1461
Associations Between Prostate Cancer Lesion Location on mpMRI and Upgrading from Biopsy-Confirmed Histopathology to Final Pathology1Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
Keywords: Cancer, Prostate, mpMRI, Gleason Score, Upgrading
Motivation: Given discrepancies in biopsy-confirmed histopathology and final pathology in prostate cancer, there is a clinical need to improve diagnosis and treatment planning using multiparametric MRI (mpMRI).
Goal(s): To assess associations between mpMRI lesion location and upgrading of prostate cancer from biopsy-confirmed histopathology to final pathology.
Approach: 191 patients who underwent both MRI-ultrasound fusion biopsy and prostatectomy were included. A modified χ² test assessed associations between mpMRI lesion location and upgrading from biopsy-confirmed histopathology to final pathology.
Results: mpMRI lesions in the peripheral zone and posterior region were more likely to be upgraded than lesions in the transition zone and anterior region respectively.
Impact: In patients who undergo MRI-ultrasound fusion biopsy and prostatectomy, mpMRI lesions in the peripheral zone and posterior region were more likely to be upgraded from biopsy-confirmed histopathology to final pathology than lesions in the transition zone and anterior region respectively.
Background
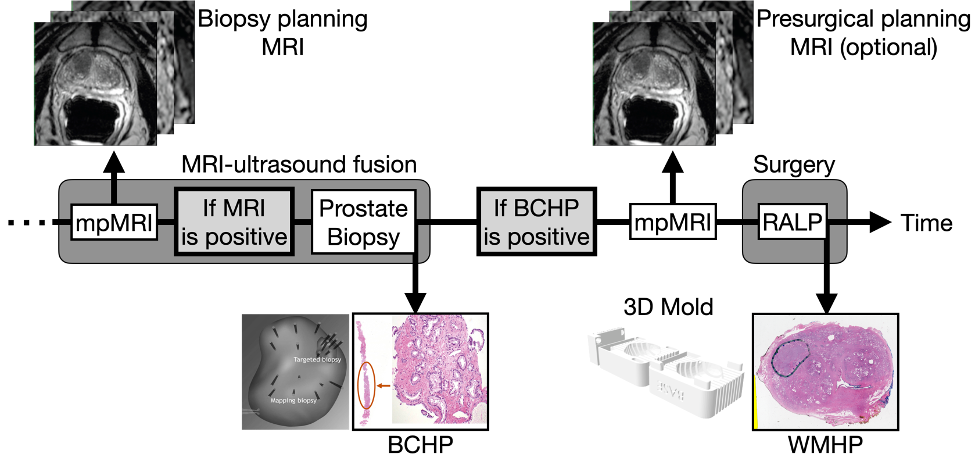
Prostate multiparametric magnetic resonance imaging (mpMRI) is a non-invasive tool for detecting high-grade and larger tumors (1). When mpMRI findings are positive and/or clinical suspicion of prostate cancer is high, an MRI-targeted prostate biopsy will be performed, and if biopsy-confirmed histopathology (BCHP) is positive, the patient can undergo robot-assisted laparoscopic prostatectomy (RALP) or other treatments. When subjects undergo RALP, two histopathological findings are available (Figure 1), including BCHP and whole-mount histopathology (WMHP). Prior studies have shown that more than 30% of cases of indolent prostate cancer at biopsy are upgraded to clinically significant prostate cancer, while more than 25% of clinically significant prostate cancer at biopsy are downgraded to indolent prostate cancer, compared to WMHP after RALP (2). Therefore, there is a clinical need to understand the spatial characteristics of prostate cancer lesions on mpMRI when discrepancies exist between BCHP and WMHP to improve diagnosis and treatment planning.Methods
In this retrospective study, we reviewed 942 consecutive patients who underwent mpMRI prior to RALP from 2010 to 2023. Clinicodemographic, MRI, and histopathologic data were extracted from our prospectively maintained integrated diagnostics (IDx) database with IRB and HIPAA approval. We also combined MRI-ultrasound fusion biopsy and RALP to identify patients who underwent both MRI-ultrasound fusion biopsies and RALP and had available radiologic and pathologic data. A total of 415 true positive mpMRI lesions from 191 patients were isolated, and the maximum Gleason Scores from targeted biopsy and prostatectomy were collected. All the lesions were mapped into a sector map, described in Prostate Imaging Reporting and Data System (PI-RADS) v2.1, for the standardized prostate segmentation model (3).Lesions were identified as being upgraded, downgraded, or isograded based on changes in their Gleason Grade from BCHP to WMHP. The number of lesions in each sector of the prostate that was upgraded, downgraded, or isograded was recorded, and adjusted weights were calculated based on the relative prevalence of lesions in each sector. The sum of adjusted weights was calculated for each region of the prostate (transition vs. peripheral zone, anterior vs. posterior, base vs. midgland vs. apex, and left vs. right). A modified χ² test was used to assess associations between mpMRI lesion location, race (Black vs. Non-Hispanic White), and upgrading of prostate cancer from BCHP to WMHP.
Results
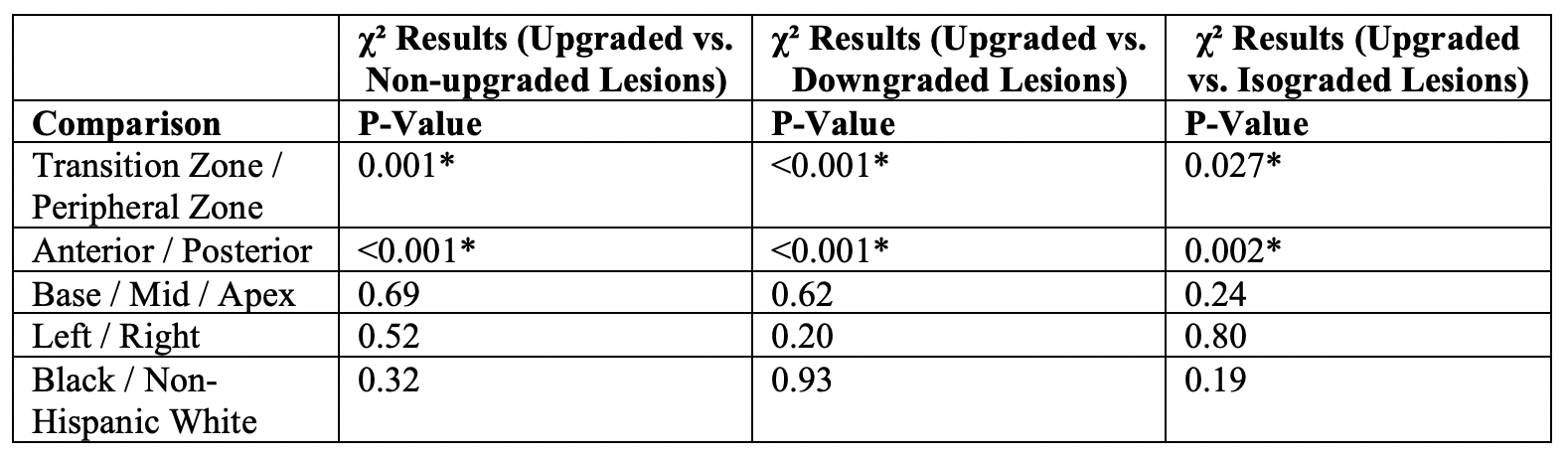
Compared with mpMRI lesions in the transition zone, lesions in the peripheral zone were more likely to be upgraded vs. non-upgraded (P = 0.001), downgraded (P < 0.001), or isograded (P = 0.027). Compared with mpMRI lesions in the anterior region, lesions in the posterior region were more likely to be upgraded vs. non-upgraded (P < 0.001), downgraded (P < 0.001), or isograded (P = 0.002). In the base vs. midgland vs. apex of the prostate, there was not a statistically significant difference between actual and expected sums of adjusted weights for lesions that were upgraded vs. non-upgraded (P = 0.69), downgraded (P = 0.62), or isograded (P = 0.24). In the left vs. right side of the prostate, there was not a statistically significant difference between actual and expected sums of adjusted weights for lesions that were upgraded vs. non-upgraded (P = 0.52), downgraded (P = 0.20), or isograded (P = 0.80). For Black vs. Non-Hispanic White patients, there was not a statistically significant difference between rates of upgrading vs. non-upgrading (P = 0.32), downgrading (P = 0.93), or isograding (P = 0.19). Table 1 summarizes the results of our analysis.Conclusions
mpMRI lesions in the peripheral zone and posterior region had a higher likelihood of being upgraded than lesions in the transition zone and anterior region, respectively. Multicenter, prospective trials are necessary to further characterize the role of mpMRI in predicting discrepancies between BCHP and WMHP, and future trials should incorporate additional quantitative and qualitative parameters extracted from mpMRI.Acknowledgements
This work was supported by the National Institutes of Health (NIH) R01-CA248506 and R01-CA272702, and funds from the Integrated Diagnostics Program, Departments of Radiological Sciences & Pathology, David Geffen School of Medicine at UCLA.References
1. Turkbey B, Brown AM, Sankineni S, Wood BJ, Pinto PA, Choyke PL. Multiparametric prostate magnetic resonance imaging in the evaluation of prostate cancer. CA Cancer J Clin. Jul 2016;66(4):326-36. doi:10.3322/caac.21333
2. Epstein JI, Feng Z, Trock BJ, Pierorazio PM. Upgrading and downgrading of prostate cancer from biopsy to radical prostatectomy: incidence and predictive factors using the modified Gleason grading system and factoring in tertiary grades. Eur Urol. May 2012;61(5):1019-24. doi:10.1016/j.eururo.2012.01.050
3. Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. Sep 2019;76(3):340-351. doi:10.1016/j.eururo.2019.02.033
Figures