1495
Myocardial cine T1 mapping using dynamic multiple trigger delay acquisition1Department of Radiological Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
Keywords: Myocardium, Cardiomyopathy, myocardium/T1Mapping
Motivation: Myocardial T1-mapping is a widely used quantitative method to evaluate the characteristics of myocardium. Commonly, the cardiac trigger delay (TD) during the diastolic phase depends on the settings of the system. However, because myocardial characteristics can affect both diastole and systole, acquiring T1 mapping at various cardiac phases may have clinical significance.
Goal(s): To acquire cardiac T1 mapping at various cardiac phases in one scan.
Approach: Dynamic trigger delay
Results: The proposed technique was successfully implemented. Application of image registration technique has improved the accuracy of T1 value quanitification.
Impact: CINE T1 mapping can acquire quantitative mapping of several different cardiac phases simultaneously in one scan; it may be useful for more detailed diagnosis of myocardial properties.
Introduction
Quantitative myocardial T1 mapping enables sensitive detection of myocardial lipid and iron deposition and myocardial edema using native T1, as well as quantitative evaluation of myocardial extracellular volume expansion due to diffuse fibrosis and amyloid deposition using ECV [1]. Generally, myocardial T1 mapping is acquired during the diastolic phase and the trigger delay (TD) used depends on the settings of the system. However, previous studies reported that normal myocardial T1 values can vary between the diastolic and systolic phases [2, 3]. Acquisition of T1 mapping at multiple cardiac phases (diastolic and systolic, at least), could be clinically useful to accurately assess diffuse myocardial pathologies. Conventionally, separate scans were required to obtain T1 mapping at diastolic and systolic phases. In this study, we proposed a new T1 mapping technique called CINE T1 mapping. Similarly as CINE imaging, this technique allows simultaneous acquisition of T1 maps at several different cardiac phases including diastolic and systolic phases by utilizing Dynamic Trigger Delay (DynTD).Methods
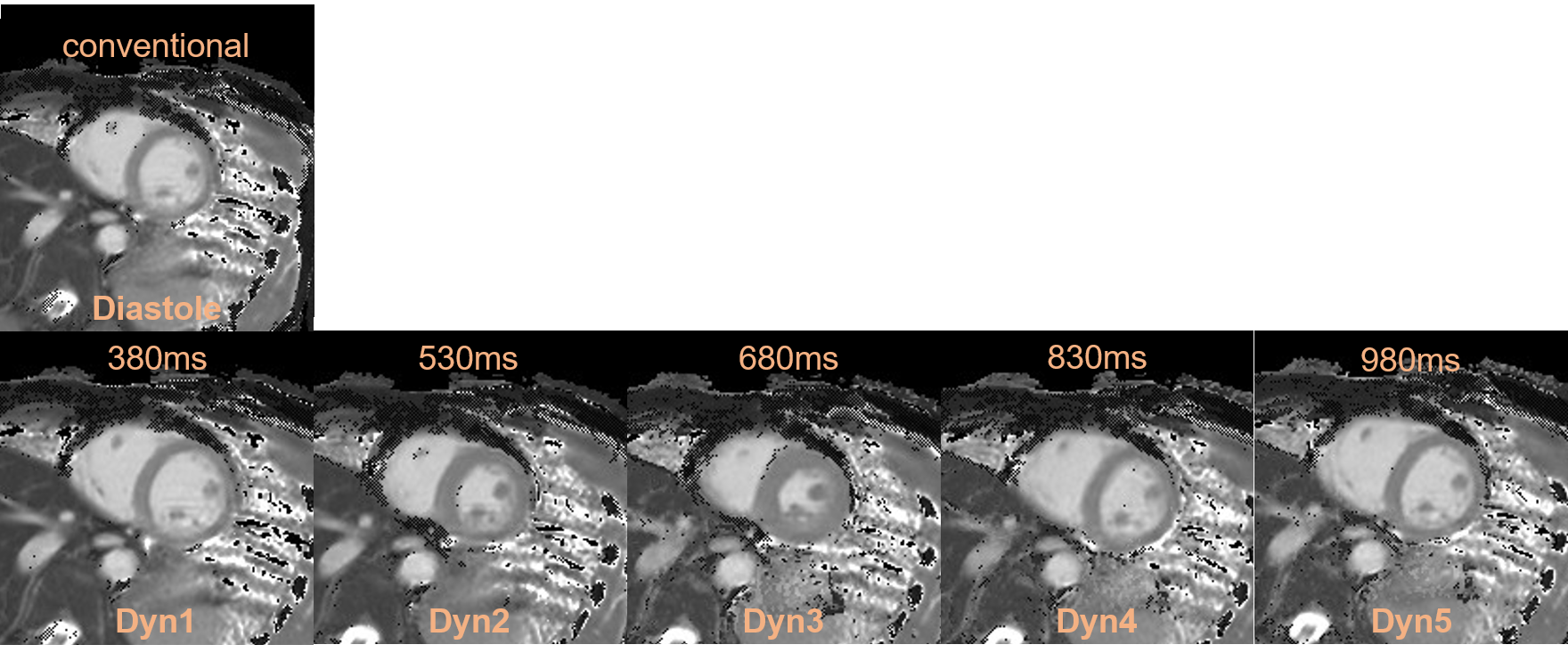
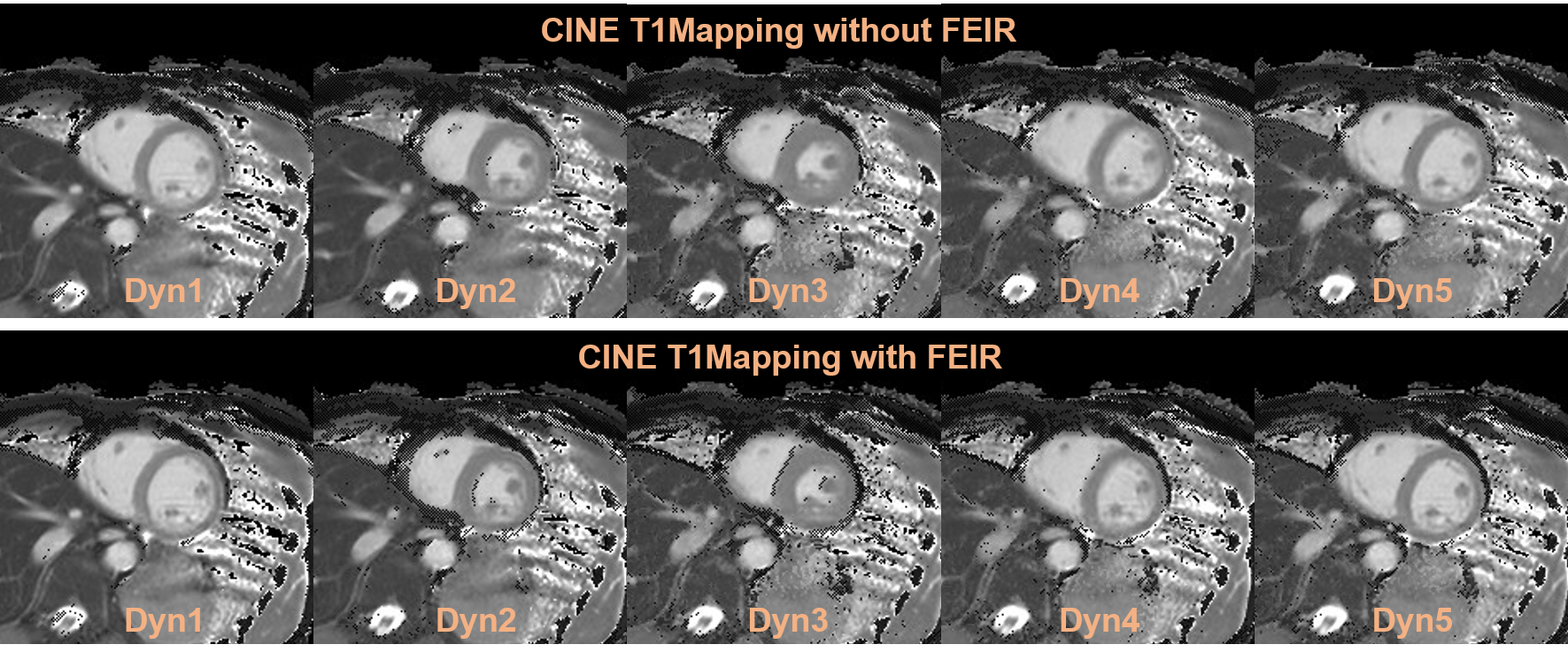
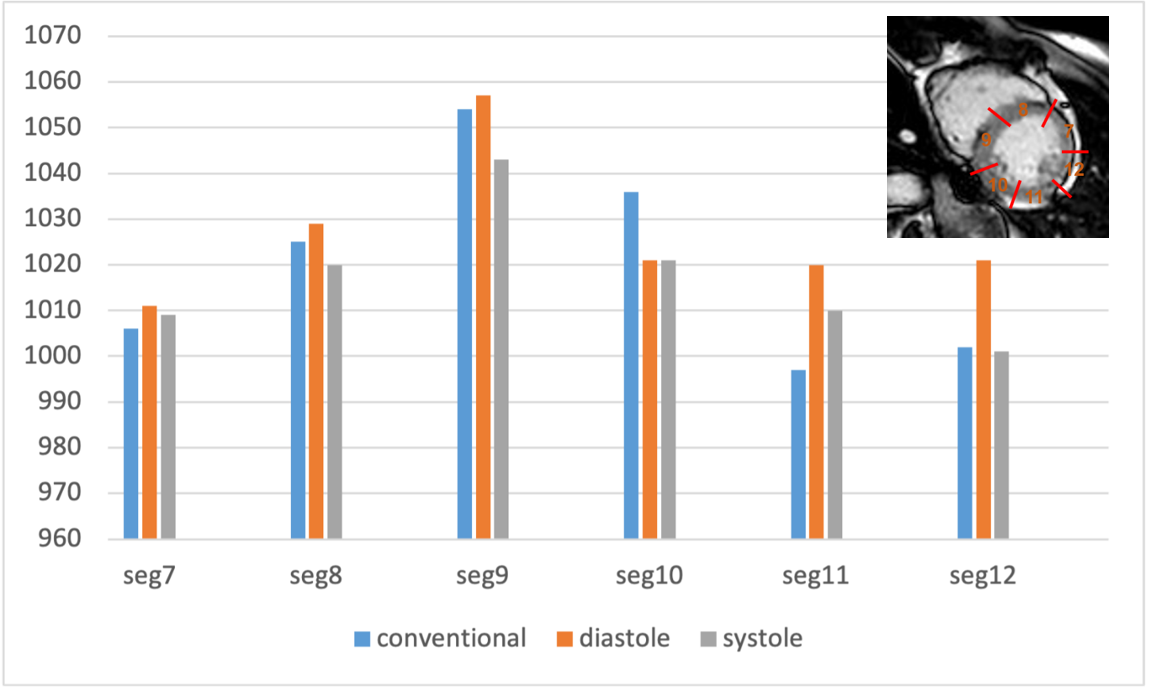
A total of five volunteers were examined on a 1.5T system (Ingenia CX Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. We compared two procedures in respective T1 Map acquisition: is conventional approach (operator set the preset TD timing for diastole and TD was automatically determined by MR system software) and visual approach using MoSE-CINE (operator visually defined the diastolic phase as the TD where the heart structure is not obscured by cardiac movements) [4]. DynTD was combined with the dynamic scan procedure, but the scan parameters (including TR, TE, number of slices, etc.) of each scan were the same. TD only increased with the number of dynamic scans, and the TD increment (ms/dyn) can be determined arbitrarily. Consequently, DynTD can acquire images of multiple different time-phase images in one scan [5]. To minimize motion-induced misalignment, fast elastic image registration (FEIR) [6] [7] was used for motion correction. FEIR registers the source images before generating the parametric map and has been reported to be able to correct in-plane miss-registration in the heart [8]. Regions of interest (ROI) were placed in the middle myocardium in the 6 regions (seg7 to seg12) of the AHA classification of the short-axis image of the left ventricle, and the T1 value and standard deviation (SD) of relaxation time in each ROI were calculated across all datasets [9]. Imaging-parameters; 2D-ssh-TFE with DynTD (CINE-T1-mapping): FOV=300×300mm, voxel-size=2.0×2.0×8.0mm, TR/TE=2.2/1.0ms, flip-angle=35, TFE-factor=50, TFE shot interval=1 heartbeat, C-SENSE factor=3, and acquisition time=12 sec×5 times (depend on the heart rate).Results and Discussion
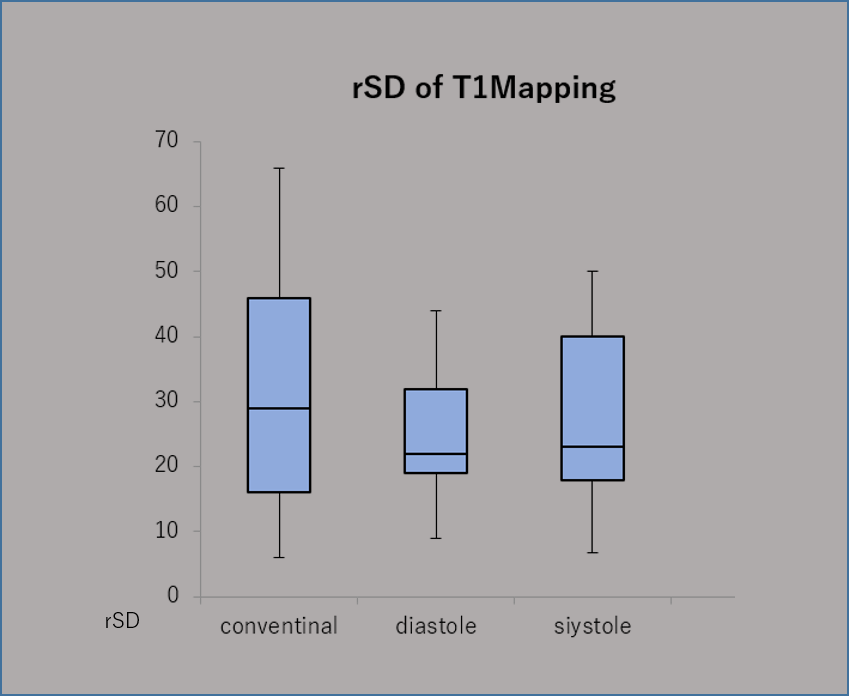
Figure 1 shows representative source images of CINE-T1-mapping that were acquired by DynTD. Figure 2 shows the T1 map with multiple cardiac phases embedded. Figure 3 shows the comparison MOLLI T1mapping confidence map with/without FEIR applied. FEIR clearly improved the accuracy of T1 mapping. Figure 4 shows the comparison of myocardial T1 value values in short-axis (SA) between conventional method at diastole (blue) and CINE-T1-mapping at diastole (orange) and systole (gray). The bar shows the average T1 relaxation time for all volunteers in each sequence. Figure 5 shows the rSD(Variation in T1 value)of 6-segment ROI. rSD of CINE-T1-mapping at diastole was smaller than that of conventional method.Conclusion
We demonstrated the feasibility of CINE-T1 mapping to simultaneously acquire several different cardiac phases, including diastolic and systolic, in a single scan within a clinically acceptable scan time. Simultaneous acquisition of diastolic and systolic T1 maps may potentially enable more detailed diagnosis of myocardial properties. More systematic studies are needed to study its clinical robustness and accuracy of quantification compared to conventional techniques.Acknowledgements
No acknowledgements found.References
[1]. Hamlin SA, et.al. Mapping the future of cardiac MR imaging: case-based review of T1 and T2 mapping techniques. Radiographics. 2014 Oct; 34(6):1594-611. [2]. Kawel et al.: T1 mapping of the myocardium: Intra-individual assessment of the effect of field strength, cardiac cycle and variation by myocardial region. Journal of Cardiovascular Magnetic Resonance 2012 14:27. [3]. Reiter et al. Normal Diastolic and Systolic Myocardial T1 Values at 1.5T-MR Imaging:Correlations and Blood Normalization Radiology 271 2014 May [4]. Isao S, et al, Motion-Sensitive (MoSe) CINE imaging: utility for improving robustness of myocardial quantitative mapping. Proc. ISMRM:2020.2061 [5]. Mana K, et al. Rapid multiple breath-hold myocardial cine T2mapping with dynamic multiple trigger delay acquisition. Proc. ISMRM:2021. [6]. Kabus S, et al. Fast elastic image registration. Proc. MICCAI:2010. 81–89. [7]. Zhang S, et al. Cardiac magnetic resonance T1 and extracellular volume mapping with motion correction and co-registration based on fast elastic image registration. MAGMA. 2018 Feb;31(1):115-129. [8]. Takumi O, et al. Minimizing motion artifacts in myocardial quantitative mapping by combined use of motion-sensitive CINE imaging and FEIR. Proc. ISMRM:2021. [9]. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation,105:539-42,2002.Figures