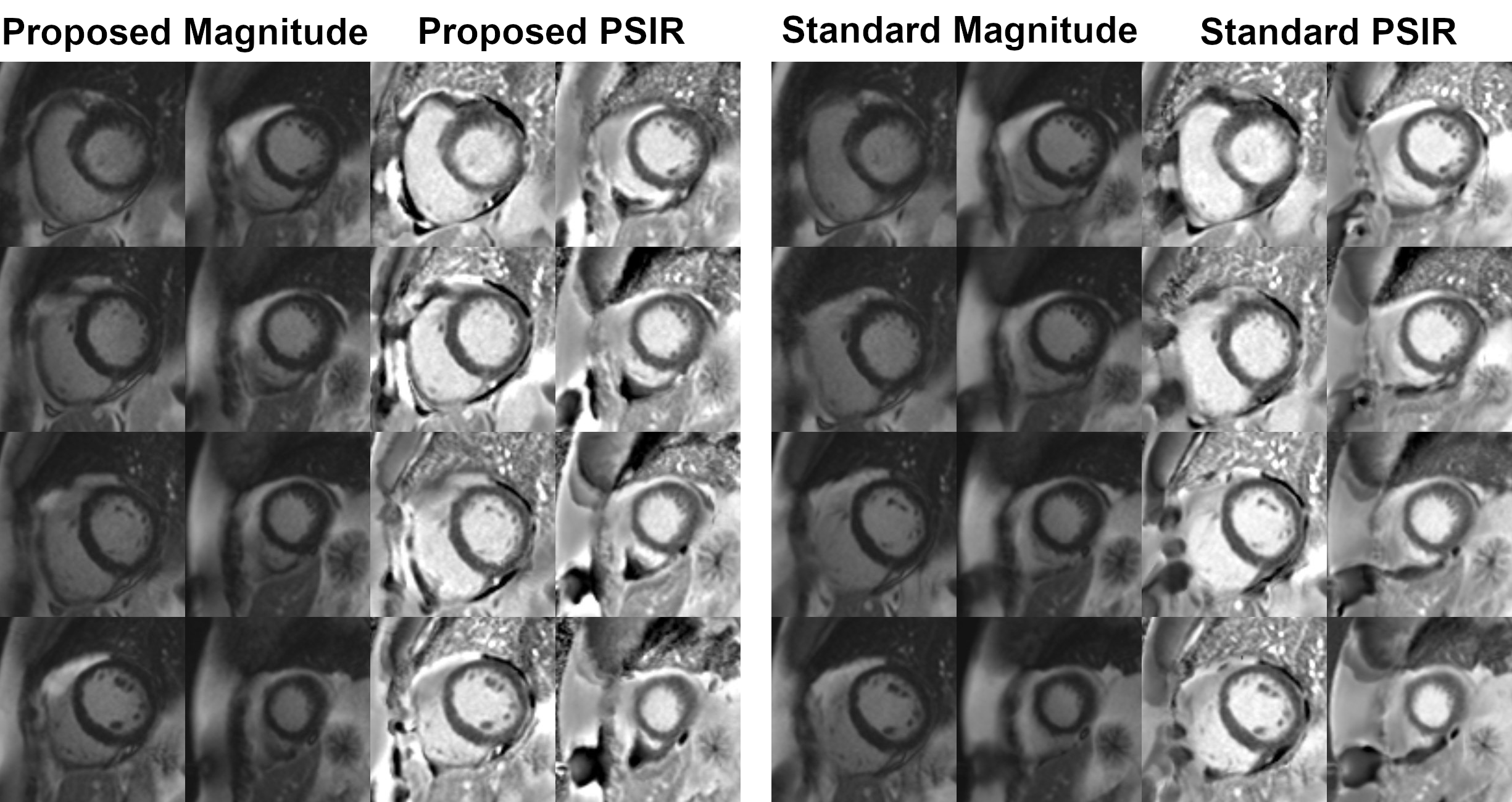
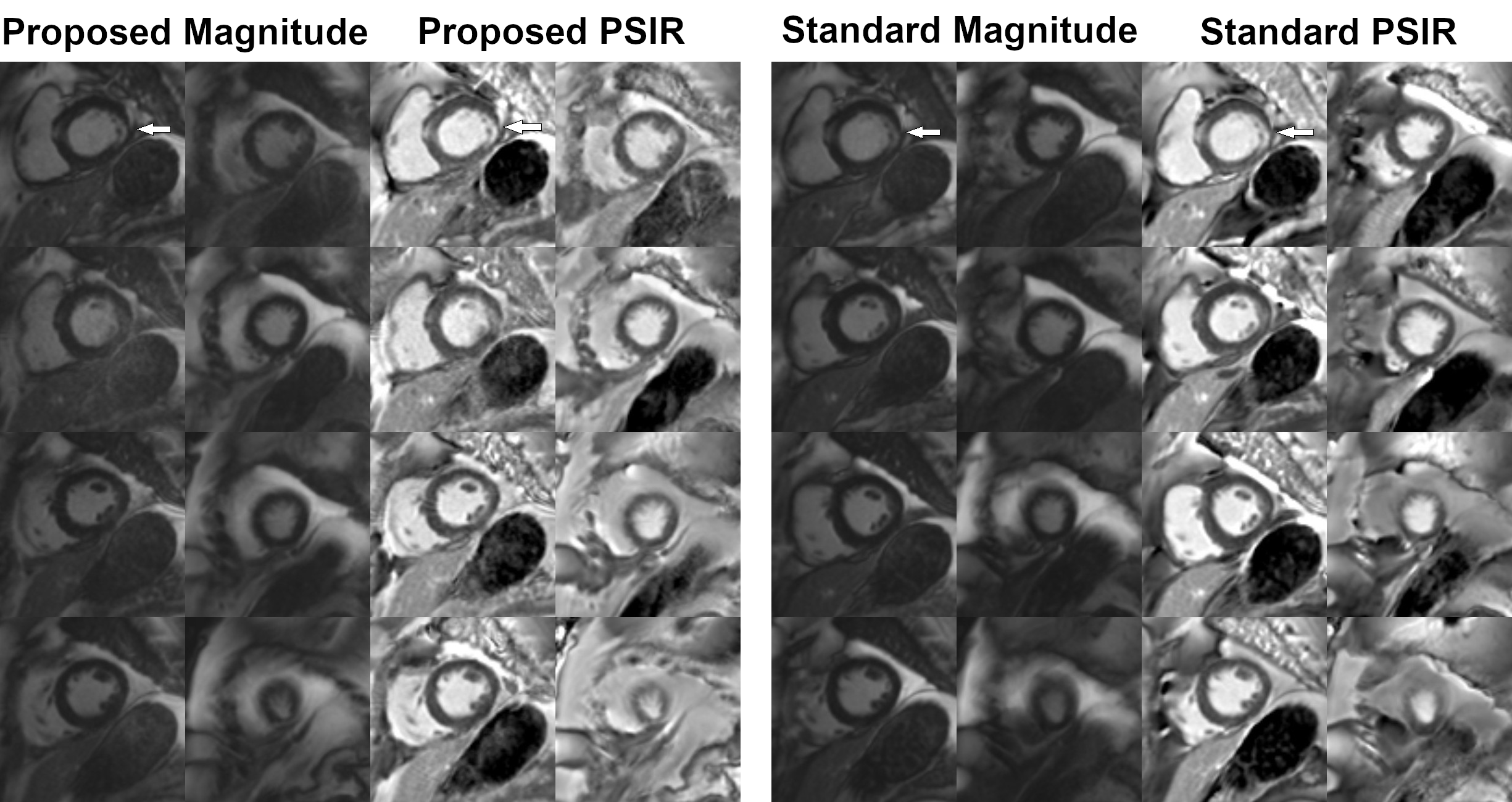
Fig. 1 and 2 show representative images acquired with both sequences in two patients. Similar image quality can be observed between the two techniques. Over all patients, the proposed approach resulted in a two-fold reduction of acquisition time (proposed: 1.8±0.3min, standard: 3.9±1.2min, p<0.001). There were no statistically significant differences between the proposed and standard approaches in terms of myocardial sharpness (0.39±0.07 vs. 0.37±0.07 p=0.45) and blood SNR (34.3±24.9 vs. 31.3±24.1 p = 0.24). The image quality assessment showed good to excellent image scores with no statistical significance for Reader 1 (3.44±0.28 vs. 3.49±0.21 p=0.22) and trending to statistically significant difference for Reader 2 (3.77±0.33 vs. 3.84±0.30 p=0.05) between proposed and standard techniques respectively.Discussion
The proposed SMS approach halved acquisition time while preserving myocardial sharpness and SNR. The increased standard deviation in the total acquisition time of FB-MOCO-LGE is explained by the single case where patient’s heart rate changed during the scan resulting in miss-triggering. While no difference in image quality was observed from the first reader, the score from the second reader were near statistical significance threshold. However, this potential difference in image quality was of very small amplitude and both approaches resulted in good to excellent image quality. Therefore, this technique has strong clinical potential which will need to be confirmed in larger studies. The use of a higher multiband factor in the proposed sequence has the potential to provide further data acquisition acceleration. Higher spatial resolution may also be feasible if combined with more advanced reconstruction techniques.Conclusion
SMS FB-MOCO-PSIR-LGE was successfully developed and results in a two-fold reduction of scan time with no differences in myocardial sharpness, SNR and minimal impact on image quality, in comparison to clinical standard FB-MOCO-PSIR-LGE. Further investigations are warranted to validate its performance across varied conditions.Acknowledgements
No acknowledgement found.References
[1] Ledesma-Carbayo MJ, Kellman P, Hsu LY, Arai AE, McVeigh ER. Motion corrected free-breathing delayed-enhancement imaging of myocardial infarction using nonrigid registration. J Magn Reson Imaging. 2007;26:184–190. [2] Piehler KM, Wong TC, Puntil KS, Zareba KM, Lin K, Harris DM, et al. Free-breathing, motion-corrected late gadolinium enhancement is robust and extends risk stratification to vulnerable patients. Circ Cardiovasc Imaging. 2013;6:423–32. [3] Plein S., Kozerke S.Are We There Yet?: The Road to Routine Rapid CMR Imaging, JACC: Cardiovascular Imaging. 2021;14(9):1755-1757 [4] Stab D, Speier P. Gradient-controlled local Larmor adjustment (GC-LOLA) for simultaneous multislice bSSFP imaging with improved banding behavior. Magn Reson Med. 2019; 81: 129-139. [5] Ledesma-Carbayo MJ, Kellman P, Hsu L-Y, Arai AE, McVeigh ER. Motion corrected free-breathing delayed-enhancement imaging of myocardial infarction using nonrigid registration. J. Magn. Reson. Imaging. 2007;26:184–90.Figures