1459
Radiomics and Background Parenchymal Enhancement of Fibroglandular Tissue for Predicting Treatment Response in Triple-Negative Breast Cancer1Cancer Systems Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 2Imaging Physics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 3Breast Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 4Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 5Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 6Radiology - Breast Imaging, UT Southwestern Medical Center, Dallas, TX, United States, 7Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 8Abdominal and Breast Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States
Synopsis
Keywords: Breast, Cancer, Treatment response, DCE-MRI, neoadjuvant therapy
Motivation: No imaging biomarkers are currently available for predicting response to neoadjuvant systemic treatment (NAST) in triple negative breast cancer (TNBC), contributing to toxicity to patients from ineffective treatment regimens.
Goal(s): To evaluate if quantitative analyses of breast parenchyma can serve as noninvasive biomarker of treatment response in TNBC.
Approach: Mean background parenchymal enhancement (BPE) and radiomic features of fibroglandular tissue from longitudinal DCE-MRI were evaluated using AUC analysis on a prospective cohort of 273 TNBC patients.
Results: Four first order radiomic features were predictive of pCR with AUC>0.6. Multivariable radiomic models and BPE changes had AUC<0.6 for pCR prediction in TNBC undergoing NAST.
Impact: Radiomic features from fibroglandular tissue and background parenchymal enhancement changes in ipsilateral and contralateral breasts using DCE MRI during treatment of triple-negative breast cancer patients were evaluated as noninvasive biomarkers for prediction of pathologic complete response to neoadjuvant systemic therapy.
Introduction
Triple-negative breast cancer (TNBC) accounts for approximately 20% of all breast cancers and is an aggressive subtype with high risk of disease relapse and a lower overall survival1. Presurgical neoadjuvant systemic therapy (NAST) is standard of care in the treatment of TNBC with diverse response that currently lacks clinically available profiling strategies for response prediction2. Pathological complete response (pCR) to NAST is associated with excellent long-term outcomes. However, less than 50% of TNBC patients achieve pCR and remaining patients suffer from high toxicity of treatment with limited benefits3. Prior studies showed that tumoral radiomic features from DCE-MRI images could be predictive of NAST response in breast cancer patients4. BPE has been studied as an imaging biomarker for predicting NAST response5-8, with most of the work based on breast cancer of all molecular subtypes, with limited studies evaluating TNBC subtype9. In this study we are investigating if mean BPE changes and FGT radiomic features from the DCE-MRI of ipsilateral and contralateral breasts in patients with TNBC can serve as noninvasive imaging biomarker for prediction of treatment response (pCR vs non-pCR).Methods
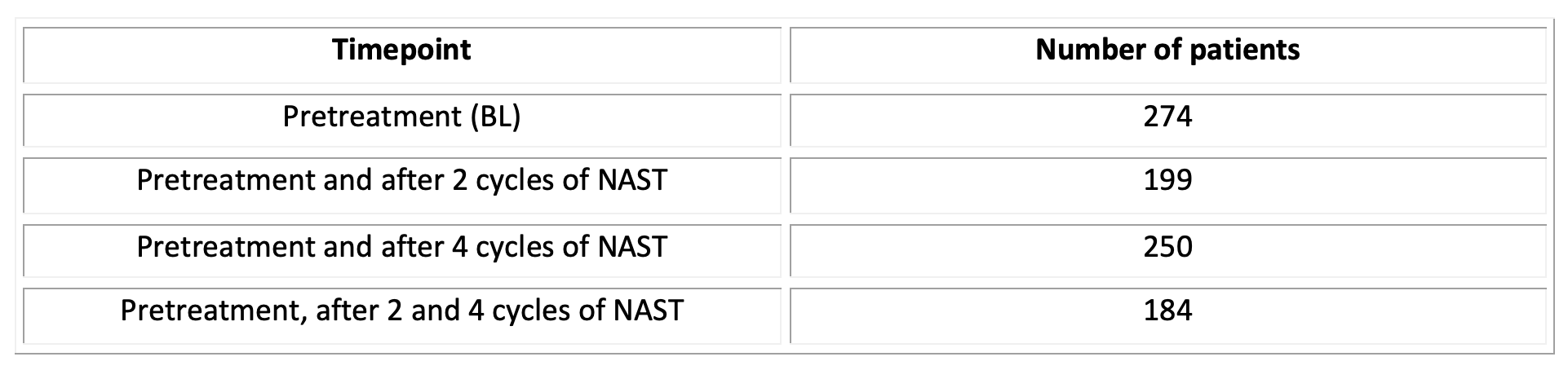
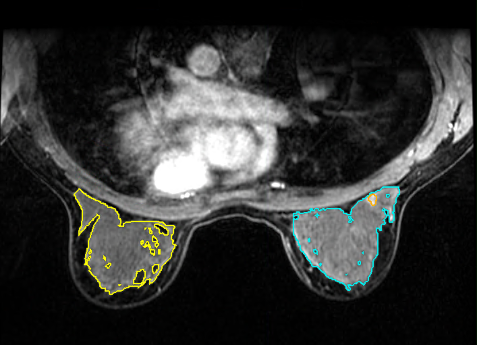
Datasets: We included 274 patients with stage I-III TNBC who were enrolled in an IRB approved prospective clinical trial (NCT02276433) and had longitudinal DCE MRI. The DCE series was scanned with the Differential Subsampling with Cartesian Ordering (DISCO) sequence on 3T whole-body scanners (GE Healthcare, Waukesha, WI, USA). The DCE images used were 2.5 minutes after contrast agent injection. Three MRI scans were acquired longitudinally; baseline (BL), after two cycles of NAST (C2), and after four cycles of NAST (C4). All patients had MRI prior to the initiation of NAST. The details of patients’ scans are listed in Table 1.Models: Three VOIs FGT of the normal breast side (contralateral), FGT of the affected breast side (ipsilateral) with exclusion of the tumor, and combined FGT of both breasts were semi-automatically segmented on the 2.5 minutes DCE images using MIM Maestro (MIM Software Inc. Cleveland, OH, USA) across the 3 different timepoints (Figure 1). Within each segmentation mask, mean BPE was calculated from DCE-MRI at each treatment time point according to the following formula5:$$BPE=\frac{1}{N}\times\sum_{i=1}^N(\frac{S_{1,i}-S_{0,i}}{S_{0,i}})$$where S0 is the precontract signal intensity, S1 is the postcontrast signal intensity of the image volume acquired at 2.5 minutes after contrast injection, and N is the number of included voxels. One hundred and seven radiomic features were extracted using Py-Radiomics10. Changes in BPE and radiomic features during treatment were compared between pCR and non-pCR using Wilcoxon Rank Sum test and Fisher’s exact test.
Statistics: The samples were split into training and testing data sets in a 2:1 ratio. Area under the receiver operating characteristics curve (AUC ROC) was used for univariable analysis for predicting pCR status. Logistic regression with elastic net regularization was performed for texture feature selection. Parameter optimization was performed by using 5-fold cross-validation based on mean cross-validated AUC in the training set.
Results and Discussion
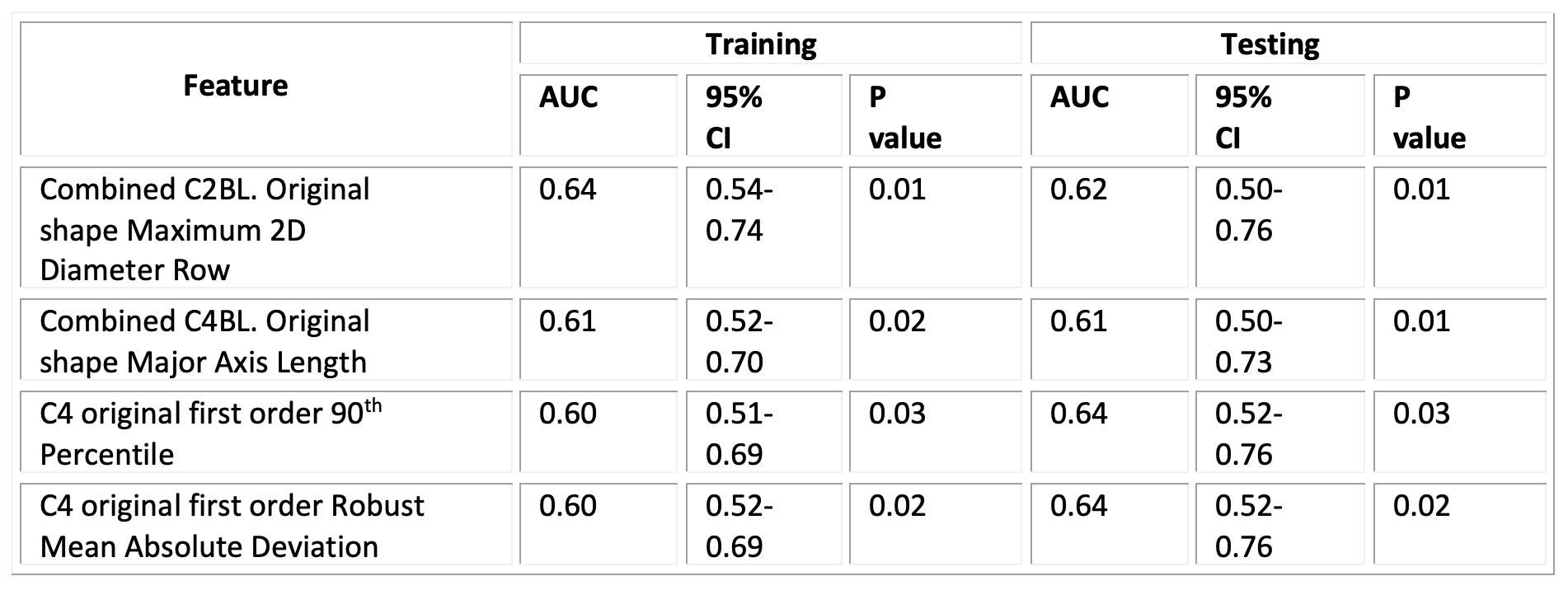
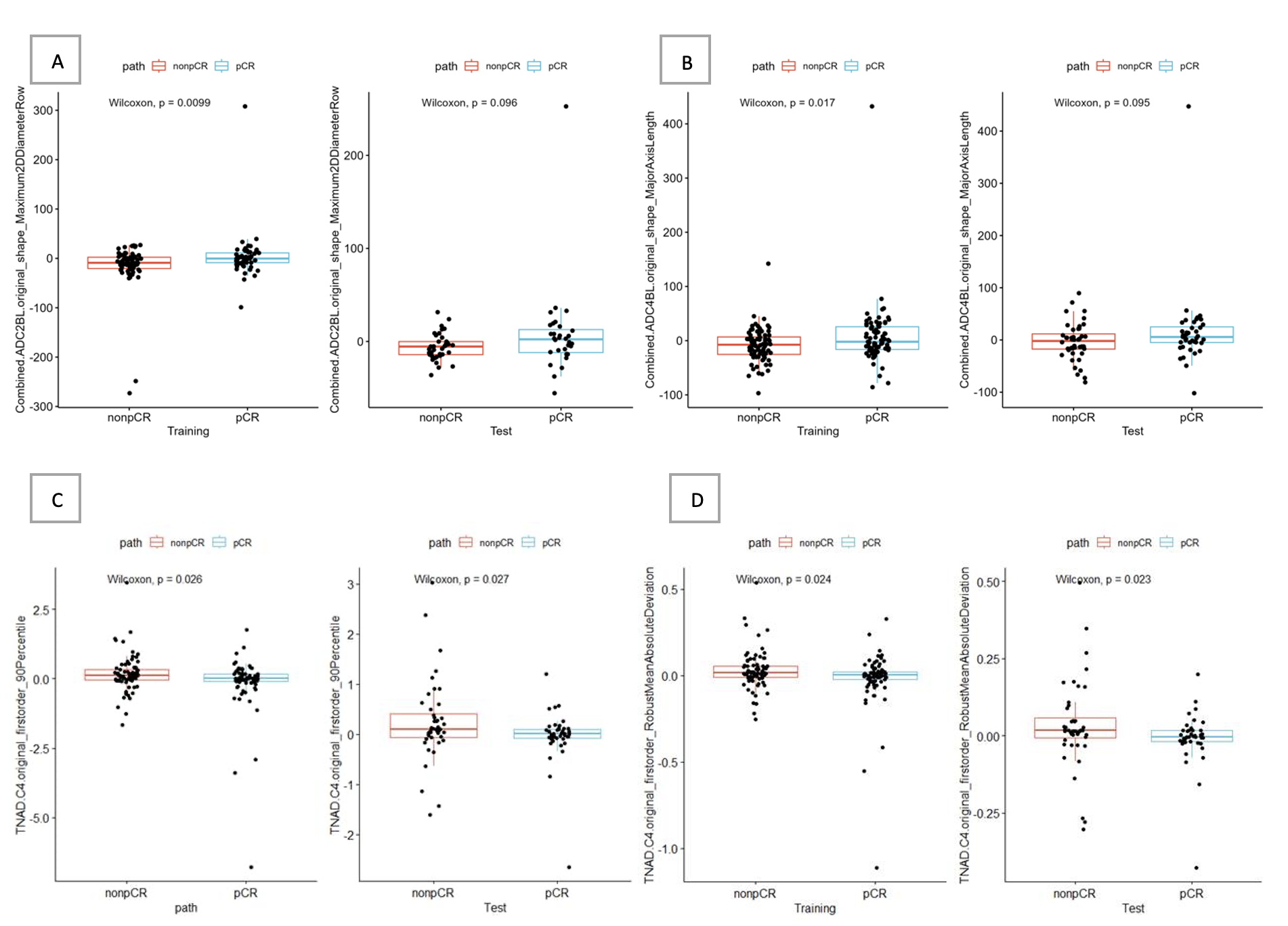
Of the total 274 patients, 130 (47%) had pCR and 144 (53%) had non-pCR. Using univariable analysis, two shape-based (2D) radiomic features of combined FGT from both breasts had AUC >0.6 in the testing set: from C4/BL (Major Axis Length) had AUC =0.61 and from C2/BL (Maximum 2D Diameter Row) had AUC =0.62 (Table 2 and Figure 2). Radiomic analysis of the feature difference between ipsilateral and contralateral FGT showed two first order radiomic features at C4 (90 percentile and Robust Mean Absolute Deviation) had AUC = 0.64 in the testing set (Table 2 and Figure 2). Multivariable models were not able to differentiate pCR versus non-pCR patients in both training and testing sets (AUC<0.6).Analysis of mean BPE and change of the mean BPE in ipsilateral and contralateral FGT at different time points during NAST demonstrated AUC <0.6 for pCR prediction. Analysis of mean BPE difference between ipsilateral and contralateral breasts also had AUC<0.6 for prediction of pCR.
Conclusion
Only four first order radiomics features from the FGT of both breasts were predictive of response to the NAST in TNBC. Neither multivariable radiomic models, nor mean BPE change were able to show significant difference between pCR and non-pCR TNBC patients. These findings suggest that FGT features and BPE changes may be hormone sensitive and not as useful for NAST response in TN molecular subtype of breast cancer. Future research for this subtype of breast cancer should be based on quantitative analysis of primary tumor as likely more useful biomarker of NAST response and evaluation of the possible additive role of the FGT for combined (tumor+FGT) models.Acknowledgements
This work was supported by the University of Texas MD Anderson Moon Shots Program and Robert D. Moreton Distinguished Chair Funds in Diagnostic Radiology. This study was supported by the NIH/NCI under award number P30CA016672.References
1. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938-1948.
2. Yao H, He G, Yan S, et al. Triple-negative breast cancer: is there a treatment on the horizon?. Oncotarget. 2017;8(1):1913-1924.
3. von Minckwitz G, Untch M, Blohmer JU, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30(15):1796-1804.
4. Panthi B, Adrada BE, Candelaria RP, Guirguis MS, Yam C, Boge M, Chen H, Hunt KK, Huo L, Hwang K-P, et al. Assessment of Response to Neoadjuvant Systemic Treatment in Triple-Negative Breast Cancer Using Functional Tumor Volumes from Longitudinal Dynamic Contrast-Enhanced MRI. Cancers. 2023; 15(4):1025.
5. Nguyen AA, Arasu VA, Strand F, et al. Comparison of Segmentation Methods in Assessing Background Parenchymal Enhancement as a Biomarker for Response to Neoadjuvant Therapy. Tomography. 2020;6(2):101-110.
6. Arasu VA, Kim P, Li W, et al. Predictive Value of Breast MRI Background Parenchymal Enhancement for Neoadjuvant Treatment Response among HER2- Patients. J Breast Imaging. 2020;2(4):352-360.
7. You C, Peng W, Zhi W, et al. Association Between Background Parenchymal Enhancement and Pathologic Complete Remission Throughout the Neoadjuvant Chemotherapy in Breast Cancer Patients. Transl Oncol. 2017;10(5):786-792.
8. Virostko J, Kuketz G, Higgins E, et al. The rate of breast fibroglandular enhancement during dynamic contrast-enhanced MRI reflects response to neoadjuvant therapy. Eur J Radiol. 2021;136:109534.
9. Xu C, Yu J, Wu F, et al. High-background parenchymal enhancement in the contralateral breast is an imaging biomarker for favorable prognosis in patients with triple-negative breast cancer treated with chemotherapy [published correction appears in Am J Transl Res. 2023 Jul 15;15(7):4970]. Am J Transl Res. 2021;13(5):4422-4436.
10. van Griethuysen JJM, Fedorov A, Parmar C, et al. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017;77(21):e104-e107.
Figures