1491
A self-supervised motion-correction approach for cardiac T1 mapping1School of Medical Technology, Beijing Institute of Technology, Beijing, China, 2School of Life Science, Beijing Institute of Technology, Beijing, China, 3Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China
Synopsis
Keywords: Myocardium, Myocardium
Motivation: Deep-learning algorithm has the potential to alleviate the impaction from motion in myocardial T1 mapping. However, there is no ground truth for the training.
Goal(s): The aim of this study is to develop a deep learning-based algorithm to correct motion in myocardial T1 mapping using a self-supervised manner.
Approach: We proposed a deep-learning approach and trained it using synthesized reference from the input T1-weighted images, eliminating the need for ground truth.
Results: Our results indicated that a self-supervised deep-learning approach could align the left-ventricle myocardium and therefore improve the T1 map quaintly and accuracy.
Impact: A self-supervised deep-learning approach could automatically perform motion correction for cardiovascular magnetic resonance T1 mapping, alleviating the impaction from motion and improving the quality of pixel-wise T1 map.
Introduction
Cardiovascular magnetic resonance T1 mapping technique has high sensitivity in detecting abnormalities in myocardium tissue, such as fibrosis1. T1 mapping generally acquires several different T1-weighted images under breath-holding. Each image is trigged using ECG and acquired at the same cardiac phase. Therefore, T1 at each pixel reveals the property of the corresponding voxel. However, changes in heart rate, non-compliance, or inadequate breathing holding will result in the mismatch of left-ventricle myocardium across images, leading to T1 estimation error and confusing application.Several algorithms have been proposed to alleviate the impaction from the misregistration of T1-weighted images2-4. However, the robustness, accuracy, and efficiency of these methods are compromised by the change in contrast of myocardium among images, partial volume, and artifacts. Besides, some methods need manual initialization4. In addition, the supervised deep learning-based method requires ground truth. Therefore, there is still a need to develop unsupervised, robust, and automatic approaches for myocardial T1 mapping to alleviate motion impaction.
In this study, we proposed a self-supervised deep-learning approach for the motion correction in myocardial T1 mapping.
Methods
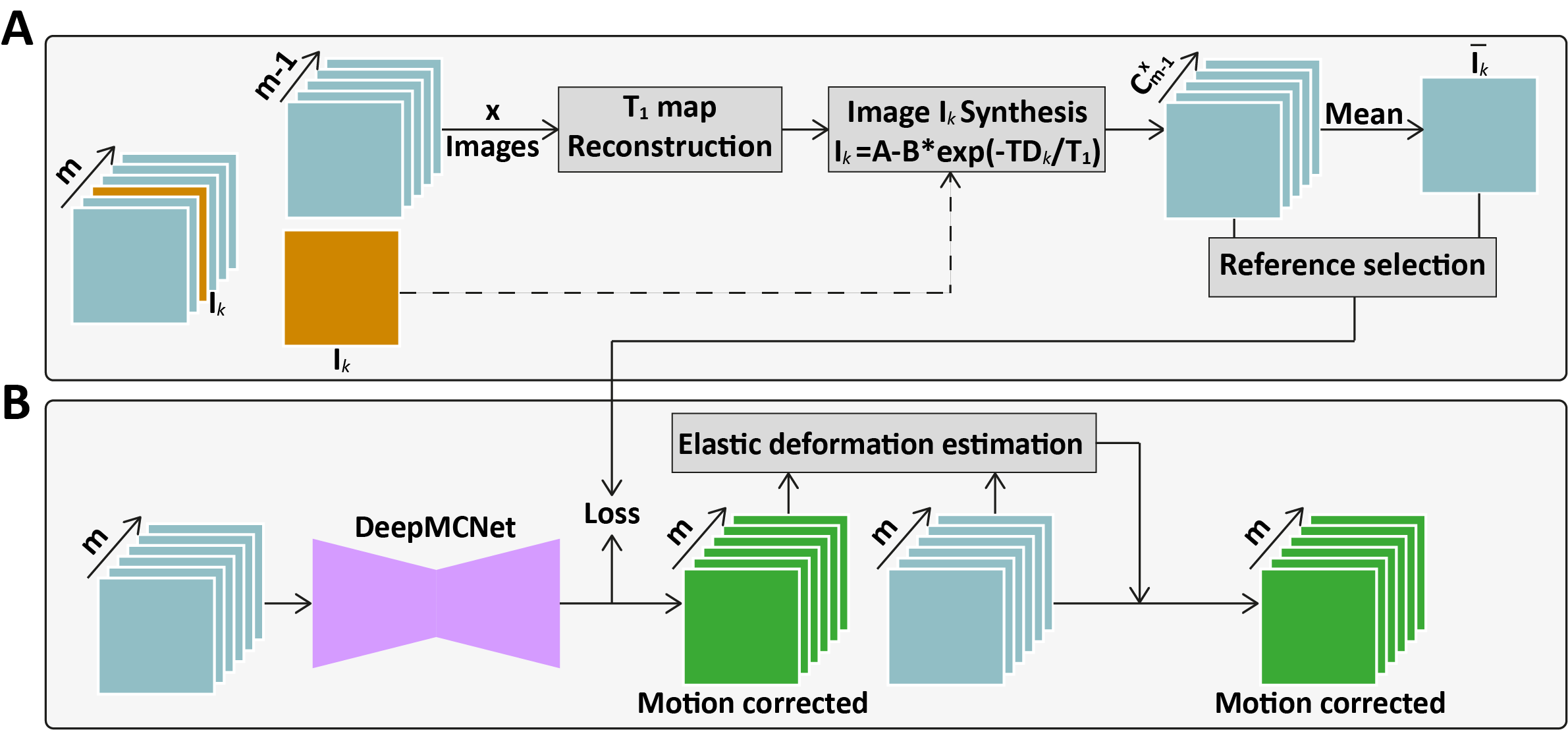
A publicly available T1 mapping dataset was used2, which included data of 210 patients (134 males; age 57 ± 14 years). All images were collected on a 1.5T scanner using a free-breathing sequence5. Each patient was imaged with 5 slices. T1 mapping of each slice has 10 inversion-recovery T1-weighted images from two inversion-recovery experiments and one at the M0. We used ten inversion-recovery images to simulate two MOLLI5(3)3 T1 mapping scans. We split the dataset into 80% for training, 20% for validation, and 20% for testing.For each MOLLI5(3)3 with $$$m$$$ images, leave-one-out strategy was used to generate $$$m$$$ motion-free images for the reference in training. As shown in Figure 1A, we used $$$m-1$$$ images without $$$I_k$$$ to calculate A, B, and T1 maps using $$$I_j=A+B*exp(-\frac{TDj}{T_1})$$$. Then, A, B, and T1 maps with the delay time of $$$I_k$$$ are used to generate $$$I_k^{ref}$$$, which means $$$I_k^{ref}$$$ would match well with other images. In addition, in order to reduce the impaction from the motion in other images, we used $$$x$$$ of the $$$m-1$$$ images to generate $$$I_{k,i}^{ref,x}$$$ ($$$x\geq4$$$). Totally, $$$C_{m-1}^x$$$ references for $$$I_k$$$ have been generated. A mean $$$\overline{I_k^{ref,x}}$$$ is calculated and used to select the best reference for $$$I_k$$$. The variation between $$$I_{k,j}^{ref,x}$$$ and $$$\overline{I_k^{ref,x}}$$$ is calculated using below equation.
$$$Var_j={\lambda}{L_1}(I_{k,i}^{ref,x},\overline{I_k^{ref,x}})+{\mu}(1-SSIM(I_{k,i}^{ref,x},\overline{I_k^{ref,x}}))$$$
$$$I_{k,j}^{ref,x}$$$ with lowest variation against $$$\overline{I_k^{ref,x}}$$$is picked.
We employed a U-shaped conventional neural network (DeepMCNet) to generate the motion-resolved images $$$I_k^{net}$$$ for input $$$I_k$$$ (Figure 1B). To improve the robustness, an elastic displacement vector field estimation algorithm was used to generate the DVF between $$$I_k^{net}$$$ and input $$$I_k$$$. Then the DVF is applied to $$$I_k$$$ for motion correction.
DeepMCNet was implemented on a DELL 7920 Server with one Quadro RTX 5000 GPUs using Pytorch. DeepMCNet’s encoder and decoder included $$$m$$$ channels for $$$m$$$ T1-weighted images of MOLLI5(3)3. we trained DeepMCNet by four iterations according to results of validation. Results of each iteration were used to simulate the reference for the next iteration.
The epi- and endocardial contours of all images were manually delineated. The mean dice coefficient between images was calculated for each slice. After motion correction, the epi- and endocardial contours were deformed by DVF and then mean dice was calculated for evaluating the performance.
Results
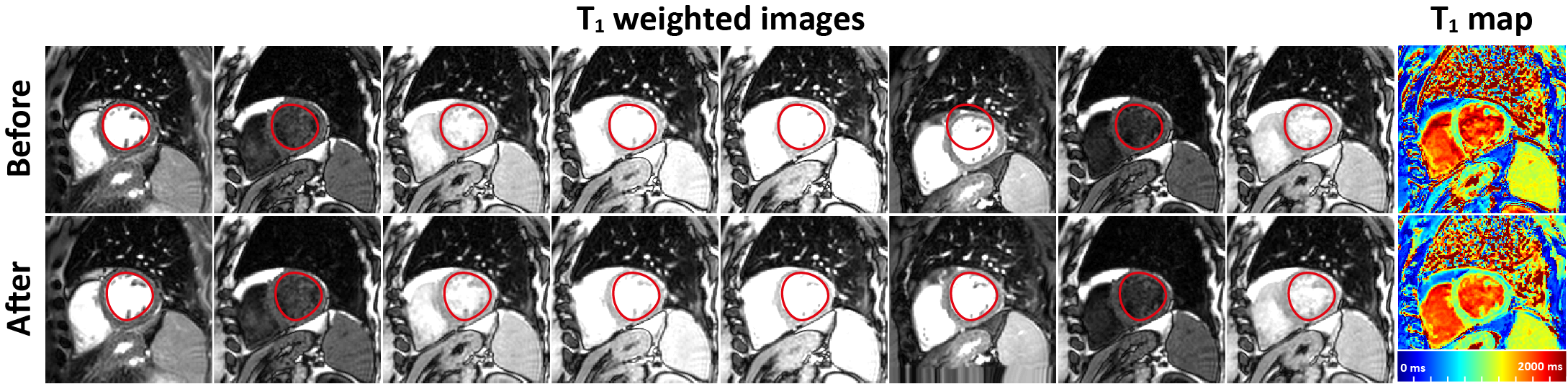
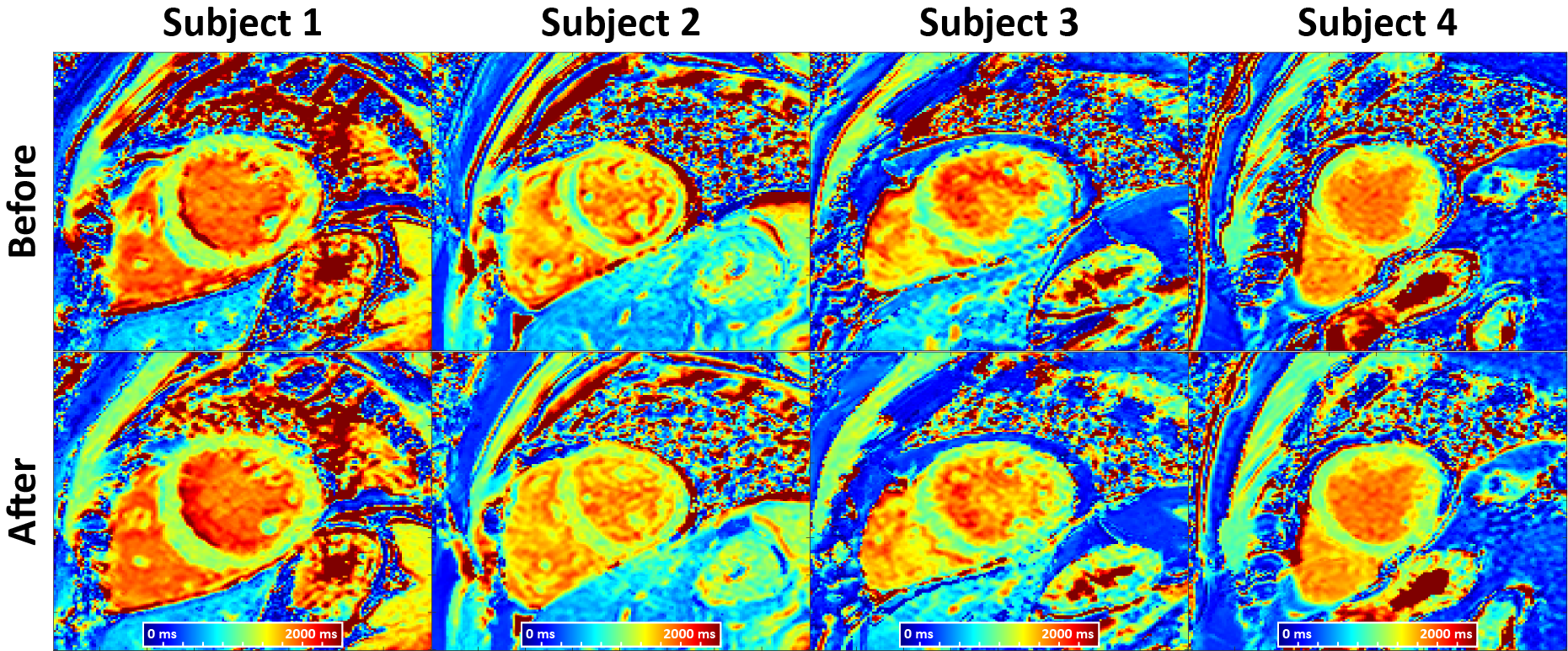
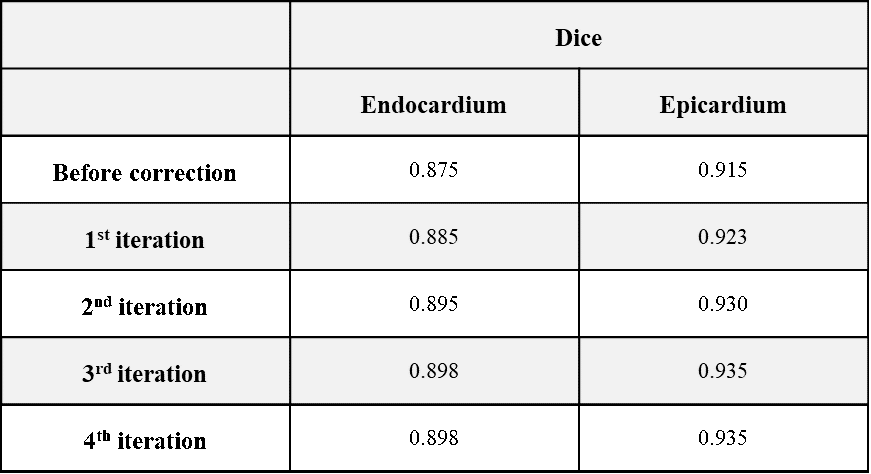
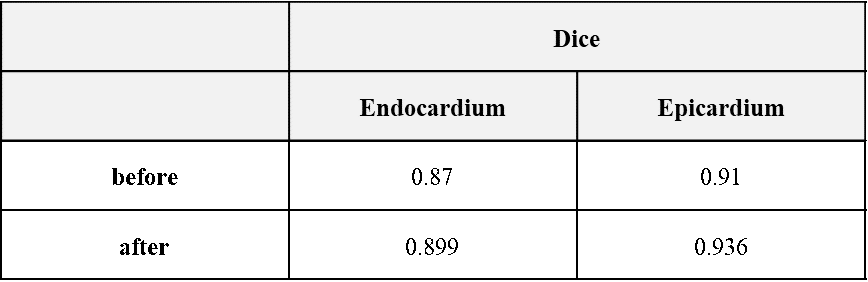
In Table 1, DeepMCNet could improve the dice for both epi- and endocardial contours. Two dice values were improved along with the iterations and reached a steady state after the third iteration. Therefore, we adopted four iterations for the DeepMCNet training. Figure 2 shows the representative results. As can be seen, images after motion correction are matched well and yield high-quality T1 map. In Figure 3, apparent motion artifacts are presented in the maps before motion correction and alleviated by the proposed approach. Dice of epi- and endocardial contours (0.936 and 0.899) in Table 2 were close to corresponding values of validation datasets, meaning the robustness of DeepMCNet and the improvement in alignment of the left-ventricle myocardium across images.Discussion and Conclusion
In this study, synthetized images are used in the self-supervised deep-learning training to address the lack of ground truth in motion correction of CMR images. In addition, a subset of images is used to synthesize the reference for the target input to avoid translating motion information to the reference, improving motion correction performance. Our results indicated left-ventricle myocardium could be aligned by the proposed self-supervised deep-learning approach. Further validation and optimization are warranted.Acknowledgements
This work is supported by the National Natural Science Foundation of China for Young Scholars (No. 82202138), the Fundamental Research Funds for the Young Investigator (No. XSQD-202213003), and the Fundamental Research Funds for the Central Universities (No. LY2022-22).References
1. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, Mascherbauer J, Nezafat R, Salerno M, Schelbert EB, Taylor AJ, Thompson R, Ugander M, van Heeswijk RB, Friedrich MG. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19(75).
2. El-Rewaidy H, Nezafat M, Jang J, Nakamori S, Fahmy AS, Nezafat R. Nonrigid active shape model-based registration framework for motion correction of cardiac T1 mapping. Magn Reson Med 2018;80(2):780-791.
3. Xue H, Shah S, Greiser A, Guetter C, Littmann A, Jolly MP, Arai AE, Zuehlsdorff S, Guehring J, Kellman P. Motion correction for myocardial T1 mapping using image registration with synthetic image estimation. Magn Reson Med 2012;67(6):1644-1655.
4. Roujol S, Foppa M, Weingartner S, Manning WJ, Nezafat R. Adaptive registration of varying contrast-weighted images for improved tissue characterization (ARCTIC): application to T1 mapping. Magn Reson Med 2015;73(4):1469-1482.
5. Weingärtner S, Roujol S, Akçakaya M, Basha TA, Nezafat R. Free‐breathing multislice native myocardial T1 mapping using the slice‐interleaved T1 (STONE) sequence. Magnetic Resonance in Medicine 2014;74(1):115-124.
Figures