1481
The value of Synthetic Magnetic Resonance Imaging in differentiating Muscular Invasion in Bladder Cancer1Radiology, Affiliated Cancer Hospital of Zhengzhou University; Henan Cancer Hospital, Zhengzhou, China, 2GE Healthcare MR Research, Beijing, China
Synopsis
Keywords: fMRI Analysis, Bladder
Motivation: The evaluation of muscular invasion in bladder cancer is essential for determining the optimal surgical approach for patients1. The application of Synthetic magnetic resonance imaging (MAGic resonance imaging, MAGiC) in assessing muscular invasion has not been reported previously2.
Goal(s): To assess the value of MAGiC in diagnosing muscular invasion in bladder cancer.
Approach: This study evaluated the differences of T1/T2/ADC and VI-RADS between non-muscle invasive and muscle invasive lesions and the differentiation performance of the indices.
Results: Improved diagnosis performance was obtained with combined T2 relaxometry and VI-RADS in compared with each single index.
Impact: The findings of this study demonstrate that quantitative MRI parameters enhance the precision and objectivity of assessing muscular invasion in bladder cancer, exhibiting minimal dependence on the clinical experience of diagnostic physician, thus holding promise for their wide-ranging application.
Introduction
The preoperative diagnosis of muscular invasion in bladder cancer plays a crucial role in treatment option selection and prognostic prediction1. The VI-RADS scoring system released in 2018 was considered valuable in determining the invasion of the muscle layer in bladder cancer3. Several studies have evaluated the reproducibility and diagnostic ability of VI-RADS4-6, however, the accuracy of these evaluations relies heavily on the diagnostic experience of the imaging physicians7. The development of quantitative imaging parameters is necessary for facilitating the diagnosis. The aim of this study is to explore the value of synthetic magnetic resonance imaging in diagnosing muscular invasion in bladder cancer, and evaluate whether its quantitative parameters can improve the diagnostic performance of the VI-RADS scoring system.Methods and Materials
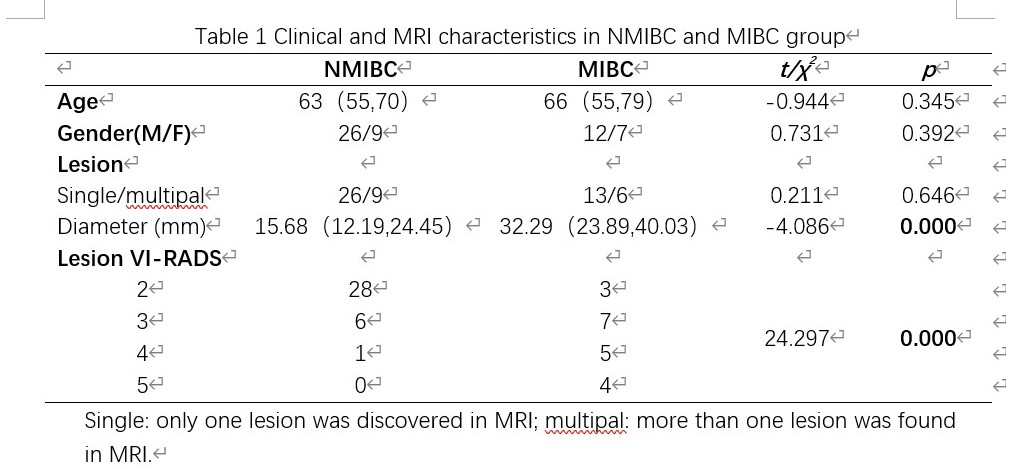
A total of 54 patients with bladder cancer were prospectively enrolled between May 2023 and September 2023. The inclusion criteria are: (1) Patients for consultation due to bladder masses or hematuria, (2) Routine MRI + MAGiC performed; and the exclusion criteria are: (1) Postoperative pathology confirmed a pathological type other than urothelial carcinoma,(2) History of other tumors,(3) Received antitumor treatment or underwent biopsy before the examination,(4) Contraindications for MRI,(5) Unable to undergo surgery after multidisciplinary clinical consultation,(6) Maximum lesion diameter ≤ 5mm,(7) Poor image quality. According to postoperative pathology, they were divided into non-muscle invasive group (NMIBC) and muscle invasive group (MIBC). All patients underwent routine T1 weighted (T1W), T2 weighted (T2W), DWI (b = 800 s/mm2) MRI and MAGic examination on a 3T MR (Signa Architect, GE Healthcare). The acquisition parameters for SyMRI are as follows: TR/TE, 4500/18.6 msec; slice thickness, 5 mm; FOV, 340 mm; acquisition matrix, 256×160; NEX, 1. Data from MAGiC acquisition was processed with software SyMRI (SyntheticMR, Linköping, Sweden, ver. 8.0) to obtain the T1, T2 and PD maps. Region of interest (ROI) in T1, T2, PD and ADC maps was defined in the slice covering the maximum level using the T1W as reference. VI-RADS scores for the lesions were evaluated based on T2WI and DWI images3. The numeric variables were compared using t-test or Wilcoxon test according to the normality and homogeneity of variance, while the categorical variables were analyzed with chi-square test or Fisher exact test. Univariate and multivariate logistic regression were performed to identify independent predictors for muscle invasion and explore the optimal combined indices for muscle invasion diagnosis. DeLong's test was applied to compare the area under curve (AUC) among parameters.Results
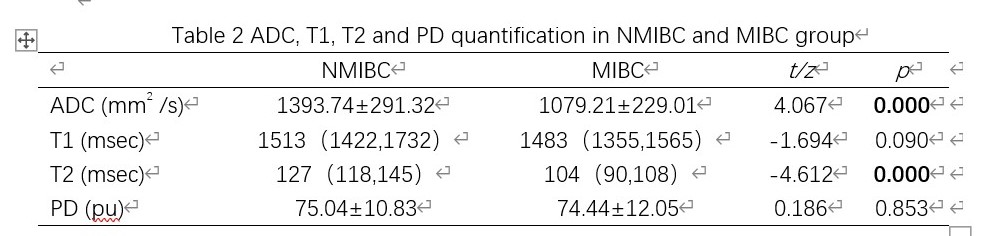
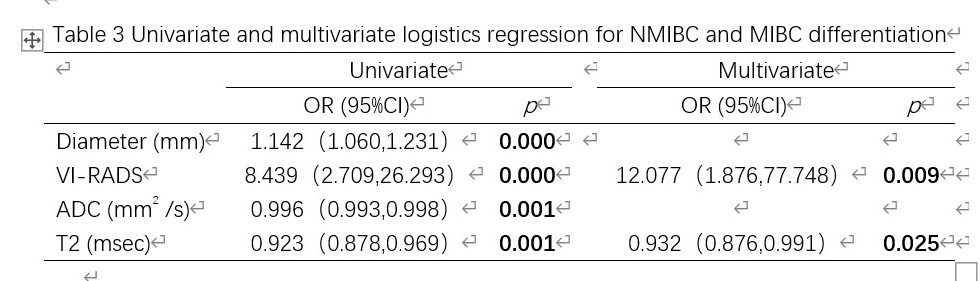
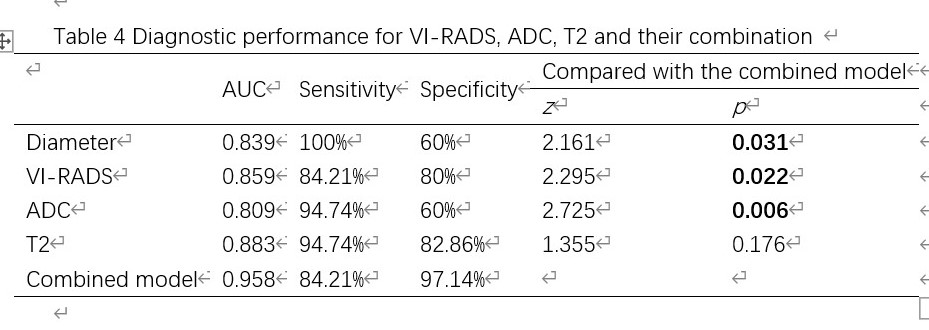
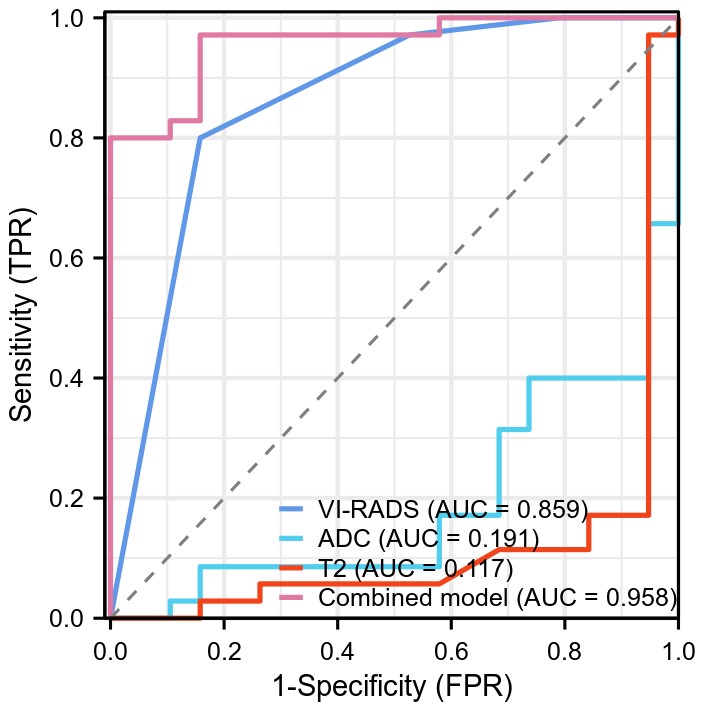
Significant differences were found for Diameter, VI-RADS score, ADC, and T2 relaxometry between NMIBC and MIBC groups (Table1, Table2) (p < 0.05). Univariate and multivariate analysis indicated the VI-RADS score and T2 relaxometry the independent predictors for muscle invasion in bladder cancer (Table 3). The AUC for model combing the VI-RADS and T2 is of 0.958 (sensitivity = 0.8421, specificity = 0.9714), which outperformed the performance with each single index (Table 4, Figure1).Discussion
A statistically significant higher T2 relaxometry was observed for T2 values of the NMIBC group than that of the MIBC group, which is consistent with the study on cervical cancer 8. These similar findings may be attributed to the fact that MIBC grow faster than NMIBC, which results in a higher cellular density, further decreasing the extracellular space and the free water content in tissue. Moreover, MIBC are more likely to be accompanied by cellular necrosis, and macromolecular substances are released into the extracellular space. These factors may account for the lower T2 value in high-grade tumors than in low-grade tumors. ADC was lower in MIBC than in NMIBC group, which is consistent with the previous study2. The cellular density was higher in MIBC group, which results in a decrease of water molecules in the extracellular space, leading to restricted diffusion of water molecules. Compared with a single parameter, the combined model of VI-RADS+T2 mainly improves the specificity, while the specificity of ADC is lower than that of VI-RADS, so it is not helpful to VI-RADS.Conclusion
T2 relaxometry and VI-RADS score were identified the independent factors for muscle invasive lesion differentiation. Higher specificity of T2 relaxometry can improve the performance of VI-RADS score, which contribute to the accurate determinization for optimal surgical strategy.Acknowledgements
No acknowledgement found.References
[1] Compérat E, Amin MB, Cathomas R, et al. Current best practice for bladder cancer: a narrative review of diagnostics and treatments. Lancet. 2022 Nov 12;400(10364):1712-1721. doi: 10.1016/S0140-6736(22)01188-6. Epub 2022 Sep 26. PMID: 36174585.
[2] Cai Q, Wen Z, Huang Y, et al. Investigation of Synthetic Magnetic Resonance Imaging Applied in the Evaluation of the Tumor Grade of Bladder Cancer. J Magn Reson Imaging. 2021 Dec;54(6):1989-1997. doi: 10.1002/jmri.27770. Epub 2021 Jun 3. PMID: 34080268.
[3] Panebianco V, Narumi Y, Altun E, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur Urol. 2018 Sep;74(3):294-306. doi: 10.1016/j.eururo.2018.04.029. Epub 2018 May 10. PMID: 29755006; PMCID: PMC6690492.
[4] Wang H, Luo C, Zhang F, et al. Multiparametric MRI for Bladder Cancer: Validation of VI-RADS for the Detection of Detrusor Muscle Invasion. Radiology. 2019 Jun;291(3):668-674. doi: 10.1148/radiol.2019182506. Epub 2019 Apr 23. PMID: 31012814.
[5] Del Giudice F, Barchetti G, De Berardinis E, et al. Prospective Assessment of Vesical Imaging Reporting and Data System (VI-RADS) and Its Clinical Impact on the Management of High-risk Non-muscle-invasive Bladder Cancer Patients Candidate for Repeated Transurethral Resection. Eur Urol. 2020 Jan;77(1):101-109. doi: 10.1016/j.eururo.2019.09.029. Epub 2019 Nov 5. PMID: 31699526.
[6] Panebianco V, Pecoraro M, Del Giudice F, et al. VI-RADS for Bladder Cancer: Current Applications and Future Developments. J Magn Reson Imaging. 2022 Jan;55(1):23-36. doi: 10.1002/jmri.27361. Epub 2020 Sep 17. PMID: 32939939.
[7] Ueno Y, Tamada T, Takeuchi M, et al. Vesicle Imaging and Data Reporting System (VI-RADS): Multi-institutional multi-reader diagnostic accuracy and inter-observer agreement study. American Journal of Roentgenology. 2020. doi:10.2214/ajr.20.23604.
[8] Wang Y, He M, Cao P, et al. Tissue Characteristics of Endometrial Carcinoma Analyzed by Quantitative Synthetic MRI and Diffusion-Weighted Imaging. Diagnostics (Basel). 2022 Nov 25;12(12):2956. doi: 10.3390/diagnostics12122956. PMID: 36552962; PMCID: PMC9776551.
Figures