1471
A pilot study on the value of T1ρ mapping in preoperatively predicting the status of ER, PR, HER-2 and Ki-67 in breast cancer1West China Hospital, Chengdu, China, 2Philips Healthcare, Chengdu, China
Synopsis
Keywords: Breast, Breast
Motivation: Noninvasive imaging methods capable of revealing molecular characteristic heterogeneity in breast cancer may help to compensate for the sampling errors of biopsy and guide tailored treatment.
Goal(s): To explore the value of T1ρ mapping in preoperatively predicting the status of ER, PR, HER-2 and Ki-67 in breast cancer.
Approach: This is a prospective diagnostic study. The differences of T1ρ values of tumors with different status of ER, PR, HER-2 and Ki-67 were compared between groups.
Results: The T1ρ values showed significant differences in ER (P<0.01), PR(P=0.01), HER-2 (P=0.04), and Ki-67(P=0.02) negative and positive groups, with respective AUCs of 0.867, 0.79, 0.77, and 0.75.
Impact: T1ρ mapping is expected to be a non-invasive tool to help evaluate ER, PR, HER-2, and Ki-67 status before surgery in breast cancer, and to provide assistance in individualized treatment.
Introduction
Breast cancer is a highly heterogeneous, which complicates its treatment planning, clinical outcomes and prognosis. It is classified based on the molecular subtypes using the expression levels of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER-2), and Ki-67. Core needle biopsy (CNB), which is widely applied for preoperative molecular subtyping, can suffer from intratumor heterogeneity due to the small sample size. Preoperative Noninvasive imaging methods capable of revealing histologic and molecular characteristic heterogeneity in breast cancer may be used to compensate for the sampling errors of CNB and guide tailored treatment schedules. T1ρ mapping is a functional MRI sequence that is sensitive to biological processes associated with alterations in the macromolecular content of tissues. The molecular information produced from T1ρ imaging could provides an opportunity to expand the array of biological processes that can be further examined cancers, and it can be added easily to the routine MRI protocol for cancer imaging with no need of contrast injection. Thus we intended to find the potential role of T1ρ mapping in predicting the status of ER, PR, HER-2 and Ki-67 in breast cancer before surgery.Methods
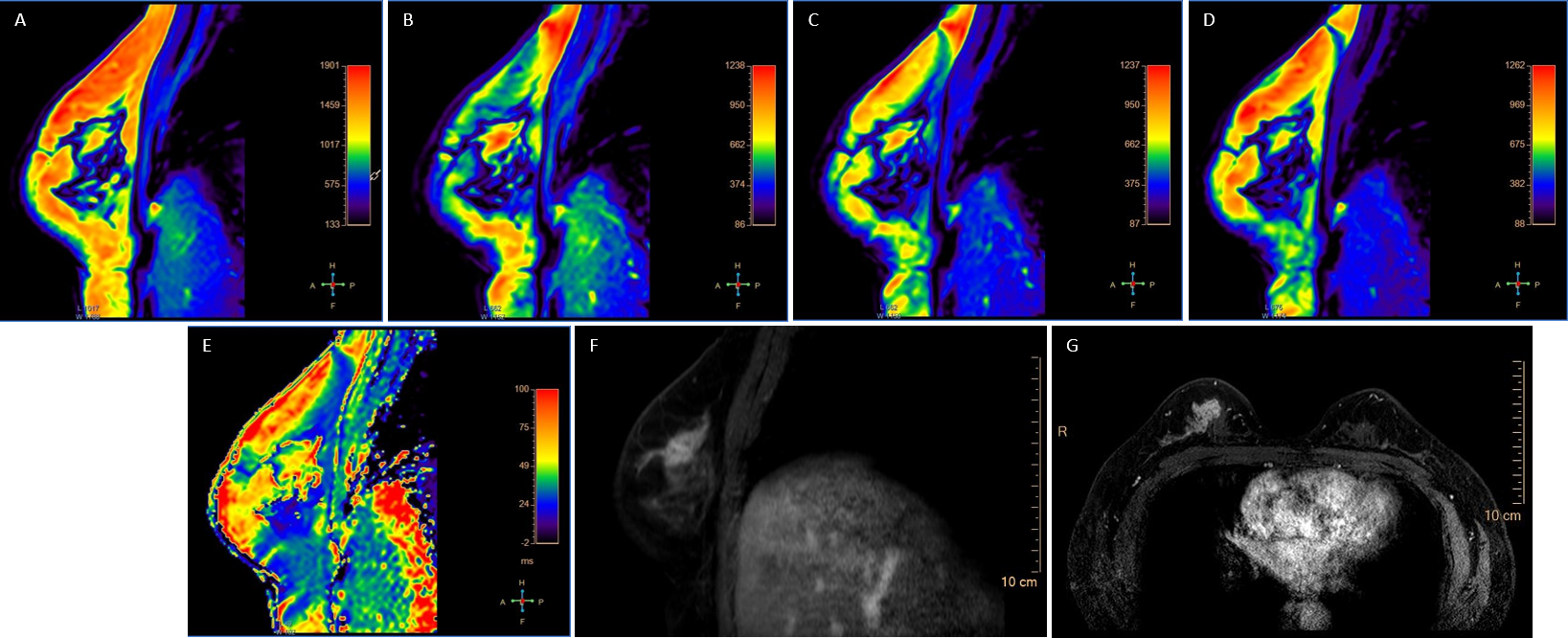
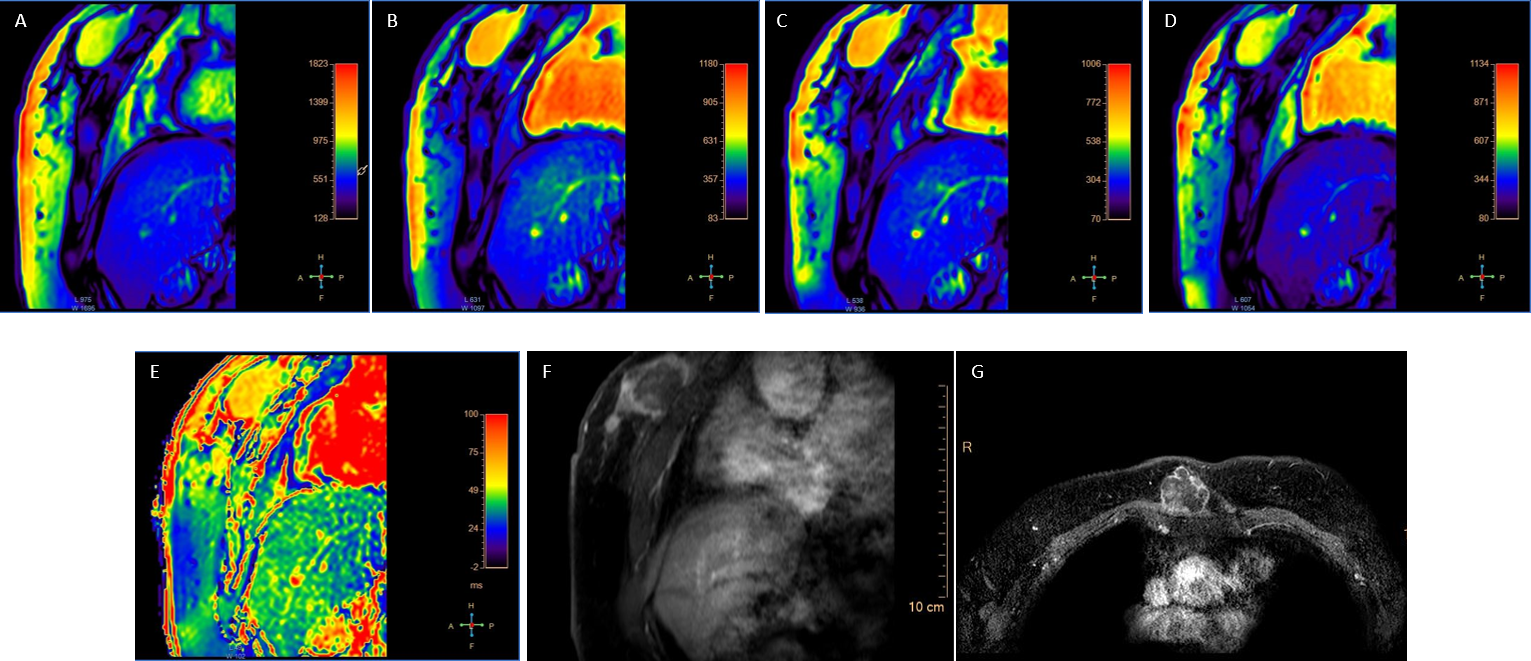
26 biopsy proved breast cancer patients were prospectively enrolled in this study. This study was approved by the Institutional Review Board, and informed consent was obtained from all patients. They all received preoperative clinical routine breast MRI, including T2 weighted imaging (T2WI), T1 weighted imaging (T1WI), diffusion weighted imaging (DWI), contrast dynamic enhancement (DCE), and T1ρ mapping sequences with an eight-channel phased-array breast coil in prone position. Patients were grouped into ER, PR, HER-2 and Ki-67 negative (n=5, 5, 20, 13, respectively) and positive groups (n=21, 21, 6, 13, respectively) with reference to pathological results. Regions of interest (ROIs) were drawn by two radiologists along the edge of the tumor at three largest slices on T1ρ mapping images, and avoiding artifacts, blood vessels, necrosis, etc. The average value of two measurements was calculated as a final absolute T1ρ value of the lesion. Independent t test, receiver operating characteristic (ROC) curves analysis were used for statistical analyses.Results
Patients with ER positive status had significantly lower T1ρ value compared with negative group (57.93±9.13 vs. 72.94±10.79, P<0.01). ROC curve showed that T1p presented areas under ROC curves (AUCs) of 0.867 in predicting ER status, sensitivity of 100% and specificity of 71%, with the cut-off value of 62.5. Patients with PR positive status also had significantly lower T1ρ value compared with negative group (58.27±9.21 vs. 71.54±12.62, P=0.01). ROC curve showed that T1p presented AUCs of 0.79 in predicting PR status, sensitivity of 80% and specificity of 71%, with the cut-off value of 64.44. Patients with HER-2 positive status had significantly higher T1ρ value compared with negative group (69.98±11.81 vs. 58.07±9.43, P=0.04). ROC curve showed that T1p presented AUCs of 0.77 in predicting PR status, sensitivity of 83% and specificity of 70%, with the cut-off value of 62.6. Patients with Ki-67 positive status showed significantly higher T1ρ value compared with negative group (65.6±9.41 vs. 56.05±10.76, P=0.02). ROC curve showed that T1p presented AUCs of 0.75 in predicting Ki-67 status, sensitivity of 77% and specificity of 69%, with the cut-off value of 59.19.Discussion
T1ρ values can distinguish between positive and negative states of ER, PR, HER-2, and Ki-67. T1ρ mapping has the potential for preoperative evaluation of ER, PR, HER-2, and Ki-67 status. MR T1ρ mapping imaging can be used to study low-frequency motion in biological systems, such as proton exchange between water and large molecules, thus suggesting an indirect exploration of the content of large molecules such as proteoglycans and proteins in soft tissue. It probes the slow motion interactions between motion-restricted water molecules and their local macromolecular environment. The extracellular matrix in tumor provides a motion-restricted environment to water molecules. The extracellular matrix is composed of proteins, proteoglycans, and collagen, and is an important barrier to prevent tumor invasion and metastasis. Breast cancer cells can secrete a variety of proteolytic enzymes to degrade extracellular matrix components and promote cancer cell metastasis. Changes to the extracellular matrix, such as proteoglycan loss related with different ER, PR, HER-2, and Ki-67 status may be reflected in measurements of T1ρ value.Conclusion
T1ρ mapping is expected to be a non-invasive tool to help evaluate ER, PR, HER-2 and Ki-67 status in breast cancer patients before surgery, and to provide assistance for doctors in individualized treatment in clinical.Acknowledgements
None.References
1. Kazama T, Takahara T, Hashimoto J. Breast Cancer Subtypes and Quantitative Magnetic Resonance Imaging: A Systemic Review. Life (Basel). 2022 Mar 28;12(4):490. doi: 10.3390/life12040490. PMID: 35454981; PMCID: PMC9028183.
2. Amano M, Fujita S, Takei N, Sano K, Wada A, Sato K, Kikuta J, Kuwatsuru Y, Tachibana R, Sekine T, Horimoto Y, Aoki S. Feasibility of Quantitative MRI Using 3D-QALAS for Discriminating Immunohistochemical Status in Invasive Ductal Carcinoma of the Breast. J Magn Reson Imaging. 2023 Mar 23. doi: 10.1002/jmri.28683. Epub ahead of print. PMID: 36951614.
3. Liu Z, Wen J, Wang M, Ren Y, Yang Q, Qian L, Luo H, Feng S, He C, Liu X, Wu Y, Luo D. Breast Amide Proton Transfer Imaging at 3 T: Diagnostic Performance and Association With Pathologic Characteristics. J Magn Reson Imaging. 2023 Mar;57(3):824-833. doi: 10.1002/jmri.28335. Epub 2022 Jul 11. PMID: 35816177.
4. Rahbar H, Zhang Z, Chenevert TL, Romanoff J, Kitsch AE, Hanna LG, Harvey SM, Moy L, DeMartini WB, Dogan B, Yang WT, Wang LC, Joe BN, Oh KY, Neal CH, McDonald ES, Schnall MD, Lehman CD, Comstock CE, Partridge SC. Utility of Diffusion-weighted Imaging to Decrease Unnecessary Biopsies Prompted by Breast MRI: A Trial of the ECOG-ACRIN Cancer Research Group (A6702). Clin Cancer Res. 2019 Mar 15;25(6):1756-1765. doi: 10.1158/1078-0432.CCR-18-2967. Epub 2019 Jan 15. PMID: 30647080; PMCID: PMC6420847.
5. Someya Y, Iima M, Imai H, Yoshizawa A, Kataoka M, Isoda H, Le Bihan D, Nakamoto Y. Investigation of breast cancer microstructure and microvasculature from time-dependent DWI and CEST in correlation with histological biomarkers. Sci Rep. 2022 Apr 20;12(1):6523. doi: 10.1038/s41598-022-10081-7. PMID: 35444193; PMCID: PMC9021220.
Figures