1462
Weakly Supervised Learning for Prostate Cancer Detection from Co-registered bi-parametric MRI and Patient’s Clinal Data1Joint Department of Medical Imaging, University Health Network, Sinai Health System and University of Toronto, Toronto, ON, Canada, 2Lunenfeld-Tanenbaum Research Institute, Sinai Health System, University of Toronto, Toronto, ON, Canada, 3KITE Research Institute, University Health Network and University of Toronto, Toronto, ON, Canada, 4Institute of Biomedical Engineering, University of Toronto, Toronto, ON, Canada
Synopsis
Keywords: Cancer, Prostate, Image Registration
Motivation: Bi-parametric MRI (bpMRI) is now part of the diagnostic workup for prostate cancer (PCa). Radiologists cognitively coregister bpMRI sequences when interpreting MRI. Conversely, machine learning (ML) algorithms have difficulty learning this implicit coregistration because of the distortion often present in diffusion-weighted images.
Goal(s): Introduce a novel method for automated 1) bpMRI coregistration; and 2) detection of csPCa.
Approach: A weakly supervised learning paradigm was employed for bpMRI co-registration. A combination of co-registered bpMRI and the patient’s clinical data was used for automated csPCa detection.
Results: The proposed method achieved a true and false positive rate of 86% and 41% on 100 test cases.
Impact: The obtained results demonstrated the value of co-registration and including patient clinical data for designing ML-based methods for automated csPCa detection. The proposed algorithm might improve the accuracy of reading bpMRI, thereby beneficial for patients with prostate cancer.
Itroduction
Prostate cancer is the second most common cancer in men worldwide 1. Bi-parametric MRI—consisting of T2-weighted (T2W) images, DWI, and calculated apparent diffusion coefficient (ADC) maps—is a useful tool for the diagnosis of PCa lesions. Machine learning (ML) could reduce the interobserver variability and dependence of accuracy on reader experience currently present in PCa detection from bpMRI 2.Many studies have previously published ML-based methods for automated contouring of PCa on MRI 3-5. Our previous study demonstrated the value of co-registration by showing that a PCa detection model trained on co-registered bpMRI significantly outperformed similar models trained on either unregistered bpMRI or single-sequence MRI (p<0.001; both scenarios) 6.
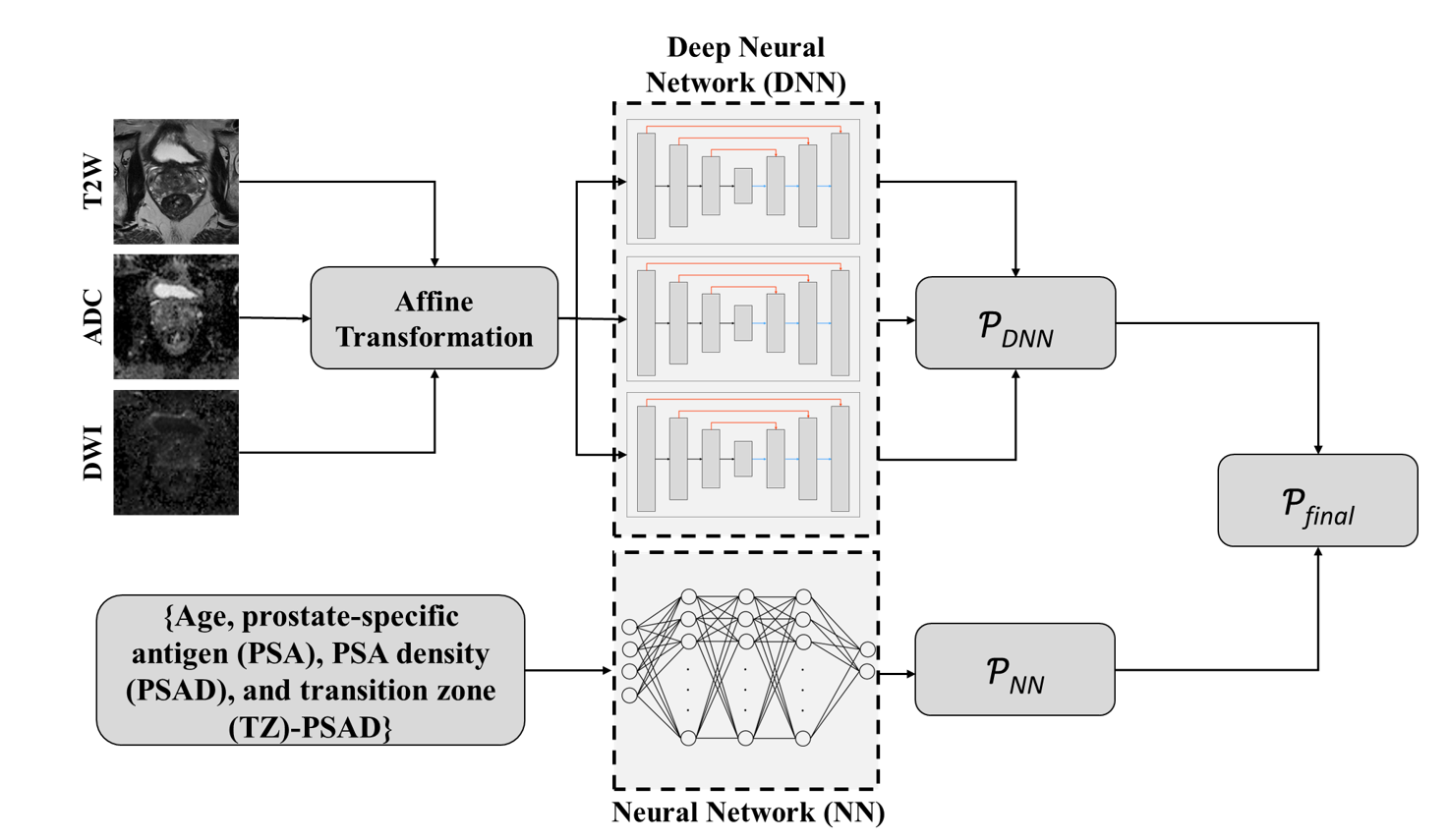
A bottleneck for co-registration algorithms is accurate segmentation of the prostate on bpMRI. Accurate prostate segmentation facilitates the alignment between prostate anatomy on different MR sequences. However, training a prostate segmentation algorithm requires carefully annotated data. For this study, data from Prostate Imaging, Cancer AI Grand Challenge (PI-CAI) was used, where annotation of the prostate anatomy only exists for T2W images (i.e., not for ADC nor DWI). Since the MR sequences are not co-registered, this T2W segmentation does not match the boundary of the prostate on other MR sequences. To reduce the cost of human-expert annotation, we employed weakly supervised learning to train a deep neural network (DNN) for producing a segmentation map of the prostate whole gland on ADC and DWI. The segmentation maps were used to compute a transformation function. An ensemble of three DNNs was then trained to contour csPCa from co-registered bpMRI. However, employing an ensemble of DNNs leads to error aggregation, increasing false positives (FPs). For this reason, in addition to performing co-registration, we trained another neural network (NN) using patient clinical data including patient age, prostate-specific antigen (PSA), PSA density (PSAD), and transition zone (TZ)-PSAD to distinguish and remove FPs (Figure 1).
Method
We used the PI-CAI dataset, consisting of 1295 bpMRI, of which 220 contained csPCa and 1075 did not. Data was split into 1195 and 100 cases for training and testing (respectively), preserving a 1:5 ratio for cases with: without csPCa in both sets.To address the issue of inaccurate supervision resulting from unregistered data, 58 cases (out of 1195 training samples) with severe misalignment between MR sequences were removed from training samples, which is a common approach in inaccurate supervision 7. Two separate 3D U-Nets were trained to delineate the prostate whole gland on the T2W and ADC images. After applying the translation function, computed from prostate segmentation maps, a three-channel image was created from co-registered bpMRI, to be used as an input of the csPCa tumor detection ensemble model.
Another NN was trained using the patient’s clinical data. For cases with csPCa tumors, the probability of the NN was used as a reference to identify FPs. The following equation was used for the final prediction where Ii ∈ {bpMRI1, bpMRI2, …}, xi∈ {(x1, x2, x3, x4)1, (x1, x2, x3, x4)2, …}, yi ∈ {csPCa, non-csPCa}, ƤDNN and ƤNN are the predictions of the ensemble and NN, and µ1 and µ2 were set to 0.7 and 0.3, experimentally.
Ƥfinal = µ1 * ƤDNN (Ii|yi) + µ2 * ƤNN (xi|yi)
Results
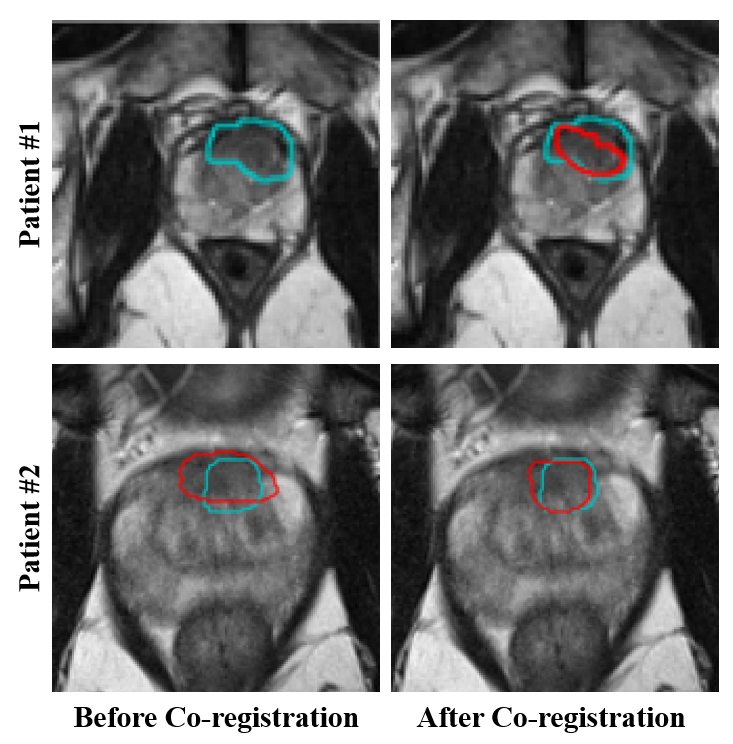
Our test set comprises 80 normal cases and 20 patients with csPCa, with a total of 21 csPCa lesions. The proposed method achieved a true positive rate (TPR) of 86% and 85% per lesion and per patient, with a false positive rate (FPR) of 41%. The area under the receiver operating characteristic curves and average precision at one FP per patient were 0.844 and 0.643, respectively. Figure 2 shows exemplary results for two patients with a csPCa lesion. The results of the ablation study demonstrated that 1) using co-registered bpMRI improved TPR by 10% compared to non-registered MR sequences (86% vs. 76%; p-value = 0.07), while FPR increased by 2%, and 2) embedding NN significantly reduced FPR (41% vs. 71%; P < 0.0001) at the cost of reducing TPR by 4%.Conclusion and Discussion
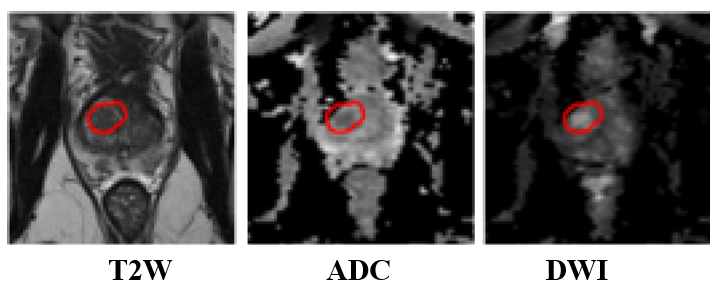
We introduced a novel method for automatically detecting csPCa from a combination of co-registered bpMRI and clinical data. Although using co-registered bpMRI improves the performance of the method for csPCa detection it increases the number of FPs. A possible explanation for this increase is that training a network with co-registered data can encourage the model to capture suspicious regions on T2W that have corresponding dark and bright areas on the ADC and DWI, respectively, as shown in Figure 3. Including dynamic contrast-enhanced MRI might address this issue.Acknowledgements
The Ontario Institute of Cancer Research, Sinai Hospital Foundations, and University Medical Imaging Toronto, Ontario, Canada supported this work.
References
[1] World Cancer Research Fund International. Prostate Cancer Statistics. https://www.wcrf.org/cancer-trends/prostate-cancer-statistics. March 23, 2022. Accessed October 5, 2023.
[2] Woo S, Suh CH, Kim SY, et al. Diagnostic Performance of Prostate Imaging Reporting and Data System Version 2 for Detection of Prostate Cancer: A Systematic Review and Diagnostic Meta-analysis. Eur Urol. 2017;72:177-188.
[3] Yoo S, Gujrathi I, Haider MA, et al. Prostate Cancer Detection using Deep Convolutional Neural Networks. Sci Rep. 2019; 9:19518.
[4] Zabihollahy F, Ukwatta E, Krishna S, et al. Fully automated localization of prostate peripheral zone tumors on apparent diffusion coefficient map MR images using an ensemble learning method. J Magn Reson Imaging. 2020;51:1223-1234.
[5] Giannini V, Mazzetti S, Vignati A, et al. A fully automatic computer-aided diagnosis system for peripheral zone prostate cancer detection using multi-parametric magnetic resonance imaging. Comput Med Imaging Graph. 2015;46(Pt 2):219-26.
[6] Zabihollahy F, Heming CAM, Gujrathiet I, et al., Anatomically Constrained Multiparametric MRI Co-Registration for False Positive Aware Prostate Cancer Tumor Detection. Journal of Medical Image Analysis, Under Review.
[7] Zhou ZH, A brief introduction to weakly supervised learning. National Science Review. 2018;5(1):44–53.
Figures