1468
Amide proton transfer weighted imaging and diffusion kurtosis imaging in differentiating breast lesions by comparing with BI-RADS1Department of Radiology, Affiliated Hospital of Jiangnan University, Wuxi Medical School of Jiangnan University, Wuxi, Jiangsu, 214122, People’s Republic of China, Wuxi, China, 2GE Healthcare, MR Research China GE Healthcare, MR Research China, Beijing, P.R. China, Beijing, China
Synopsis
Keywords: fMRI Acquisition, Breast, Amide proton transfer weighted imaging, Diffusion kurtosis imaging
Motivation: Breast Imaging Reporting and Data System (BI-RADS) is an internationally recognized scoring standard for the diagnosis of breast lesions, but it is highly subjective.
Goal(s): To evaluate the diagnostic performance of amide proton transfer weighted imaging (APTWI) and diffusion kurtosis imaging (DKI) in terms of differentiating breast lesions and to compare them with the BI-RADS independently or jointly.
Approach: Prospective cohort study
Results: APTWI and DKI can be used to distinguish breast lesions. The combination with APTWI and DKI can significantly improve the AUC values and specificity when compared with BI-RADS alone. The APTWI+DKI+BI-RADS has the best diagnostic performance in distinguishing breast lesions.
Impact: The combined APTWI and DKI outperformed BI-RADS alone in distinguishing benign and malignant breast lesions.
INTRODUCTION
Diffusion kurtosis imaging (DKI) is a diffusion imaging technique based on non-Gaussian diffusion model to reflect the real state of water molecules.Meanwhile, amide proton transfer weighted imaging (APTWI), as a noninvasive molecular-level MRI technique, can generate unique image contrast by measuring the mobile protons in amide compounds and bulk water protons [3]. APTWI and DKI have shown advantages in the diagnosis of tumor lesions and prognosis assessment in recent years[4-9]. However, whether quantitative parameters of APTWI and DKI could improve diagnostic performance of qualitative evaluation (BI-RADS) in the breast remains unclear. We hypothesized that BI-RADS combined with DKI and APTWI would be valuable in diagnosing breast cancer. Thus, this study aimed to investigate the clinical potential of APTWI and DKI in differentiating malignant from benign breast lesions by comparing with BI-RADS, and to further explore the added value of APTWI and DKI to BIRADS.METHODS
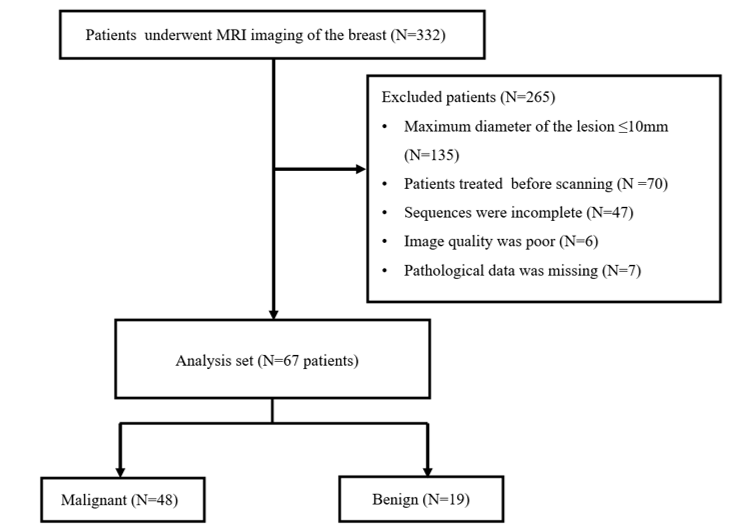
SubjectsThis prospective study was approved by the local institutional review board (LS2022083), with each patient providing informed consent. The study ultimately included 67 participants with 67 breast lesions, including 48 malignant and 19 benign lesions confirmed by pathological test.
MRI experiments
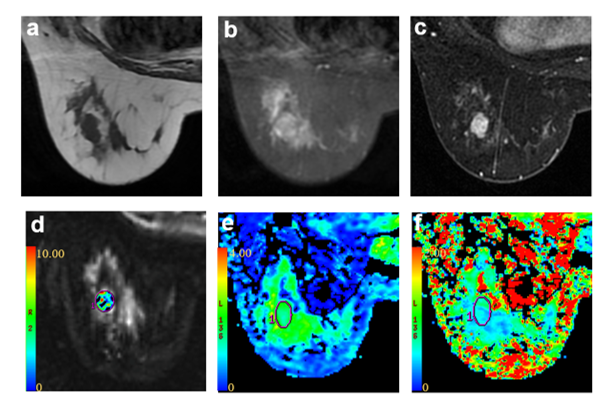
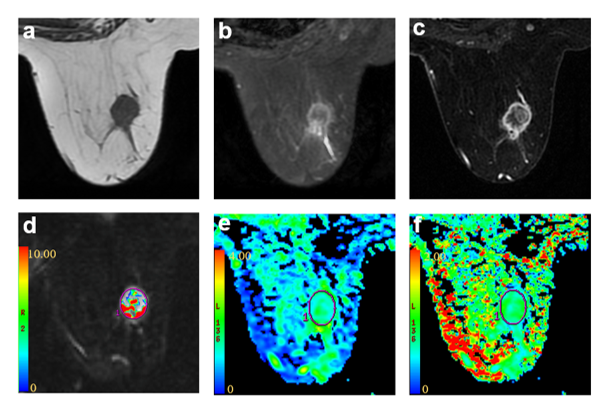
A3.0T MR scanner (Architect, GE Healthcare), equipped with a dedicated 8-channel bilateral breast coil, was used. Under the guidance of an experienced radiologist, and in reference to T1WI and T2WI anatomic imaging, DKI and APTWI were applied for breast cancer patients with covering tumor tissue region[10, 11].
For DKI, a single-shot echo planar imaging sequence with 5 b-values (0,500,1000,1500, 2000 s/mm2) with 15 diffusion directions per b value was applied. Other scan parameters were TR/TE,5000/86.4ms; field-of-view, 32cm×32cm; matrix, 96×128; slice thickness, 5mm; scan time, 2 min 50 s.
For APTWI, a single slice spin echo echo-planar imaging sequence with 52 frequencies images, including three times reference images and 49 frequencies ranging from -600 to 600Hz with an increment of 25Hz, was applied in axial view. The applied saturation power was 2µT and the saturation duration was 2000ms. Other scan parameters were: TR/TE,3000/mini ms; field-of-view, 20cm×20cm; matrix, 128×128; slice thickness, 4mm; scan time, 5min 12 s.
Image processing and analysis
APTWI and DKI data were separately analyzed using the post-processing software developed in the GE ADW4.6 workstation. The APTWI derived MTRasym at 3.5ppm and DKI parameters of mean kurtosis (MK) and mean diffusivity (MD) values were measured independently by two radiologists (with 4 and 5 experiences). The mean values of each parameter measured by the two radiologists were used for final analysis. BI-RADS was scored by another two radiologists (with 5 and 13 experiences).
Statistical
analysisSPSS 26.0 and MedCalc 20.0 statistic software were used for statistic analyses. Intra-class correlation coefficients analysis (ICC) was applied to assess the inter-observer agreement of parameter measurements over two radiologists. The differences in the continuous parameter values between the benign and malignant breast lesions were assessed by using the independent sample t test or Mann ‒Whitney U test. Receiver Operating Characteristic (ROC) curve analysis was separately employed to assess the diagnostic efficacies of APT, DKI, BI-RADS and the combined model in distinguishing benign from malignant breast cancer. The significance threshold was set as P<0.05.
RESULTS
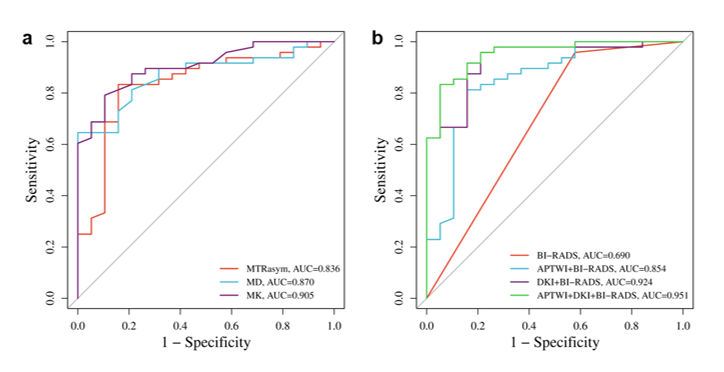
For 67 participants with 67 breast lesions, including 48 malignant and 19 benign lesions, no significant difference was found in age or lesion diameter between the two groups (P > 0.05). The ICCs for MTRasym, MD and MK were 0.985, 0.971, and 0.949. MTRasym and MK were significantly higher in malignant breast lesions than benign lesions, whereas MD was significantly lower in malignant breast lesions than benign lesions. The AUCs of MTRasym, MD, and MK values for the differential diagnosis of benign and malignant breast lesions were 0.836, 0.870, and 0.905, respectively. The AUC of BI-RADS alone was 0.690. The combination of APTWI+BI-RADS, and DKI+BI-RADS can significantly improve the AUC values when compared with BI-RADS alone (0.690 vs. 0.854;0.690 vs. 0.924). Furthermore, the combination of APTWI+DKI+BI-RADS revealed the optimal efficacy in distinguishing benign and malignant breast lesions with largest AUC (0.951) and specificity (94.74%), although BI-RADS still presents the highest sensitivity.DISCUSSION
Our study showed that MTRasym and MK were significantly higher in malignant lesions than benign lesions, and an opposite pattern was found in MD. The malignant lesions are characterized by rapid cell proliferation and increased protein expression, and therefore may have high concentrations of mobile proteins and peptides as well as high cell polarity and more complex tissue structure.CONCLUSION
APTWI and DKI have been demonstrated as effective quantitative techniques for distinguishing the characteristics of breast lesions and may augment the diagnostic performance of BI-RADS.Acknowledgements
Thanks to Dr. Weiqiang Dou and Guangnan Kwon of GE for their help in adjusting the parameters of the magnetic resonance sequence and proofreading the article.References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A: Cancer statistics, 2022. CA Cancer J Clin 2022, 72(1):7-33.
2. Radiology ACo: Breast Imaging Reporting and Data System (BI-RADS) 5th ed. Reston, VA: American College of Radiology; 2013.
3. Zhou J, Payen JF, Wilson DA, Traystman RJ, van Zijl PC: Using the amide proton signals of intracellular proteins and peptides to detect pH effects in MRI. Nat Med 2003, 9(8):1085-1090.
4. Hempel JM, Schittenhelm J, Bisdas S, Brendle C, Bender B, Bier G, Skardelly M, Tabatabai G, Castaneda Vega S, Ernemann U et al: In vivo assessment of tumor heterogeneity in WHO 2016 glioma grades using diffusion kurtosis imaging: Diagnostic performance and improvement of feasibility in routine clinical practice. J Neuroradiol 2018, 45(1):32-40.
5. Meng N, Wang X, Sun J, Han D, Ma X, Wang K, Wang M: Application of the amide proton transfer-weighted imaging and diffusion kurtosis imaging in the study of cervical cancer. Eur Radiol 2020, 30(10):5758-5767.
6. Suo S, Chen X, Wu L, Zhang X, Yao Q, Fan Y, Wang H, Xu J: Non-Gaussian water diffusion kurtosis imaging of prostate cancer. Magn Reson Imaging 2014, 32(5):421-427.
7. Togao O, Yoshiura T, Keupp J, Hiwatashi A, Yamashita K, Kikuchi K, Suzuki Y, Suzuki SO, Iwaki T, Hata N et al: Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades. Neuro Oncol 2014, 16(3):441-448.
8. Wang HJ, Cai Q, Huang YP, Li MQ, Wen ZH, Lin YY, Ouyang LY, Qian L, Guo Y: Amide Proton Transfer-weighted MRI in Predicting Histologic Grade of Bladder Cancer. Radiology 2022, 305(1):E59. 9. Yang L, Wang L, Tan Y, Dan H, Xian P, Zhang Y, Tan Y, Lin M, Zhang J: Amide Proton Transfer-weighted MRI combined with serum prostate-specific antigen levels for differentiating malignant prostate lesions from benign prostate lesions: a retrospective cohort study. Cancer Imaging 2023, 23(1):3.
10. Rosenkrantz AB, Padhani AR, Chenevert TL, Koh DM, De Keyzer F, Taouli B, Le Bihan D: Body diffusion kurtosis imaging: Basic principles, applications, and considerations for clinical practice. J Magn Reson Imaging 2015, 42(5):1190-1202.
11. Tee YK, Donahue MJ, Harston GW, Payne SJ, Chappell MA: Quantification of amide proton transfer effect pre- and post-gadolinium contrast agent administration. J Magn Reson Imaging 2014, 40(4):832-838.
Figures