1451
Clinical study on distinguishing Triple-Negative Breast Cancer from Non-Triple-Negative Breast Cancer using 3D-APT and DWI1Department of Radiology, Affiliated Hospital of Chengdu University, Chengdu, China, 2GE Healthcare, MR Research, Beijing, China
Synopsis
Keywords: Cancer, Breast, Triple-negative breast cancer; Non-triple-negative breast cancer; Amide proton transfer imaging; DWI
Motivation: Triple-negative breast cancer (TNBC) is a highly malignant and prognostically challenging subtype of breast cancer often elusive in conventional MRI scans [1.4.5]. Three-Dimensional Amide Proton Transfer Imaging (3D-APT), a non-invasive molecular imaging technique, shows promise in improving TNBC diagnosis.
Goal(s): This study aimed toinvestigate the diagnostic potential of 3D-APT, alone and in conjunction with diffusion-weighted imaging (DWI), in distinguishing TNBC from non-TNBC.
Approach: Quantitative analysis and comparison of APTw and DWI were conducted.
Results: Results revealed higher APTw and ADC values in TNBC compared to non-TNBC. Both APTw and DWI exhibit commendable diagnostic efficiency individually, while their combined application demonstrates superior discriminatory power.
Impact: These findings provide essential insights for tailoring individualized treatment strategies and assessing prognosis in clinical practice.
Introduction
Triple-negative breast cancer is a unique form of breast cancer characterized by the absence of estrogen receptors, progesterone receptors, and human epidermal growth factor receptor 2 (HER2) expression[1]. This type of cancer is highly aggressive, prone to recurrence, and associated with a poor prognosis.Distinct treatment approaches and prognoses differ between triple-negative breast cancer and other subtypes[2-3.6], making accurate identification of triple-negative breast cancer crucial for treatment decisions and prognosis assessment for patients. In recent years, advancementsin imaging techniques such as three-dimensional amide proton transfer (3D-APT) and diffusion-weighted imaging (DWI) has provided valuable insights in the diagnosis of breast cancer.However, in the current research, there are still aspects of its molecular subtyping that have not yet been explored.This study aims to investigate the potential application value of both 3D-APT and the combination of 3D-APT with DWI in accurately distinguishing between triple-negative breast cancer and non-triple-negative breast cancer.Methods
In this prospective study, a total of 53 cases confirmed as breast cancer by surgical resection or biopsy pathology between October 2022 and September 2023 were collected. The dataset was divided into TNBC and non-TNBC groups based on pathological results. All Magnetic resonance imaging (MRI) scan were performed on a 3.0T MRI scanner (Signa Premier, GE Healthcare, Milwaukee, USA) , including conventional MRI, dynamic contrast-enhanced imaging, three-dimensional amide proton transfer imaging (3D-APT), and diffusion-weighted imaging (DWI). Apparent diffusion coefficient (ADC) values and Magnetic transfer ratio asymmetry [MTRasym (3.5 ppm)] rate of the lesions were obtained from DWI and amide proton transfer-weighted imaging (APTWI). General clinical data, differences in ADC values, and MTRasym (3.5 ppm) between the two groups were analyzed. Receiver operating characteristic curve (ROC) analysis was utilized to compare and evaluate the diagnostic performance of 3D-APT, DWI, and their combined use.All quantitative parameters were obtained by using software(ITK-SNAP software, version 2.2.0; http://www.itksnap.org).Statistical analysis
The data were statistically analyzed using SPSS 26.0 (IBM, Armonk, New York, USA) and R language(Ver.4.3.2).Patients were categorized into either the triple-negative group or the non-triple-negative group based on histopathological results obtained from needle biopsies or surgical resections. Independent sample t-tests or Mann-Whitney U tests were assessed to assess the differences in age, APTw, and ADC values between the two groups.ROC curves were plotted for DWI and APTWI to differentiate between the triple-negative group and non-triple-negative group based on the pathological diagnosis. The areas under the curve (AUC) for DWI, APTw, and the combined diagnosis were compared using the DeLong test. The optimal cutoff values were determined based on the ROC curves, and the sensitivity and specificity for differentiating the triple-negative group and non-triple-negative group were evaluated using the McNemar test for DWI, APTw, and the combined diagnosis.Results
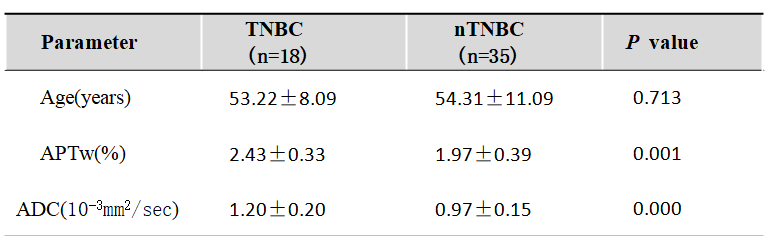
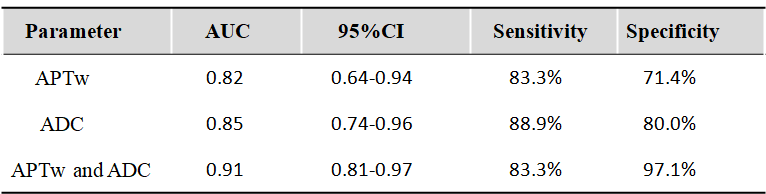
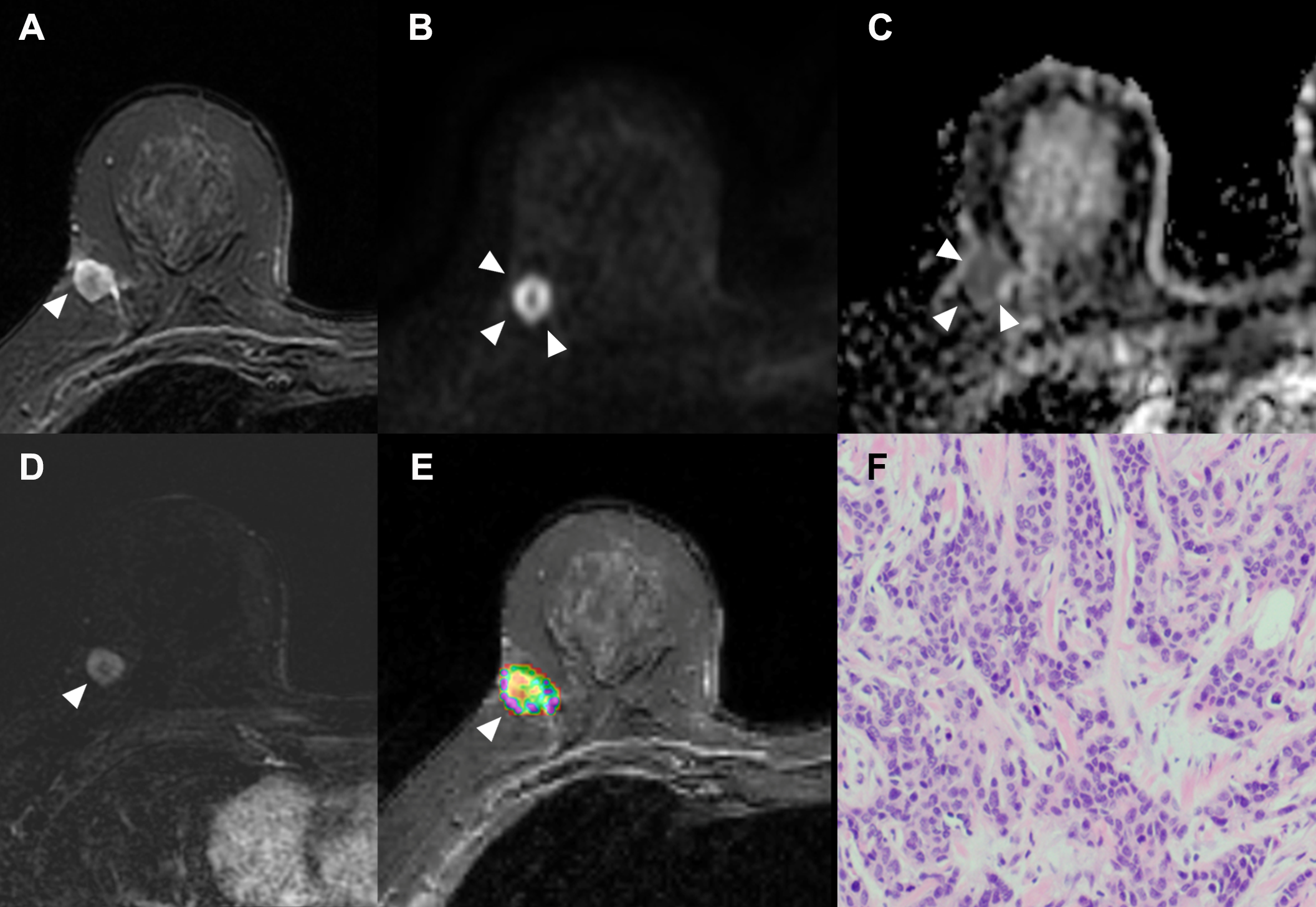
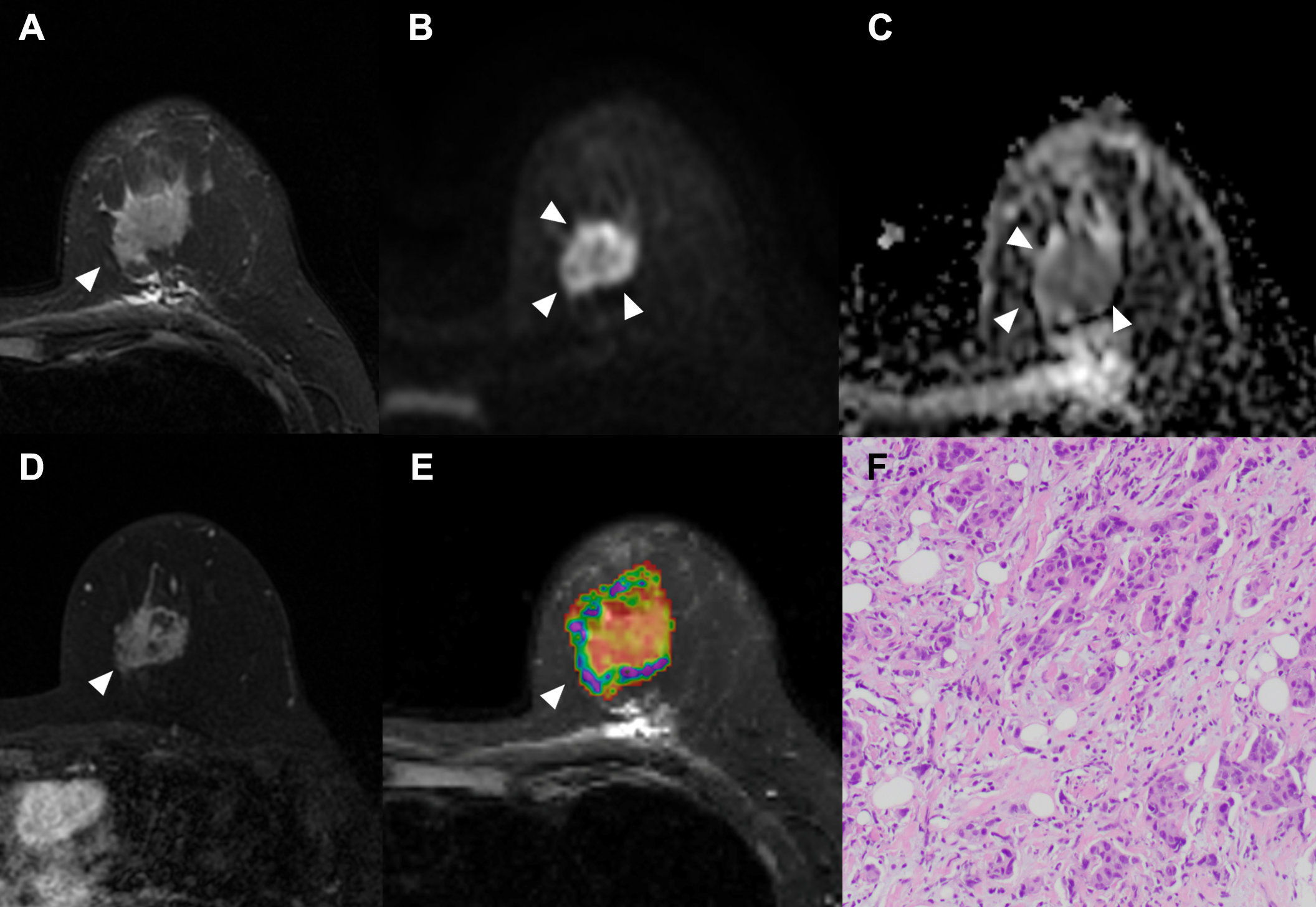
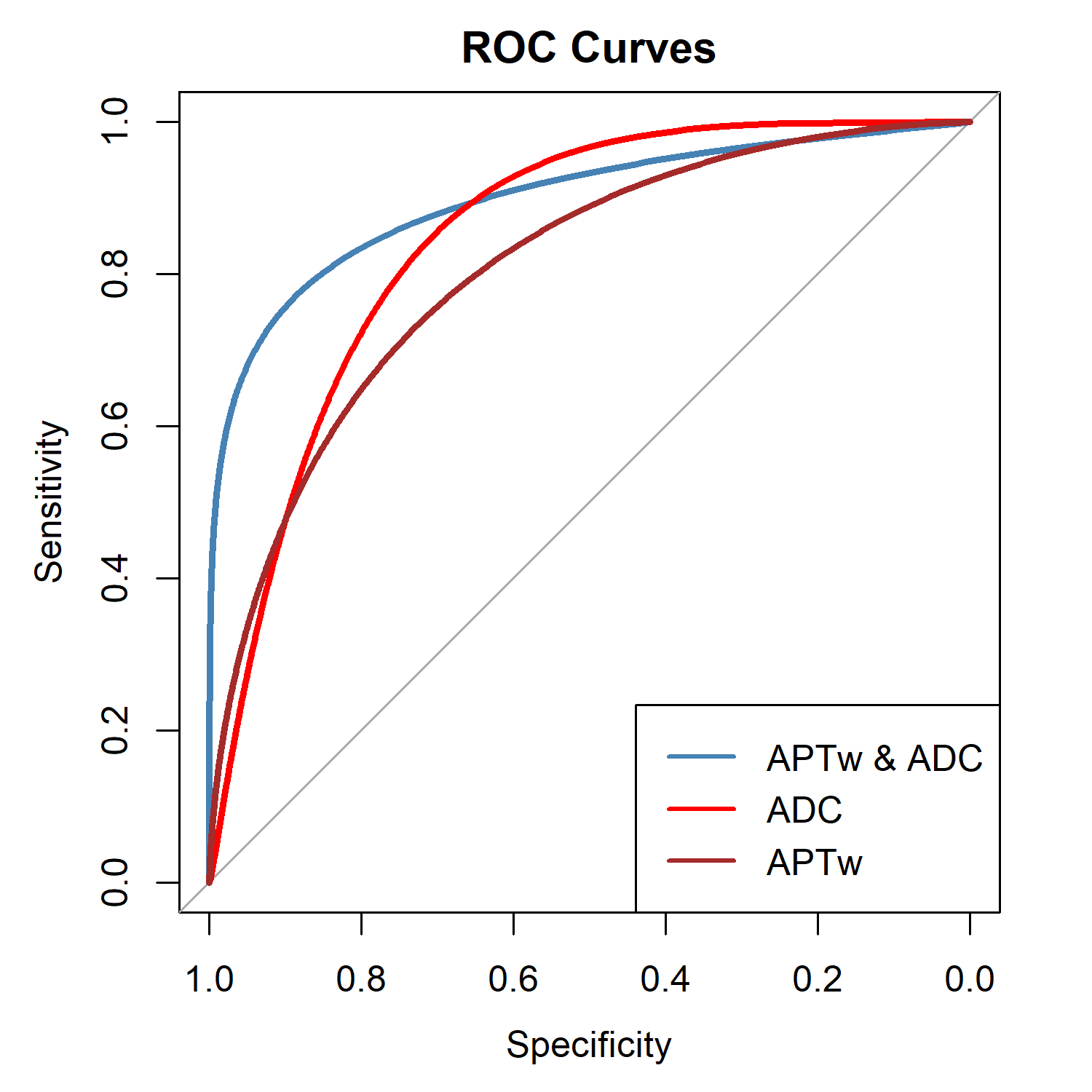
This study included 53 lesions from 53 patients with an average age of 51.0±13.1 years. Among them, 18 cases were TNBC, and 35 cases were non-TNBC. Key parameters for TNBC compared to non-TNBC were as follows: APTw values were (2.43±0.33)% and(1.97±0.37)%, with a statistically significant difference (P<0.05); ADC values were (1.20±0.20)×10-3mm2/sec and (0.97±0.15)×10-3mm2/sec, also showing a statistically significant difference (P<0.05), in Table1and Figure1-2. The areas under the ROC curves (AUC) for APTw and ADC in distinguishing between triple-negative and non-triple-negative breast cancer were 0.82 and 0.85, respectively, and there was no statistically significant difference between them(P=0.96). However, when APTw was combined with ADC, the AUC for the ROC curve increased to 0.91, which was relatively higher than APTw and ADC alone. This increase in AUC was statistically significant (P<0.05), as shown in Table2 and Figure 3.Discussion
The results of this study indicate that the combination of 3D-APT and DWI can serve as an effective imaging approach for distinguishing triple-negative breast cancer from non-triple-negative breast cancer. These findings hold significant importance in terms of enabling early diagnosis and guiding treatment decisionsfortriple-negative breast cancer, offering valuable insights for clinical practice.Conclusion
Three-dimensional amide proton transfer imaging (3D-APT) is beneficial in distinguishing between triple-negative breast cancer and non-triple-negative breast cancer. Furthermore, the combination of 3D-APT and DWI exhibits higher diagnostic performance, and when combined with DWI, it provides additional information. These findings hold significant value as a crucial point of reference for developing individualized treatment strategies and assessing prognosis in clinical practice.Acknowledgements
NoneReferences
1. Wang HJ, Cai Q, Huang YP, et al . Amide Proton Transfer-weighted MRI in Predicting Histologic Grade of Bladder Cancer. Radiology. 2022;305(1): 127-134.
2. Koike H, Morikawa M, Ishimaru H, et al. Amide Proton Transfer-Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review. Diagnostics (Basel). 2023; 28;13(5):914.
3.Togao O, Yoshiura T, Keupp J, et al. Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades. Neuro Oncol. 2014 ;16(3):441-448.
4. Kamitani T, Sagiyama K, Yamasaki Y, et al. Amide proton transfer (APT) imaging of breast cancers and its correlation with biological status. Clin Imaging. 2023;96:38-43.
5. Heo HY, Jones CK, Hua J, et al. Whole-brain amide proton transfer (APT) and nuclear overhauser enhancement (NOE) imaging in glioma patients using low-power steady-state pulsed chemical exchange saturation transfer (CEST) imaging at 7T. J MagnReson Imaging. 2016;44(1):41-50.
6. Kamimura K, Nakajo M, Yoneyama T, et al. Amide proton transfer imaging of tumors: theory, clinical applications, pitfalls, and future directions. Jpn J Radiol. 2019;37(2):109-116.
Figures