1494
Diagnosing LGE-negative hypertrophic cardiomyopathy with T1 mapping and feature tracking: a preliminary study1Baoji Central Hospital, Baoji, China, 2The First Affiliated Hospital of Xinjiang Medical University, urumchi, China, 3Baoji Hospital of Traditional Chinese Medicine, Baoji, China, 4GE HealthCare MR Research, Beijing, China
Synopsis
Keywords: Myocardium, Quantitative Imaging, HCM
Motivation: The presence of myocardial fibrosis in HCM has significant prognostic power in the prediction of severe cardiac complications in HCM.
Goal(s): To compare native T1、ECV and myocardial strain parameters in patients with LGE-negative HCM with healthy participants to evaluate for the presence of subtle myocardial fibrosis and regional myocardial function in HCM.
Approach: Seventeen patients with LGE-negative HCM and twenty-eight healthy participants were underwent the MRI scan and the quantitative parameters were analyzed.
Results: Overall native T1 and ECV values were increased in HCM patients ; GLS, GRS, and GCS were all decreased in HCM patients with LGE negative.
Impact: The cardiac magnetic resonance T1 mapping technique combined with the feature tracking technique can reflect subtle myocardial fibrosis, myocardial deformation, and impaired myocardial systolic function earlier in HCM patients from LGE negative patients.
Introduction
Hypertrophic cardiomyopathy (HCM) is the most prevalent inherited primary cardiomyopathy, affecting approximately one in 500 individuals. Conventional late gadolinium enhancement (LGE) techniques can identify regional variations in myocardial contrast enhancement compared to unaffected myocardium. However, they face challenges in detecting subtle diffuse myocardial enhancement. Native myocardial T1 mapping allows for the calculation of absolute T1 values of the myocardium and the myocardial extracellular volume (ECV) fraction. This approach is instrumental in identifying the presence of myocardial interstitial fibrosis. Our study aims to investigate the diagnostic and prognostic potential of cardiac magnetic resonance T1 mapping combined with feature tracking (CMR-FT) techniques for quantitative analysis of myocardial fibrosis and myocardial deformation in patients diagnosed with LGE-negative hypertrophic cardiomyopathy (HCM).Methods
This study was approved by Ethics Committee and all patients and healthy volunteers signed informed consent. From June 2021 to January 2023, 17 patients (9 males and 8 females) clinically diagnosed with HCM and LGE negative were prospectively enrolled in our study as case group. Meanwhile, a total 28 matched healthy volunteers were included as control group. Both groups underwent cardiac MR examination with a 3T scanner equipped with 16 channel cardiac coil. Scan sequence include black blood, steady-state free precession (SSFP) cine images of standard short axis-slice,long-axis, 2-chamber, 3-chamber, 4-chamber views, and native modified Look-Locker inversion recovery (MOLLI) T1 mapping . The detailed sequence parameters for T1 mapping and Cardiac cine are as follows: (a)T1 mapping: 3 different short axis slice(the base, midchamber, and apex) TR/TE2.2/1.8 ms, flip angle:20 degree, Field of View: 300*300 mm,matrix 152 × 150 and slice thickness 10 mm; (b)CINE: TR/TE: 2.3/1.02 ms, Flip angle: 20 degree, Field of View: 300*300 mm, Acqiostion matrix: 152*150, layer thickness: 8 mm, layer spacing: 2 mm. After scan, all CMR images were transferred to a post-processing workstation for analysis with CVI42 v5.14 (Circle Cardiovascular Imaging, Canada). Image markers inclduing left ventricular ejection fraction (LVEF), Global native T1, T2, Global ECV, global longitudinal strain (GLS), global circumferential strain (GCS), and global radial strain (GRS) were calculated and compared between the two groups (Figure 1). Diagnostic efficacy was evaluated with receiver operating characteristic (ROC). Statistical analysis was performed with SPSS 26.0 software, where p<0.05 was considered to be significant.Results
In comparison to the control group, the HCM group exhibited the following findings: (1) a significant reduction in LVEF (p=0.003) and an increase in systolic/diastolic myocardial mass (p=0.001), as illustrated in Table 1; (2) notable increases in left ventricular global, basal base, apical native T1, ECV, and middle T1 values in the HCM group (p<0.05), as presented in Table 2; (3) a marked reduction in the peak values of GCS, GRS, and GLS within the HCM group, with statistically significant differences (p<0.05), as outlined in Table 3. The diagnostic performance of the global ECV value, characterized by an area under the curve (AUC) of 0.812, sensitivity of 0.818, specificity of 0.727, and a Youden index of 0.545, was found to be the most efficient (p<0.05), as indicated in Table 4 and Figure 2.Discussion
In LGE-negative HCM patients, our findings revealed elevated overall, basal, intermediate, and apical native T1 values, as well as overall, basal, and apical ECV values, in comparison to the control group. However, there were no statistically significant differences in the overall, basal, intermediate, and apical T2 values and the intermediate ECV values when compared to the normal control group. These results indicate the presence of varying degrees of diffuse fibrosis in LGE-negative HCM patients. Previous studies have primarily associated a decrease in GLS, GRS, and GCS with LGE-positivity, emphasizing left ventricular (LV) fibrosis as a robust predictor of adverse cardiovascular events. Nonetheless, limited research has focused on patients with LGE-negative HCM. In our current study, we observed reductions in the peak values of GLS, GCS, and GRS among LGE-negative HCM patients. This highlights the potential for early ventricular dysfunction detection through CMR-FT, underscoring the value of CMR-FT in identifying preclinical LV dysfunction. Therefore, LV myocardial strain, as assessed by CMR-FT, proves to be a sensitive indicator of preclinical LV dysfunction.Conclusion
LGE-negative patients with HCM had elevated overall, basal, intermediate, and apical native T1 values and ECV values, suggesting that diffuse fibrosis exists to varying degrees in patients with HCM; Additionally, LGE-negative patients with HCM had decreased GLS, GRS, and GCS, suggesting that CMR ⁃FT technology can reflect myocardial morphology and impaired systolic function at an earlier stage.Acknowledgements
No acknowledgement found.References
Xu J, Zhuang B, Sirajuddin A, Li S, Huang J, Yin G, Song L, Jiang Y, Zhao S, Lu M. MRI T1 Mapping in Hypertrophic Cardiomyopathy: Evaluation in Patients Without Late Gadolinium Enhancement and Hemodynamic Obstruction. Radiology. 2020 Feb;294(2):275-286. doi: 10.1148/radiol.2019190651. Epub 2019 Nov 26. PMID: 31769741; PMCID: PMC6996717.
Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, Mascherbauer J, Nezafat R, Salerno M, Schelbert EB, Taylor AJ, Thompson R, Ugander M, van Heeswijk RB, Friedrich MG. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson. 2017 Oct 9;19(1):75. doi: 10.1186/s12968-017-0389-8. Erratum in: J Cardiovasc Magn Reson. 2018 Feb 7;20(1):9. PMID: 28992817; PMCID: PMC5633041.
Figures
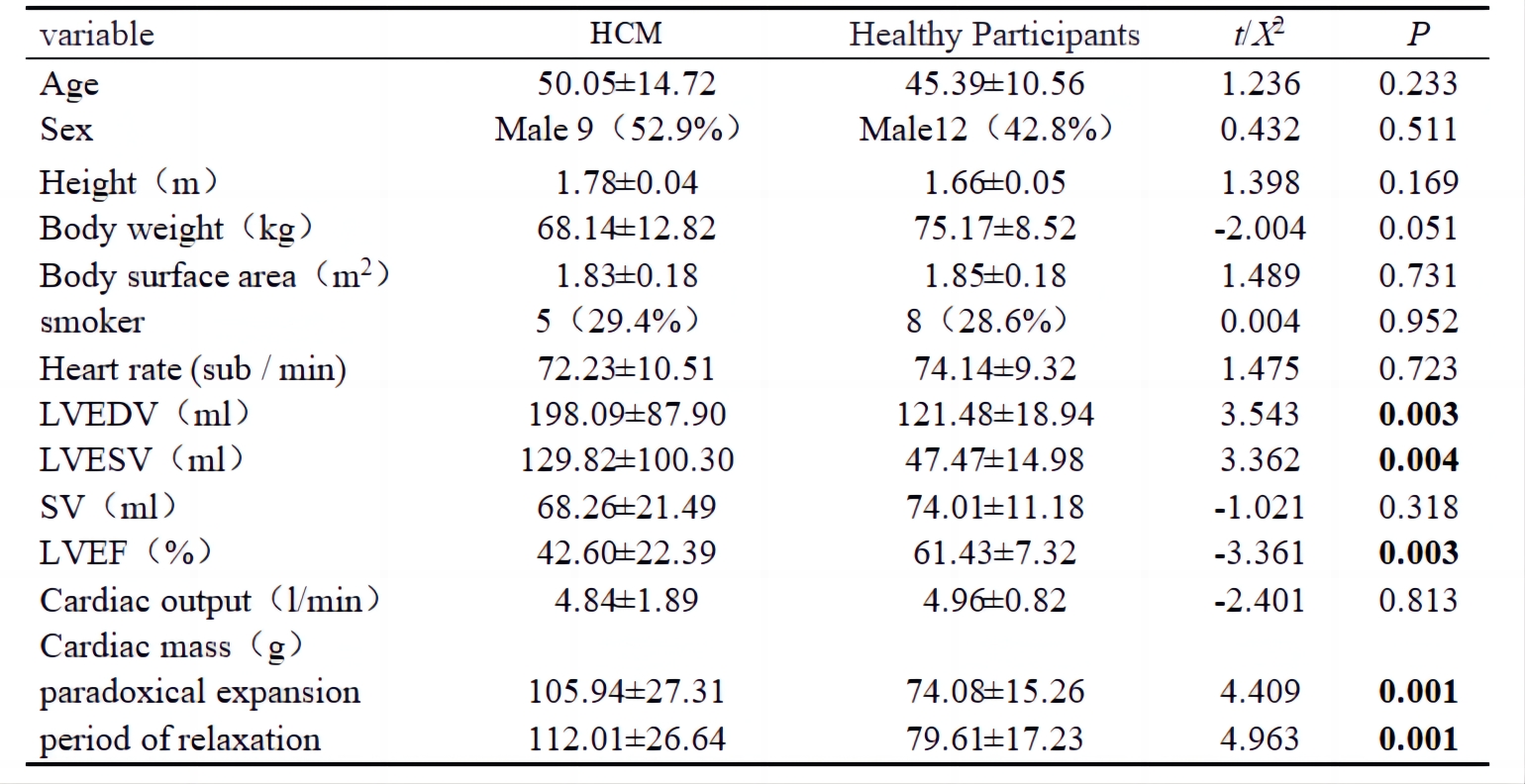
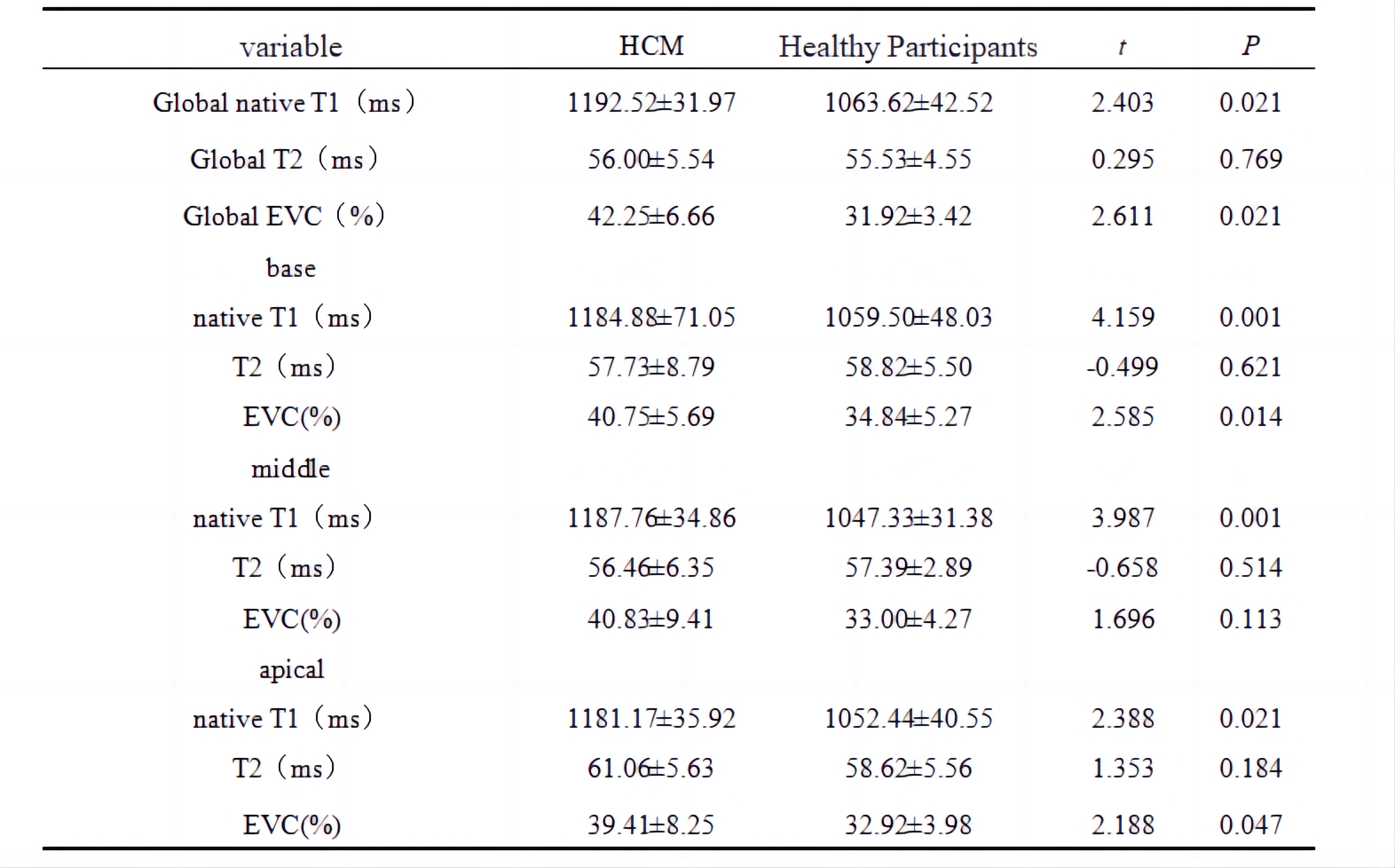

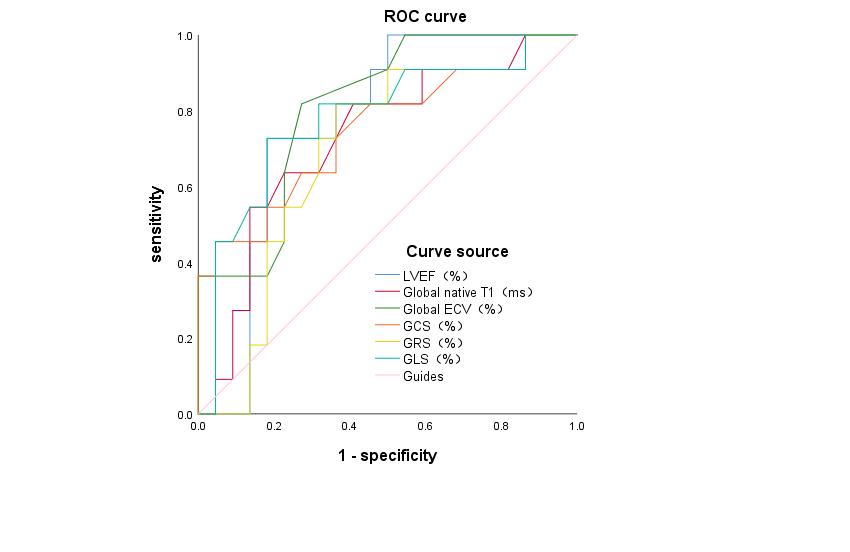
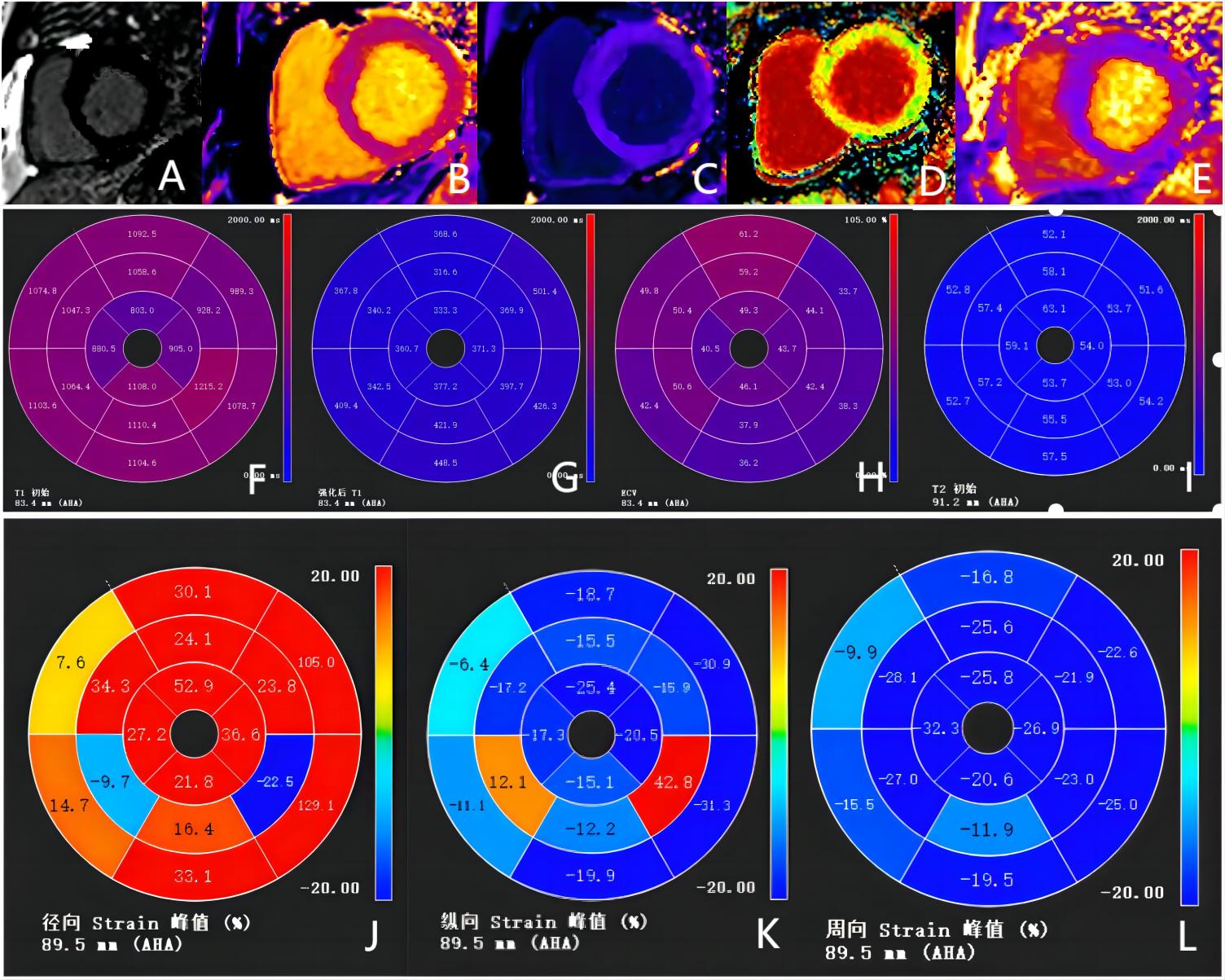
Figure 1: Imaging of a typical case (46-year-old HCM man with LGE negative )
A~E are LGE figures, native T1, enhanced T1, ECV, and T2 pseudo-color maps
F~I is the 16-segment bull's eye diagram of native T1, enhanced T1, ECV, and T2
J~L is the 16-segment bull's eye diagram of GRS, GLS and GCS.